![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
186 Cards in this Set
- Front
- Back
|
What is the most common variant of R. hepatic artery? |
off SMA (20%) courses behind pancreas posterolateral to the common bile duct |
|
|
What is the most common variant of L. hepatic artery? |
Off left gastric artery (20%). Will find in gastrohepatic ligament medially |
|
|
What does the falciform ligament carry? |
the remnant of the umbilical vein in the ligamentum teres |
|
|
What does the ligamentum teres carry? |
the obliterated umbilical vein to the undersurface of the liver (extends from falciform) |
|
|
What is Cantlie's line? |
line drawn from middle of gallbladder fossa to IVC (separates right and left lobes) |
|
|
What are the anatomic divisions of the liver? |
Right anterior, posterior Left medial and lateral |
|
|
What are Couinaud's segments? |
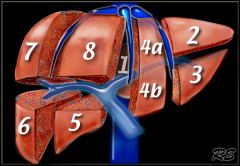
Segment 1 = caudate 2 = superior left lateral 3= inferior left lateral 4= left medial (a = superior, b =inferior) 5= inferior right anteromedial 6=inferior right posterolateral 7=superior right posterolateral 8= superior right anteromedial |
|
|
What is Glisson's capsule? |
peritoneum covering liver |
|
|
What is the bare area? |
spot not covered by Glissons capsule on the posterior-superior surface of liver |
|
|
What are the ligaments of the liver? |
Coronary ligaments on posterior surface, medial and lateral triangular ligaments |
|
|
What segments does the portal triad enter? |
4 and 5 |
|
|
Where on the livers does the gallbladder lie? |
segments 4 and 5 |
|
|
What is the relationship of the common duct, portal vein and the proper hepatic artery? |
portal vein is posterior, common duct is lateral and proper hepatic is medial |
|
|
What are Kupffer cells? |
liver macrophages |
|
|
What ligament contains the porta hepatis? |
the hepatoduodenal ligament |
|
|
What is the Pringle maneuver? |
clamping of the porta hepatis through the formen of winslow to stop bleeding. |
|
|
What type of bleeding will the pringle maneuver not stop? |
from the hepatic veins or posterior IVC |
|
|
What is the foramen of winslow? |
entrance to the lesser sac, posterior to the porta hepatis |
|
|
What are the boundaries of the foramen of Winslow? |
anterior: porta hepatis posterior : IVC superior : liver (caudate) inferior : duodenum |
|
|
What structures form the portal vein? |
splenic vein and the SMV (there are no valves) |
|
|
Where does the IMV empty? |
Splenic vein |
|
|
What percentage of O2 delivery is from the portal vein? |
about 65% (2/3rds) |
|
|
Which segments of the liver does the left portal vein supply ? |
II, III, IV |
|
|
Which segments of the liver does the right portal vein supply ? |
V, VI, VII, VIII |
|
|
Where does the middle hepatic artery originate? |
left hepatic artery |
|
|
What is the blood supply to most liver tumors? |
hepatic arteries |
|
|
What does the left hepatic vein drain? |
segments II, III, IVa |
|
|
What does the middle hepatic vein drain? |
segments IVb, V |
|
|
What does the right hepatic vein drain? |
segments VI, VII, VIII |
|
|
What is the most common variant of the middle hepatic vein? |
branches off left hepatic (80%) other 20% drains directly into IVC |
|
|
What do accessory hepatic veins do? |
drain medial aspect of the right lobe directly into IVC |
|
|
Where do the inferior phrenic veins drain? |
into IVC |
|
|
What is the blood supply to the caudate? |
receives separate right and left portal and arterial blood flow, separate hepatic veins drain directly into IVC |
|
|
Where is liver alkaline phosphatase stored? |
in canalicular membrane of hepatocytes |
|
|
Where in the hepatocyte does nutrient uptake occur? |
in the sinusoidal membrane |
|
|
What is the usual energy source for the liver? |
ketones (glucose stored as glycogen, excess glucose converted to fat) |
|
|
Where is urea synthesized? |
in the liver |
|
|
What blood clotting factors are NOT made in the liver |
factor 8 and von Willebrand factor (made in endothelium) |
|
|
What type of vitamin does the liver store? |
fat-soluble (also B12) |
|
|
Which hepatocytes are most sensitive to ischemia? |
the central lobular (acinar zone III) |
|
|
How much liver can be safely resected? |
75% a future liver remnant volume of 25% to 30% is considered adequate in a normal liver, especially if two contiguous Couinaud segments are preserved. Calculate with CT volumitry (divide part to be resected by total volume) If cirrhotic, must have 40-50% remnant |
|
|
What are the breakdown products of hemoglobin? |
-->heme-->biliverdin-->bilirubin |
|
|
What enzyme conjugates bile? |
glucuronyl transferase (occurs in liver bile-->glucuronic acid) improves solubility in water |
|
|
Where is urobilinogen made? |
breakdown of conjugated bilirubin by bacteria in the terminal ileum-->excreted in urine as urobilin excess urobilinogen makes urine very dark |
|
|
What are the components of bile? |
bile salts (85%), proteins, phospholipids, cholesterol, bilirubin |
|
|
How is water reabsorbed in the gallbladder? |
actively through Na/K ATPase |
|
|
What are bile salts? |
bile conjugated to taurine and glycine (improves water solubility) |
|
|
What are the primary bile acids? |
cholic and chenodoxycholic |
|
|
What are secondary bile acids? |
deoxycholic and lithocolic (dehydroxylated by bacteria in gut) |
|
|
What is the main biliary phospholipid? |
lecithin (emulsifies fat and solubilizes cholesterol)
|
|
|
What is the function of bile? |
solubilizes cholesterol and emulsifies fats so that they may be absorbed by the intestinal enterocytes |
|
|
At what bilirubin level does jaundice occur? |
>2.5 (see first under tongue) |
|
|
What is the maximum bilirubin (and what are the exceptions?) |
30 unless underlying renal dz, hemolysis, or bile duct hepatic vein fistula |
|
|
What causes elevated un-conjugated bilirubin (indirect)? |
pre-hepatic causes (hemolysis) hepatic deficiencies in uptake or conjugation |
|
|
What causes elevated conjugated bilirubin (direct)? |
secretion defects into bile ducts, excretion defects into GI tract (stones, stricture, tumor) |
|
|
What is Gilbert's disease? |
abnormal conjugation, mild defect in glucuronyl transferase |
|
|
What is Crigler-Najjar disease? |
inability to conjugate, severe enzymatic deficiency in glucuronyl transferase life threatening |
|
|
What is causes physiologic jaundice of the newborn? |
immature glucuronyl transferase, high unconjugated bili |
|
|
What is Rotors syndrome |
deficiency in storage ability, high conjugated bilirubin |
|
|
What is Dubin-Johnson syndrome? |
deficiency in secretion ability, high conjugated bili |
|
|
What infections can cause fulminant hepatic failure? |
hepatitis B, D, E (rare with A and C) |
|
|
What type of hepatitis can cause Hepatoma? |
hepatitis B, C, D |
|
|
What antibody is elevated in acute hepatitis B infection? |
Anti- HBc IgM x 6 months, then IgG |
|
|
What antibodies are in the blood after hepatitis B vaccination? |
Anti-HBs only |
|
|
What antibodies are in the blood after a previous hepatitis infection? |
Anti HBc and anti-HBs (no Hbs Antigen) |
|
|
What is the most common hepatitis that leads to liver transplant |
hepatitis C (long incubation period) |
|
|
What is hepatitis D? |
cofactor for hepatitis B that worsens prognosis |
|
|
What is hepatitis E? |
causes fulminant hepatic failure in pregnancy (often in 3rd trimester) |
|
|
What is the best indicator of hepatic function? |
prothrombin time |
|
|
What is the mortality rate for acute fulminant liver failure? |
80% (outcome determined by course of encephalopathy) |
|
|
What are the Kings College Criteria for urgent transplant in Tylenol induced acute liver failure? |
arterial pH <7.3 OR all of the following: INR >6.5, creatinine >3.4 mg/dL (300umol/L), grade III/IV encephalopathy |
|
|
What are the Kings College Criteria for urgent transplant in non-Tylenol induced acute liver failure? |
INR > 6.5 OR any three of the following Age<10 or >40, drug toxicity or undetermined etiology, jaundice > 7 days before encephalopathy , INR >3.5 , bilirubin >17 mg/dL |
|
|
other causes of encephalopathy besides liver failure? |
GI bleeding, infection (SBP), electrolyte imbalances, drugs |
|
|
What is the treatment for hepatic encephalopathy ? |
lactulose (cathartic)- acidifies colon and remove bacteria, blocks NH3 uptake. 2-3 stools per day limit protein intake (<70g/day) Branched chain amino acids- metabolized by skeletal muscle No antibiotics unless specifically have infection Neomycin (gets rid of ammonia producing bacteria from gut) |
|
|
Mechanism for ascites |
hepatocyte destruction--> fibrosis and scarring-->increased hepatic pressure-->portal venous congestion-->lymphatic overload-->leakage of splanchnic and hepatic lymph into peritoneum --> ascites |
|
|
What must you do after paracentesis for ascites? |
replace with albumin 1g for every 100cc removed |
|
|
What is the treatment for ascites |
water restriction (1-1.5L/day) low NaCl (1-2g/day) diuretics (spironolactone) paracentesis, TIPS prophylactic antibiotics to prevent SBP (norfloxacin-used if previous SBP or current UGI bleed) |
|
|
Why is aldosterone elevated in liver failure |
due to impaired hepatic metabolism and impaired GFR |
|
|
What is hepatorenal syndrome? |
prerenal azotemia due to liver failure. blood vessels in the kidney circulation are constricted because of the dilation of blood vessels in the splanchnic circulation(which supplies the intestines), which is mediated by factors released by liver disease (NO, prostaglandins). The consequence of this phenomenon is a decrease in the "effective" volume of blood sensed by the juxtaglomerular apparatus, leading to the secretion of renin and the activation of the renin-angiotensinsystem high ADH |
|
|
What is the treatment for hepatorenal syndrome |
stop diuretics, give volume, midodrine, octreotide, no good therapy other than liver transplant |
|
|
What causes postpartum liver failure with ascites? |
Hepatic vein thrombosis from ovarian vein, often has an infectious component (pelvic thrombophlebitis) Dx with SMA arteriogram with venous contrast Tx: heparin and antibiotics |
|
|
What is spontaneous bacterial peritonitis? |
fever, abd pain, PMNs in ascites >250 prolonged bacteremia secondary to compromised host defenses, intrahepatic shunting of colonized blood, and defective bactericidal activity within the ascitic fluid |
|
|
What is the most common pathogen in SBP? |
E.coli (then pneumococci and streptococci ) usually a single organism |
|
|
If patient with SBP has multiple organisms growing what should you be concerned about? |
bowel perforation |
|
|
What are the risk factors for SBP? |
prior SBP, UGI bleeding (variceal hemorrhage), low protein ascites |
|
|
What antibiotic is used for the treatment of SBP? |
3rd generation cephalosporin (usually see response in 48hrs) |
|
|
What is the treatment for esophageal varices? |
banding and sclerotherapy (95% effective) |
|
|
What medications can temporize variceal bleeding |
vasopressin (splanchnic a vasoconstriction), octreotide (decreased portal pressure -->lower blood flow) |
|
|
In patients with a history of CAD, what should you give when treating esophageal varices with vasopressin |
nitroglycerin |
|
|
What drug can you give for prophylaxis for esophageal varices? |
propranolol (no role in acute bleed) |
|
|
What procedure is performed for refractory variceal bleeding (even in emergency setting)? |
TIPS |
|
|
What are the 3 types of portal HTN |
1. pre-sinusoidal : schistasomiasis, congenital hepatic fibrosis, portal vein thrombosis (kids) 2. sinusoidal: cirrhosis 3. post-sinusoidal: Budd-Chiari, constrictive pericarditis, CHF |
|
|
What is the normal portal vein pressure? |
< 10-12 mmHg |
|
|
What veins act as collaterals between the portal vein and the systemic system (azygous)? |
coronary veins |
|
|
What is a TIPS procedure? |
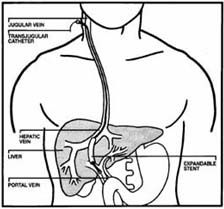
Transjugular intraheptic portosystemic shunt. Connects hepatic veins to portal veins |
|
|
What are the indications for a TIPS procedure? |
protracted bleeding, progression of coagulopathy, visceral hypoperfusion, or refractory ascites, hepatic pleural effusion allows antegrade flow from portal vein to IVC |
|
|
What is a complication of TIPS |
development of encephalopathy |
|
|
What is a splenorenal shunt (Warren shunt)? |
surgical procedure in which the distalsplenic vein (a part of the portal venous system) is attached to the left renal vein. must ligate the left adrenal vein, left gonadal vein, inferior mesenteric vein, coronary vein, pancreatic branches of the the splenic vein |
|
|
What has a lower rate of encephalopathy, TIPS or splenorenal shunt? |
splenorenal shunt (also do not need splenectomy) |
|
|
What are the indications for splenorenal shunt? |
Child A cirrhosis with bleeding |
|
|
What are the contraindications for splenorenal shunt? |
refractory ascites (can worsen ascites) |
|
|
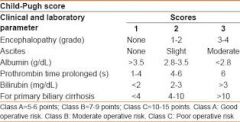
What is the Child Pugh Score? |
Calculates mortality in cirrhosis determine the prognosis, as well as the required strength of treatment and the necessity of liver transplantation. |
|
|
What is the scoring system of the Child Pugh System? |
|
|
|
What is the mortality of Child's A cirrhosis with a shunt? |
2% |
|
|
What is the mortality of Child's B cirrhosis with a shunt? |
10% mortality |
|
|
What is the mortality of Child's C cirrhosis with a shunt? |
50% mortality |
|
|
What is the most common cause of massive hematemesis in children? |
portal HTN caused by extra-hepatic portal vein thrombosis |
|
|
What is Budd Chiari syndrome? |
occlusion of hepatic veins or IVC (RUQ pain, hepatosplenomegaly, ascites, fulminant hepatic failure, muscle wasting, variceal bleeding) |
|
|
What are the causes of Budd Chiari Syndrome? |
Hepatic vein thrombosis due to: 1 Polycythemia vera (most common) 2 Pregnancy/Postpartum state 3 Use of oral contraceptives 4 Paroxysmal nocturnal hemoglobinuria 5 Hepatocellular carcinoma 6 Lupus anticoagulants |
|
|
How do you diagnose Budd Chiari? |
duplex US first angiogram with venous phase CT angio liver bx shows sinusoidal dilatation, congestion, centrilobular congestion |
|
|
What is the treatment for Budd Chiari ? |
portocaval shunt (connect to IVC above obstruction) if liver disease reversible. If acute can try catheter directed tPA If not reversible and chronic do liver transplant |
|
|
What are the symptoms of splenic vein thrombosis ? |
gastric varices that may bleed, often caused by pancreatitis |
|
|
What is the treatment for symptomatic splenic vein thrombosis ? |
splenectomy |
|
|
What side of the liver are amebic abscesses usually found? |
Right (usually solitary), from a colon infection that travels to liver from portal vein |
|
|
What are the risk factors for amebic abscesses? |
travel to Mexico, ETOH, fecal-oral |
|
|
What are the symptoms of amebic liver abscess |
fever, chills, RUQ pain, elevated WBC, jaundice, hepatomegaly |
|
|
How do you diagnose amebic liver abscess? |
serology for entamoeba hystolytica CT scan Culture of abscess usually sterile (protozoa often only in the peripheral rim) |
|
|
What is the treatment for amoebic liver abscesses? |
flagyl. Only aspirate if refractory. surgery if ruptures |
|
|
How do you diagnose echinoccocal cyst disease? |
positive casoni skin test, positive serology Sheep are carriers and dogs spread to humans (more common in right lobe of liver) |
|
|
What side of the liver are echinococcal cysts found? |
right side (calcified, double walled cyst) |
|
|
When do you perform an ERCP in echinococcal cyst disease? |
jaundice, increased LFTs, cholangitis. rule out communication with biliary system |
|
|
What is the treatment for echinoccocal cyst disease? |
pre-op albendazole (x 2 weeks), surgical removal (inject with alcohol) remove all of cyst wall (spilling can cause anaphylaxis) |
|
|
What are the symptoms of schistosomiasis? |
maculopapular rash, increased eosinophils, can cause variceal bleeding |
|
|
What is the primary infection site for schistosomiasis? |
sigmoid colon (fine granulation tissue, petechiae, ulcers) |
|
|
Treatment for schistosomiasis |
praziquantel and control of variceal bleeding |
|
|
What are the most common liver abscesses? |
pyogenic abscess (80%) |
|
|
What is the mortality associated with sepsis from pyogenic abscesses? |
15% |
|
|
What is the most common organism associated with pyogenic liver abscess? |
E coli (contiguous infection from biliary system), GNRs |
|
|
What is the second most common cause of pyogenic liver abscesses? |
bacteremia from other infections (diverticulitis, appendicitis, Crohns) |
|
|
What is the treatment for pyogenic liver abscesses? |
CT guided drainage, antibiotics surgery if unstable and continued sepsis |
|
|
What are risk factors for hepatic adenomas? |
women, steroid use, OCPs |
|
|
What is the risk of bleeding for hepatic adenoma |
20% |
|
|
What lobe of the liver are hepatic adenoma most common? |
right lobe |
|
|
How do you diagnose hepatic adenoma? |
No uptake on sulfur colloid scan (no Kupffer cells in adenoma)= cold Hypervascular tumor on MRI (well circumscribed lesion with bright peripheral enhancement) |
|
|
What is the treatment for hepatic adenoma |
If asymptomatic and less than 4cm, stop OCPs. If regresses, no further therapy If symptomatic or >4cm perform tumor resection or embolization if multiple |
|
|
How do you diagnose focal nodular hyperplasia |
CT shows central stellate scar, will take up sulfur colloid on liver scan, CT/MRI shows hypervascular tumor |
|
|
What is the treatment for FNH? |
Conservative treatment, no resection (no malignancy or rupture risk) |
|
|
How do you diagnose a hepatic hemangioma? |
MRI/CT scan shows peripheral to central enhancement (hypervascular) No biopsy as risk of hemorrhage |
|
|
What is the treatment for hepatic hemangioma |
conservative unless symptomatic then do surgery +/- embolization If unresectable can treat with steroids, XRT |
|
|
What is Kasabach-Merritt syndrome |
consumptive coagulopathy due to a hemangioma |
|
|
How much more common are metastatic malignant liver lesions than primary? |
about 20x more common |
|
|
What is the most common cancer worldwide? |
hepatocellular carcinoma |
|
|
What are the risk factors for HCC? |
Hep B (most common worldwide) HepC EtOH Hemochromatosis alpha 1 antitrypsin deficiency primary sclerosing cholangitis aflatoxins hepatic adenoma steroids pesticides Wilsons disease and primary biliary cirrhosis are NOT risk factors |
|
|
which types of HCC have the best prognosis? |
fibrolamellar Clear cell, lymphocyte infiltrative, |
|
|
What lab can you measure that correlates with the size of HCC tumors? |
AFP |
|
|
What is the 5 year survival for HCC after resection? |
30% (only 15% resectable due to cirrhosis, portohepatic LN involvement or metastases) |
|
|
What are the margins for HCC resection? |
1 cm |
|
|
Where is tumor recurrence most likely after liver resection? |
the liver |
|
|
What are risk factors for hepatic sarcoma |
PVC, thorotrast, arsenic rapidly fatal |
|
|
What is the 5 year survival for resection of solitary colonic liver mets? |
35% |
|
|
What is the vascularity of metastatic liver disease |
hypovascular low attenuation lesion on CT scan (vs hypervascular primary liver tumors) |
|
|
What is the appearance of HCC on imaging? |
heterogeneous, poorly circumscribed mass with bright arterial enhancement and quick washout |
|
|
What are the component of the MELD score |
It was initially developed to predict mortality within three months of surgery in patients who had undergone a transjugular intrahepatic portosystemic shunt (TIPS) procedure,[1] and was subsequently found to be useful in determining prognosis and prioritizing for receipt of a liver transplant. MELD = 3.78×ln[serum bilirubin (mg/dL)] + 11.2×ln[INR] + 9.57×ln[serum creatinine (mg/dL)] + 6.43 |
|
|
What are the Milan criteria? |
How to select a HCC patient for liver transplant 1. one lesion smaller than 5 cm 2. up to 3 lesions smaller than 3 cm 3. no extrahepatic manifestations 4. no vascular invasion |
|
|
What is considered a major hepatectomy? |
resection of greater than 3 segments |
|
|
What Child classification should not undergo liver resection? |
Class C (class B should only undergo a minor resection) |
|
|
What indocyanine green (ICG) retention at 15 mins is considered too high or hepatic resection |
ICGR-15 greater than 14% |
|
|
What platelet count is considered a contraindication to liver resection? |
<100,000 |
|
|
What are some risk factors for diminished survival in a patient with metastatic liver dz that has been resected? |
(a) node-positive primary tumor (b) disease-free interval less than 12 months (c) multiple liver metastases (d) largest hepatic metastasis greater than 5 cm (e) serum CEA level greater than 200 ng/mL. |
|
|
What is the duration of antibiotics for pyogenic liver absces? |
intravenous antibiotics are usually administered for 14 days, followed by oral agents for a total of 6 weeks |
|
|
What is the anatomy of a hydatid cyst? |
three layers: an outer thick fibrous pericyst, a thick middle hyaline layer or ectocyst, and an internal germinal layer or endocyst |
|
|
where in the liver can you not perform RFA |
hilar plate (bile duct wont tolerate) |
|
|
Management of Budd Chiari |
Focal obstruction of hepatic veins (web) : thrombolysis, angioplasty In patients with reversible liver damage and a patent IVC, portosystemic shunting is highly effective in controlling ascites and preserving hepatic function; clinical symptoms are relieved in 85% of such patients over 4 years. The placement of a transjugular intrahepatic portosystemic shunt (TIPS) can also be effective, but few data are available concerning long-term results. A mesoatrial shunt should be considered if BCS is complicated by IVC obstruction. Liver transplantation is advisable for patients with irreversible liver decompensation and is associated with a long-term survival of 65% to 85%. |
|
|
What is the cure rate for Sovaldi in hepatitis C? |
sofosbuvir= ant-viral medication 95% cure rate |
|
|
What is hepatic encephalopathy? |
liver failure --> inability to metabolize (buildup of ammonia, mercantanes, false neurotransmitters) |
|
|
complication of sclerotherapy for esophageal varices? |
strictures (can dilate endoscopically) |
|
|
Most common location of portal vein thrombosis? |
extra hepatic |
|
|
Sign of portal vein thrombosis? |
ascites without liver failure esophageal varices |
|
|
Treatment for portal vein thrombosis |
heparin if acute (do not give if UGI bleeding is present) may need a shunt eventually |
|
|
What proportion of hepatic adenomas are symptomatic? |
80% |
|
|
What proportion of hepatic adenomas are at risk of rupture? |
50% |
|
|
What proportion of hepatic adenomas are at risk of becoming malignant? |
5% |
|
|
What is the most common benign hepatic tumor? |
hemangioma (usually asymptomatic and rarely rupture) |
|
|
Best test for hepatic hemangioma? |
tagged RBC scan |
|
|
Treatment for solitary liver cysts? |
usually can leave alone |
|
|
Histologic subtype of HCC with worst prognosis? |
diffuse nodular |
|
|
Most important determinant of long term survival in HCC? |
vascular invasion (NOT nodal status) |
|
|
Mortality of operating on a spontaneously ruptured HCC? |
40% preferred to treat with packing, hepatic artery ligation, and transarterial embolization |
|
|
How can you measure portal venous pressure? |
hepatic wedge pressure |
|
|
marker for diving right and left hepatectomy? |
middle hepatic vein |
|
|
how are right anterior and posterior segments of liver divided? |
right portal vein |
|
|
how are left medial and lateral segments of liver divided? |
round ligament at umbilical fissure |
|
|
Types of eccinococcal cysts? |
Echinococcus granulosus (cysts), E. multilocularis (portal HTN, cholangitis) , and E. vogeli (cysts) |
|
|
Most common cause of pyogenic liver abscess? |
cholangitis (manipulation of biliary tree) |
|
|
During left hepatectomy what do you divide first? last? |
L hepatic artery last is L portal vein |
|
|
risk of seroconversion after HCV exposure? |
1.8% |