![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
37 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
HEADINGS |
01. DEf 02. Epid
|
|
|
|
01. Def
|
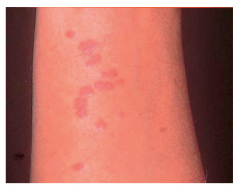
an eruption of shiny flat-topped purplish (usually itchy) papules on the wrist andforearms and thighs.
Lichen planus is a pruritic inflammatory dermatosis that is commonly associated with mucosal involvement and rarely with nail dystrophy and scarring alopecia Definition Lichen planus is a skin condition of unknown origin that produces small, shiny, flat-topped, itchy pink or purple raised spots on the wrists,forearms or lower legs, especially in middle-aged patients. |
|
|
|
02. Epid |
Lichen planus occurs worldwide; |
|
|
|
Sex, age |
Lichen planus occurs in both sexes and at any age, |
|
|
|
03. Etiology The cause is unknown; . . |
01. Viral Triger 02. Autoimune 03. Genetic HLA Associated 04. Immune reaction |
|
|
|
01. a viral trigger was considered |
but has not been substantiated |
|
|
|
02. An autoimmune pathogenesis is suspected, why? |
as there is an association with ii. primary biliary cirrhosis, iv. hepatitis B and C, v. alopecia areata, vii. and thymoma, and there are The cause is unknown but is possibly a T-cell-driven |
1. Associations 2. Similarities |
|
|
03. Immune reaction |
An immune reaction to unknown antigen is |
|
|
|
04. HLA association |
Lichen planus can occasionally occur in families and possible HLA associations have been proposed, |
|
|
|
03. Pathogenesis |
There ii. basal cell degeneration and a iii. heavy, bandlike T-lymphocyte infiltrate in the papillary dermis, with affinity for the epidermis (epidermotropism). Hyperkeratosis with thickening of the granular cell layer is |
(epidermotropism)? |
|
|
04. Clinical features |
it typically presents as |
The rash is characterized by small, purple flat-topped, polygonal papules that are intensely pruritic (Fig. 24.19). It is |
|
|
History drug History |
A careful drug history must be taken as, although |
e.g. beta-blockers, gold, levamisole, ACE inhibitors or antimalarials |
|
|
loc |
It generally |
|
|
|
char |
It is intensely itchy and lesions are violaceous, shiny, flat-topped, polygonal papules, |
(Wickham’s striae). |
|
|
ass with trauma |
New lesions may appear at |
(Köbner phenomenon) |
|
|
duration Aggra |
. Individual lesions may |
|
|
|
Remission Chronicity |
The eruption usually remits over months, but can |
|
|
|
Pst inf Hyp |
Post-inflammatory pigmentary change is common, |
|
|
|
Inv of Muc memb |
Mucous membrane |
|
|
|
Signif |
These oral changes are often asymptomatic and should be sought on examination. |
|
|
|
other muc |
Genital and other mucosal surfaces can also be affected |
|
|
|
Nail inv |
Nail involvement occurs in about |
|
|
|
Scalp |
Scalp involvement usually presents as an inflammatory scarring alopecia, often with tufting of residual hairs. |
|
|
|
dds |
The classical presentation of lichen planus |
|
|
|
other dds |
Other differential diagnoses include psoriasis, pityriasis rosea, pity riasis |
|
|
|
04. investigation |
A skin biopsy should be performed if there is diagnostic |
|
|
|
Screening |
. Screening |
|
|
|
Duartion of cond |
The condition is usually self-limiting, although rarely, |
|
|
|
05. Treatment 01. |
Treatment is symptomatic and potent local corticosteroids (topical, with occlusion or by injection for |
This requires the use of potent topical steroids (0.05% |
|
|
02. Photother |
. UVB, PUVA or UVA1 can be beneficial |
|
|
|
and, for recalcitrant disease, |
retinoids or immunosuppressants such as ciclosporin may be needed. |
|
|
|
06. Prognosis |
A low but |
The condition often clears by 18 months but can recur at |
|
|
Lichen Planus
Description Lichen planus affects between 1-2% of the population, most of whom are middle-aged women. The condition is less common in the veryyoung and the very old. The lesions are found on the skin, genitals, and in the mouth. Most cases resolve spontaneously within two years.Lichen planus is found throughout the world and is equally distributed among races. Causes and symptoms No one knows what causes lichen planus, although some experts suspect that it is an abnormal immune reaction following a viral infection,probably aggravated by stress. The condition is similar to symptoms caused by exposure to arsenic, bismuth, gold, or developers used incolor photography. Occasionally, lichen planus in the mouth appears to be an allergic reaction to medications, filling material, dentalhygiene products, chewing gum or candy. Symptoms can appear suddenly, or they may gradually develop, usually on the arms or legs. The lesions on the skin may be preceded bya dryness and metallic taste or burning in the mouth. Once the lesions appear, they change over time into flat, glistening, purple lesions marked with white lines or spots. Mild to severe itchingis common. White, lacy lesions are usually painless, but eroded lesions often burn and can be painful. As the lesions clear up, they usuallyleave a brown discoloration behind, especially in dark skinned people. Lichen planus in the mouth occurs in six different forms with a variety of symptoms, appearing as lacy-white streaks, white plaques, oreroded ulcers. Often the gums are affected, so that the surface of the gum peels off, leaving the gums red and raw. Diagnosis A doctor can probably diagnose the condition simply from looking at the characteristic lesions, but a skin biopsy may be needed to confirmthe diagnosis. Treatment Treatment is aimed at easing symptoms. Itching can be treated with steroid creams and oral antihistamines. Severe lesions can be treatedwith corticosteroids by mouth, or combinations of photochemotherapy (PUVA) and griseofulvin. Patients with lesions in the mouth may find that regular professional cleaning of the teeth and conscientious dental care improve thecondition. Using milder toothpastes instead of tartar control products also seems to lessen the number of ulcers and makes them lesssensitive. Prognosis While lichen planus can be annoying, it is usually fairly benign and clears up on its own. It may take months to reach its peak, but itusually clears up within 18 months. Key terms PUVA — A type of phototherapy that combines the oral or topical photosensitizing chemical psoralen, plus long-wave ultraviolet light-A(UVA). Resources Other Lichen Planus Self-Help. Baylor College of Dentistry. http://www.tambcd.edu/lichen. Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved. lichen /li·chen/ (līk´'n) 1. any of certain plants formed by the mutualistic combination of an alga and a fungus. 2. any of various papular skin diseases in which the lesions are typically small, firm papules set close together. lichen amyloido´sus a condition characterized by localized cutaneous amyloidosis. lichen fibromucinoido´sus , lichen myxedemato´sus a condition resembling myxedema but unassociated with hypothyroidism, markedby a fibrocystic proliferation, increased deposition of acid mucopolysaccharides in the skin, and the presence of a circulating paraprotein; itmay present as lichenoid papules or urticaria-like plaques and nodules. lichen ni´tidus a chronic inflammatory eruption consisting of many, pinhead-sized pale, flat, sharply marginated, glistening, discretepapules, scarcely raised above the skin level. lichen planopila´ris a variant of lichen planus characterized by formation of acuminate horny papules around the hair follicles, in additionto the typical lesions of ordinary lichen planus. lichen pla´nus an inflammatory skin disease with wide, flat, violaceous, shiny papules in circumscribed patches; it may involve the hairfollicles, nails, and buccal mucosa. lichen ru´ber monilifor´mis a variant of lichen simplex chronicus with papules arranged in linear beaded bands. lichen ru´ber pla´nus l. planus. lichen sclero´sus a chronic atrophic skin disease marked by white papules with an erythematous halo and keratotic plugging, usuallyaround the external genitalia or in the perianal region. lichen scrofuloso´rum , lichen scrofulo´sus any eruption of minute reddish lichenoid follicular papules in children and young adults withtuberculosis. lichen sim´plex chro´nicus a dermatosis of psychogenic origin, marked by a pruritic discrete or, more often, confluent papular eruption,usually confined to a localized area. lichen spinulo´sus a condition in which there is a horn or spine in the center of each hair follicle. lichen stria´tus a self-limited condition characterized by a linear lichenoid eruption, usually in children. Dorland's Medical Dictionary for Health Consumers. © 2007 by Saunders, an imprint of Elsevier, Inc. All rights reserved. lichen pla·nus (plns)n. A skin condition characterized by the eruption of flat-topped, shiny, violaceous papules on flexor surfaces, male genitalia, and themucosa of the oral cavity. Also called lichen ruber planus. The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company. Published by Houghton Mifflin Company. All rights reserved. lichen planus, a nonmalignant, chronic, pruritic skin disease of unknown cause that is characterized by small flat purplish polygonal papules or plaqueswith fine gray lines on the surface. Common sites are flexor surfaces of wrists, forearms, ankles, abdomen, sacrum, and genitalia. Onmucous membranes the lesions appear gray and lacy. Nails may have longitudinal ridges. Episodes of disease activity vary but may last formonths and may recur. Treatment with topical corticosteroids is common. Mosby's Medical Dictionary, 8th edition. © 2009, Elsevier. lichen planus lichen planus A pruritic dermopathy of flexor surfaces (especially wrist), orogenital mucosa, hands, feet, lower back, and thepretibial area, which is characterised by papular thickening of upper dermis, and a shiny violaceous surface. DiffDx Lichenoid drug reaction, lichenoid keratosis, granuloma annulare, systemic lupus eythematosus, psoriasis. Management Corticosteroids. Segen's Medical Dictionary. © 2012 Farlex, Inc. All rights reserved. lichen [li´ken] 1. any of certain plants formed by the mutualistic combination of an alga and a fungus. 2. any of various papular skin diseases in which the lesions are typically small, firm papules set very close together. lichen amyloido´sus a condition characterized by localized cutaneous amyloidosis. lichen fibromucinoido´sus (lichen myxedemato´sus) a condition resembling myxedema but unassociated with hypothyroidism, markedby mucinosis and a widespread eruption of asymptomatic, soft, pale red or yellowish, discrete papules. lichen ni´tidus a usually asymptomatic chronic inflammatory eruption consisting of numerous glistening, flat-topped, discrete, smooth,commonly skin-colored micropapules, located most often on the penis, lower abdomen, inner thighs, flexor aspects of the wrists andforearms, breasts, and buttocks. Widespread involvement may produce confluence of the lesions, with formation of scaly plaques. lichen pila´ris lichen spinulosus. lichen planopila´ris a variant of lichen planus characterized by formation of cone-shaped horny papules around the hair follicles, in additionto the typical lesions of ordinary lichen planus. lichen pla´nus an inflammatory skin disease with wide, flat, purplish, shiny papules in circumscribed patches; it may involve the hairfollicles, nails, and buccal mucosa; called also lichen ruber planus. lichen ru´ber monilifor´mis a generalized or localized eruption with either round, dome-shaped, waxy, dark or bright red papules, or waxy,yellow, milia-like papules, often forming a moniliform (string-of-beads) pattern, sometimes arranged in keloidal bands. Some authoritiesconsider the condition to be a variant of lichen simplex chronicus. lichen ru´ber pla´nus lichen planus. lichen sclero´sus (lichen sclero´sus et atro´phicus) a chronic atrophic skin disease marked by white papules with an erythematous haloand keratotic plugging. It sometimes affects the vulva (kraurosis vulvae) or penis (balanitis xerotica obliterans). lichen scrofuloso´rum (lichen scrofulo´sus) a form of tuberculid manifested as an eruption of clusters of lichenoid papules on the trunk ofchildren with tuberculous disease. lichen sim´plex chro´nicus dermatosis of psychogenic origin, marked by a pruritic discrete, or more often, confluent lichenoid papulareruption, usually confined to a localized area. Mechanical trauma, such as scratching or rubbing the area, is a factor in its development.The lesions may arise from normal skin or they may occur as a complication of other forms of dermatitis. Called also circumscribed orlocalized neurodermatitis and lichen chronicum simplex. Treatment consists of administration of corticosteroids applied locally as a cream or given by intralesional injection to relieve the pruritus.The area should be protected by light dressings and the patient encouraged to avoid mental stress, emotional upsets, and irritation of theaffected area. The application of very hot or very cold compresses may afford temporary relief of the itching. The condition tends to becomechronic with unexplained remissions and reappearance of lesions in a different part of the body. lichen spinulo´sus a condition in which there is a horn or spine in the center of each hair follicle; called also lichen pilaris. lichen stria´tus a self-limited condition characterized by a linear lichenoid eruption, usually in children. lichen urtica´tus papular urticaria. Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved. lichen planus (lī´kn plā´ns), n a dermatologic disease affecting the skin and oral mucosa; of unknown etiology but often associated with nervousness, fatigue,emotional depression, and allergy and considered to be a manifestation of quinacrine (Atabrine) therapy. Oral lesions often appear aswhite or blue-white striae forming an interweaving lacelike network of lines of epithelial thickening. Associated with the striated network;bullous or erosive lesions may be found. Histologically, varying degrees of hyperkeratosis and epithelial acanthosis may be found, withformation of sawtooth-shaped rete pegs of epithelium projecting into connective tissue. Subjacent to the epithelium is a bandlike infiltrateof round cells with perivascular accumulation of leukocytes. Treatment is symptomatic. Lichen planus. lichen planus, oral, n See lichen planus. Mosby's Dental Dictionary, 2nd edition. © 2008 Elsevier, Inc. All rights reserved. lichen planus Dermatology A pruritic dermatopathy of flexor surfaces–especially wrist, orogenital mucosa, characterized by papular thickening of upperdermis, a shiny violaceous surface Management Corticosteroids McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc. li·chen pla·'nus eruption of flat-topped, shiny, violaceous papules on flexor surfaces, male genitalia, and buccal mucosa of unknown cause; may formlinear groups; microscopically characterized by a bandlike subepidermal lymphocytic infiltrate. Spontaneous resolution is common aftermonths to years. Farlex Partner Medical Dictionary © Farlex 2012 li·chen pla·nus , lichen ruber planus (lī'ken plā'nŭs, rū'bĕr) Eruption of flat-topped, shiny, violaceous papules on flexor surfaces, male genitalia, and buccal mucosa of unknown cause; may formlinear groups. Spontaneous resolution is common after months to years. Medical Dictionary for the Health Professions and Nursing © Farlex 2012 li·chen pla·nus , lichen ruber planus (lī'ken plā'nŭs, rū'bĕr) Eruption of flat-topped violaceous papules on flexor surfaces and buccal mucosa of unknown cause. Medical Dictionary for the Dental Professions © Farlex 2012 Wilson, Sir William J.E., English dermatologist, 1809-1884. Wilson lichen - eruption of flat-topped, shiny, violaceous papules on flexor surfaces, male genitalia, and buccal mucosa of unknowncause. Synonym(s): lichen planus Medical Eponyms © Farlex 2012 lichen planus; LP eruption of flat-topped, shiny, violaceous, pruritic papules with overlying fine white scale (Wickham's striae) classically offlexor surfaces and buccal mucosa that gradually become symptomless and fade to brown over ensuing months; unknown cause but oftenpresents at times of stress, or in association with local trauma (see Koebner phenomenon) in susceptible individuals; plantar lesions may formparakeratotic plaques; some patients show insulin resistance and prediabetic response to glucose tolerance test |
|
|
|
Lichenoid eruptions |
Drug-induced lichenoid reactions that are clinically and |
|
|
|
GVHR |
In the acute stage of graft-versus-host disease (GVHD, |
|
|

|
ichen planus. Violaceous papules on the flexural aspect of |
|
|
|
Wiki |
Lichen planus Lichen planus Classification and external resources Lichen planus affecting the shins. ICD-10L43 ICD-9697.0 DiseasesDB7452 MedlinePlus000867 eMedicinederm/233 derm/663 MeSHD008010, D017676 Lichen planus (LP) is a disease of the skin and/or mucous membranes thatresembles lichens. It is thought to be the result of an autoimmune process withan unknown initial trigger. Where the trigger is known, a lesion is known as alichenoid lesion. There is no cure, but many different medications andprocedures have been used to control the symptoms. Classification Lichen planus has been described as an autoimmune disease,[1] a dermatosis,[2]a papulosquamous disorder, a mucocutaneous disease,[3] and an inflammatorydisease.[4] Lichen planus lesions are classified because of their "lichen-like" appearance.[5]Such lesions can be classified by the site they involve, or by their morphology. Site Lichen planus may be categorised as affecting mucosal or cutaneous surfaces. Cutaneous forms are those affecting the skin, scalp, and nails.[2][3][6] Mucosal forms are those affecting the lining of the gastrointestinal tract(mouth, pharynx, esophagus, stomach, anus), larynx, and other mucosalsurfaces including the genitals, peritoneum, ears, nose, bladder andconjunctiva of the eyes.[4][7][8]Pattern Lichen planus lesions can occur in many different forms: Lichen planuslesionmorphologyDescription [9]:465-8[10]:219-224 AnnularMeaning 'ring-shaped' lesions that develop with circular groups of papules with clear, unaffected skin in the center,occurring in occurs in approximately ten percent of lichen planus cases. LinearPapules are arranged in a line (the "Blaschko line").[11] This pattern may develop secondary to trauma (koebnerization)or uncommonly as a spontaneous, isolated eruption, usually on the extremities, and rarely on the face.[12] HypertrophicThis patterrn usually occurs on the extremities, especially the shin and interphalangeal joints, and tends to be the mostpruritic variant of lichen planus. Also known as "Lichen planus verrucosus". AtrophicThis morphology is characterized by the presence of a few well-demarcated, white-bluish papules or plaques withcentral superficial atrophy. This is a rare variant of lichen planus. BullousThis morphology is characterized by the development of vesicles and bullae with the skin lesions. This is a rare variantof lichen planus, and also known as "Vesiculobullous lichen planus". UlcerativeThis morphology is characterized by chronic, painful bullae and ulceration of the feet, often with cicatricial sequelaeevident. This is a rare variant of lichen planus. PigmentedThis morphology is characterized by hyperpigmented, dark-brown macules in sun-exposed areas and flexural folds.This is a rare variant of lichen planus. Overlap syndromes Occasionally, lichen planus is known to occur with other syndromes. For example: Lupus erythematosus–lichen planus overlap syndrome. Lesions of this syndrome share features of lupus erythematosus and lichenplanus. Lesions are usually large and hypopigmented, atrophic, and wiith a red-to-blue colour and minimal scaling. Telangectasia maybe present.[9]:366,470-1[10] Lichen planus–lichen sclerosus overlap syndrome sharing features of lichen planus and lichen sclerosus.[10]:220Signs and symptoms Lichen planus affecting the lower lip. Although lichen planus can present with a variety of lesions, it is typically described as a well-defined area of a purple-coloured itchy rash of flat-topped papules with interspersed lacy white lines(Wickham's striae). This description is known as the characteristic "6 P's" of lichen planus.[6] Thisrash, after regressing, is likely to leave an area of hyperpigmentation that slowly fades. That said, avariety of other lesions can also occur.[5] Cutaneous lichen planus Variants of cutaneous lichen planus are distinguished based upon the appearance of the lesionsand/or their distribution.[9] Lesions can affect the: Extremities (face, dorsal hands, arms, and nape of neck). This is more common in MiddleEastern countries in spring and summer, where sunlight appears to have a precipitating effect. This is also known as "Lichen planusactinicus", "Actinic lichen niditus," "Lichen planus atrophicus annularis," "Lichen planus subtropicus," "Lichen planus tropicus,""Lichenoid melanodermatitis," and "Summertime actinic lichenoid eruption"[9]:468[10]:223[12] Palms and soles Intertriginous areas of the skin. This is also known as "Inverse lichen planus".[12] Nails[13] characterized by irregular longitudinal grooving and ridging of the nail plate, thinning of the nail plate, pterygium formation,shedding of the nail plate with atrophy of the nail bed, subungual keratosis, longitudinal erthronychia (red streaks), and subungualhyperpigmentation.[10]:781 A sand-papered appearance is present in around 10% of individuals with nail lichen planus.[13] Scalp. This is also known as lichen planopilaris, acuminatus, follicular lichen planus, and peripilaris,[9]:467 characterised by violaceous,scaly, pruritic papules. Scalp lichen planus can cause scarring alopecia if it is untreated.[6][10]:223[14] Hair. This variant causes inflamation of hair follicles and gradual replacement with scarring. About 10% of people with lichen planus havethe scalp or nail variants of the condition.[6]Other variants may include: Lichen planus pemphigoides characterized by the development of tense blisters atop lesions of lichen planus or the developmentvesicles de novo on uninvolved skin.[9]:471 Keratosis lichenoides chronica (also known as "Nekam's disease") is a rare dermatosis characterized by violaceous papular andnodular lesions, often arranged in a linear or reticulate pattern on the dorsal hands and feet, extremities, and buttock.[9]:472[10]:224[12] Lichenoid keratoses (also known as "Benign lichenoid keratosis," and "Solitary lichen planus"[12]) is a cutaneous conditioncharacterized by brown to red, scaling maculopapules found on sun-exposed skin of extremities.[9]:473[12] Restated, this is a cutaneouscondition usually characterized by a solitary dusky-red to violaceous papular skin lesion.[10]:639 Lichenoid dermatitis represents a wide range of cutaneous disorders characterized by lichen planus-like skin lesions.[9]:473[12]Mucosal lichen planus Lichen planus on the lips and the lateralborder of the tongue Lichen planus affecting mucosal surfaces may have one lesion or be multifocal.[15] Examples oflichen planus affecting mucosal surfaces include:[15] Oral lichen planus, (see below). Esophageal lichen planus, affecting the esophageal mucosa. This can present withdifficulty or pain when swallowing, due to an esophagitis or the development of anesophageal stricture. It has also been hypothesized that it is a precursor to squamous cellcarcinoma of the esophagus.[7][16] Genital lichen planus, which may cause lesions on the glans penis or skin of the scrotomin males, and the vulva or vagina in females.[6] Symptoms may include lower urinary tractsymptoms associated with urethral stenosis, dyspareunia (painful sexual intercourse), andpruritus (itching).[6] Vulvovaginal-gingival syndrome, (females) and peno-gingival syndrome (males) are severe and distinct variantsaffecting vulva, vagina, and gums (females) and glans penis and gums (males).[12] It is associated with HLA-DQB1.[12][17] This mayresult in scarring, vaginal stricture formation,[18] or vulva destruction.[19]Oral lichen planus Oral lichen planus (also termed oral mucosal lichen planus),[20] is where lichen planus involves the the lining of the mouth, the oral mucosa.This may occur combination with other variants of lichen planus.[21] 6 clinical forms of oral lichen planus are recognized:[21] Reticular, the most common presentation of oral lichen planus,[1] characterised by the net-like appearance of lacy white lines, oralvariants of Wickham's straiae.[21] This is usually asymptomatic.[1] Erosive/ulcerative, the second most common form of oral lichen planus,[1] characterised by oral ulcers prsenting with persistent,irregular areas of redness (redness), ulcerations and erosions covered with a yellow slough. This can occur in one or more areas of themouth. In 25% of people with erosive oral lichen planus, the gums are involved, described as desquamative gingivitis (a condition notunique to lichen planus). It may be the initial or only sign of the condition.[21] Papular, with white papules. Plaque-like appearing as a white patch which may resemble leukoplakia.[21] Atrophic, appearing as areas. Atrophic oral lichen planus may also manifest as desquamative gingivitis.[21] Bullous, appearing as fluid-filled vesicles which project from the surface.These types often coexist in the same individual. Oral lichen planus tends to present bilaterally as mostly white lesions on the inner cheeck,[1]although any mucosal site in the mouth may be involved. Other sites, in decreasing order of frequency, may include the tongue, lips, gingivae,floor of the mouth, and very rarely, the palate.[1] Generally, oral lichen planus tends not to cause any discomfort or pain, although some people may experience soreness when eating ordrinking acidic or spicy foodstuffs or beverages.[21] When symptoms arise, they are most commonly associated with the atrophic andulcerative subtypes. These symptoms can include a burning sensation to severe pain.[1] Causes The cause of lichen planus is unknown,[5][17][22] but it is not contagious and does not involve any known pathogen.[23] It is thought to be a T cell mediated autoimmune reaction (where the body's immune system targets its own tissues).[1] This autoimmune process triggers apoptosisof the epithelial cells.[1] Several cytokines are involved in lichen planus, including tumor necrosis factor alpha, interferon gamma, interleukin-1 alpha, interleukin 6, and interleukin 8.[1] This autoimmune, T cell mediated process is thought to be in response to some antigenic change inthe oral mucosa, but a specific antigen has not been identified.[1] Where a causal or triggering agent is identified, this is termed a lichenoid reaction rather than lichen planus. These may include:[8] Drug reactions, with the most common inducers including gold salts, beta blockers, antimalarials, thiazide diuretics, furosemide,spironolactone, Metformin and penicillamine.[23] Reactions to amalgam (metal alloys) fillings.[24] Graft-versus-host disease lesions, which chronic lichenoid lesions seen on the palms, soles, face and upper trunk after several months.[23] Hepatitis, specifically hepatitis B and hepatitis C infection, and primary biliary cirrhosis.[10]:220[23]It has been suggested that lichen planus may respond to stress, where lesions may present during times of stress. Lichen planus can be partof Grinspan's syndrome.[citation needed] Diagnosis Lichen planus lesions are diagnosed clinically by their "lichen-like" appearance.[5] A biopsy can be used to rule out conditions that mayresemble lichen planus, and can pick up any secondary malignancies.[25] Histopathology Micrograph of lichen planus. H&E stain. Lichen planus has a unique microscopic appearance that is similar between cutaneous, mucosaland oral. A Periodic acid-Schiff stain of the biopsy may be used to visualise the specimen.Histological features seen include:[26] thickening of the stratum corneum both with nuclei present (parakeratosis) and without(orthokeratosis). Parakeratosis is more common in oral variants of lichen planus. thickening of the stratum granulosum thickening of the stratum spinosum (acanthosis) with formation of colloid bodies (alsoknown as Civatte bodies, Sabouraud bodies) that may stretch down to the lamina propria. liquefactive degeneration of the stratum basale, with separation from the underlying lamina propria, as a result of desmosome loss, creating small spaces (Max Joseph spaces). Infiltration of T cells in a band-like pattern into the dermis[1] "hugging" the basal layer. Development of a "saw-tooth" appearance of the rete pegs, which is much more common in non-oral forms of lichen planus.Differential Diagnosis The differential diagnosis for OLP includes: Other oral vesiculo-ulcerative conditions such as Pemphigus vulgaris and Benign mucous membrane pemphigoid Lupus erythematosus, with lesions more commonly occur on the palate and appear as centrally ulcerated or erythematous withradiating white striae. In contrast, OLP and lichenoid reactions rarely occur on the palate, and the striae are randomly arranged ratherthan radial.[27] Chronic ulcerative stomatitis Frictional keratosis and Morsicatio buccarum (chronic cheek biting) Oral leukoplakia Oral candidiasisTreatment There is no cure for lichen planus,[1] and so treatment of cutaneous and oral lichen planus is for symptomatic relief or due to cosmeticconcerns.[1][5][25] When medical treatment is pursued, first-line treatment typically involves corticosteroids,[5] and removal of any triggers.[24]Without treatment, most lesions will spontaneously resolve within 6–9 months for cutaneous lesions,[5] and longer for mucosal lesions [26] Cutaneous lichen planus Many different treatments have been reported for cutaneous lichen planus, however there is a general lack of evidence of efficacy for anytreatment.[11][28] Treatments tend to be prolonged, partially effective and disappointing.[11] First-line treatments may include retinoids such asAcitretin, or corticosteroids [5][11][28] A variety of other therapies are also used if these are unsuccessful. These include oral corticosteroids, vitamin D3 analogues, antibiotics suchas Dapsone, hydroxychloroquine and Cyclosporin, some anti-coagulants, and psoralen plus ultraviolet-A.[5][11][28] Cosmetic treatments may include laser surgery, cryotherapy, and phototherapy.[11][28] Oral lichen planus Reassurance that the condition is benign, elimination of precipitating factors and improving oral hygiene are considered initial management forsymptomatic OLP, and these measures are reported to be useful.[1] Treatment usually involves topical corticosteroids (such asbetamethasone, clobetasol, dexamethasone, and triamcinolone) and analgesics, or if these are ineffective and the condition is severe, thesystemic corticosteroids may be used. Calcineurin inhibitors (such as pimecrolimus, tacrolimus or cyclosporin) and retinoids (such astretinoin) are sometimes used.[1] Prognosis In contrast to cutaneous lichen planus, lichen planus lesions in the mouth may persist for many years,[25] and tend to be difficult to treat, withrelapses being common.[17] Atrophic/erosive lichen planus is associated with a small risk of malignant transformation,[25] and so people withOLP tend to be kept on long term review to detect any potential change early. Sometimes OLP can become secondarily infected with Candidaorganisms.[citation needed] Epidemiology The overall prevalence of lichen planus in the general population is about 0.1 - 4%.[6] It generally occurs more commonly in females, in a ratioof 3:2, and most cases are diagnosed between the ages of 30 and 60, but it can occur at any age.[6][29] Oral lichen planus is relatively common,[17] It is one of the most common mucosal diseases. The prevalence in the general population is about1.27-2.0%,[1][25] and it occurs more commonly in females than males, and in middle aged people.[1] OLP in children is rare. About 50% offemales with oral lichen planus were reported to have undiagnosed vulvar lichen planus.[6] History Lichen planus was first reported in 1869 by Erasmus Wilson |
|