![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
95 Cards in this Set
- Front
- Back
|
What is the urinary system comprised of? |
Kidneys (urine forming organs) and structures that carry urine from the kidneys to the outside of the body -> ureters, urinary bladder, and urethra |
|
|
What is the function of the kidney? |
Regulations of body's water and solute composition (osmoregulation); filters waste (metabolic, foreign), produces urine to remove waste products and excess water, ions. |
|
|
Any other functions? |
Also has an endocrine function -> production of hormones (renin, erythropoietin) and activation of vitamin D. |
|
|
What are the kidneys referred to as? |
Guardians of the internal environment. |
|
|
How is the kidney supplied blood? |
Renal artery and renal vein |
|
|
Where does urine drain to as it forms? |
into the renal pelvis, located at the inner core of each kidney |
|
|
What is the function of the bladder? |
Temporary storage site for Urine; hollow, distensible sac with smooth muscle in the walls. periodically empties to the outside of the body through the urethra |
|
|
What is the function unit of the kidney? How many are there? |
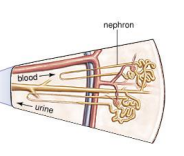
The nephron; 10^6. |
|
|
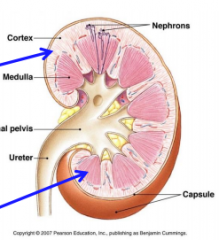
How are nephrons arranged? |
The arrangement gives rise to two distinct regions in the kidney: the Renal cortex; outer region lighter in appearance, and renal medulla; inner region made up of striated triangles called renal pyramids. |
|
|
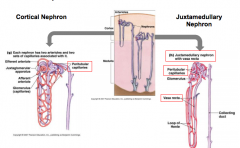
What are the two different types of nephrons? |
Cortical nephrons (80% of the nephrons are almost completely contained within cortex) and Juxtamedullary nephrons (20% of nephrons dip down into the medulla) |
|
|
Picture of nephron anatomy |

|
|
|
How many afferent and efferent arterioles are associated with each nephron? |
1 of each. |
|
|
What is the dominant feature of a nephron? |
The glomerulus, a ball like group of capillaries |
|
|
What's special about efferent arterioles? |
They are the only arterioles in the body that drain blood FROM the capillaries. |
|
|
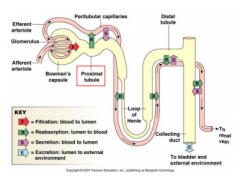
Which capillaries supply the renal tissue, and what occurs here? |
Peritubular supply the renal tissue, and this is where reabsorption and secretion occurs. |
|
|
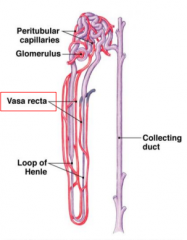
A picture of the vessels in the Nephron |

|
|
|
What does the Juxtamedullary nephron have that the cortical does not? |
The vasa recta. |
|
|
What is the vasa recta? |
A series of vessels which surround the collecting ducts and the Loop of Henle in Juxtamedullary nephrons. Supplies O2 and nutrients to the nephron segments; allows for return of reabsorbed water and solutes to the circulatory system |
|
|
Picture of vasa recta? |
|
|
|
What is a unique feature of the renal vasculature? |
The afferent and efferent arterioles have different diameters; the efferent arteriole is quite a bit smaller in diameter. Why is this important? It creates a 'backup' in the glomerulus which creates higher pressure in the glomerular cavity. |
|
|
Let's back up. What does the afferent arteriole do, and what does the efferent do? |
Afferent brings blood to the glomerulus, whereas the efferent takes blood away from the glomerulus. |
|
|
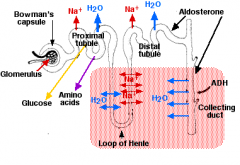
Where do the filtered components go after the glomerulus? What are these components? |
Bowman's capsule. Includes water, glucose, amino acids, and ions, and also waste (creatinine and urea). |
|
|
How much of the filtrate leaves the nephrons? |
1% |
|
|
Where does the efferent arteriole go after leaving the glomerulus? |
It branches out to form capillaries that wrap around the tubules. |
|
|
What is secretion? What materials tend to be secreted? |
Where some fluid leaves the capillaries and enter the tubules. Usually ammonia and medication (drugs) are secreted into tubules. |
|
|
What percentage of glucose and amino acids are reabsorbed? |
About 100% |
|
|
What happens in the descending limb of the loop of Henley? |
Permeable to water but low permeability to ions such as sodium and urea. Water leaves the tubule due to osmosis (due to salty environment in medulla) |
|
|
What is the main characteristic of the filtrate by the time it reaches the bottom of the loop? |
It is highly concentrated. |
|
|
What happens in the ascending limb? |
Impermeable to water, so any water remaining in the filtrate cannot escape. Sodium is actively pumped out of the thick portion of the ascending limb, and passively leaves out of the thin portion. About 25% of NaCl is reabsorbed. After these processes have occurred, the filtrate is dilute. |
|
|
How do efferent and afferent arterioles control blood flow to glomerulus? |
By constricting and dilating. |
|
|
Would glomerulus filtration rate be increased or decreased with the dilation of the afferent arteriole AND constriction of the efferent arteriole? |
GFR would increase because as the afferent arteriole dilates, more blood enters glomerulus. As the efferent arteriole constricts, the filtration pressure would increase and filtrate would enter the proximal tube (tubule immediately after glomerulus) |
|
|
Picture of material transport |
|
|
|
What affects glomerular capillary blood pressure? |
contraction of the heart (Co = HR x SV) and the resistance to blood flow offered by afferent and efferent arterioles |
|
|
What is the net pressure calculation in glomerulus? |
55 mm Hg (BP) - 30 mm Hg (osmotic pressure) - 15 mm Hg (filtrate pressure) = net 10 mm Hg pressure into tubule. |
|
|
What is filtered during glomerular filtration? What cannot pass? |
Plasma is filtered. Protein cannot pass. |
|
|
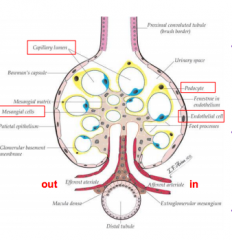
What are the three main structures of the glomerulus and what do they do? |
Glomerular Capillary wall: single layer of endothelial cells that are more permeable to water and solutes than capillaries elsewhere in the body; Mesangial cells: specialized smooth muscle cells that can regulate blood flow through capillaries, and Podocytes: these wrap around the capillaries and leave slits between them. Blood is filtered through these slits. |
|
|
Detailed picture of Glomerulus Structure. |
|
|
|
What is the basic nephron function? |
The maintenance of blood volume and electrolyte balance. |
|
|
What is the equation for total amount of solute excreted? |
Amount filtered - amount reabsorbed + amount secreted. |
|
|
What is the basic structure of the tubular nephron? |
A hollow, fluid-filled tube formed by a single layer of epithelial cells. |
|
|
What are the different function regions of the nephron? |
Bowman's capsule, proximal tubule, loop of Henle, distal tubule, collecting duct. |
|
|
What is the main function of Bowman's capsule? Proximal tubule? |
Collects glomerular filtrate; reabsorption and secretion of substances. |
|
|
What is the main function of the loop of Henle? |
Descending and ascending limbs: osmotic gradient established in Juxtamedullary nephrons. |
|
|
What is the main function of the distal tubule? Collecting duct? |
Regulated reabsorption; collects urine |
|
|
What is tubular reabsorption? |
Transfer of substances from tubular lumen into peritubular capillaries - essential 'stuff' returned to body. Highly selective, but variable - a highly regulated process. |
|
|
Picture of tubular reabsorption |
|
|
|
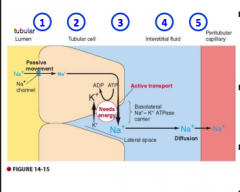
What are the reabsorption steps? |
1) Leave tubular fluid by crossing luminal membrane of tubular epithelial cell 2) pass through cytosol from one side of tubular cell to the other 3) cross basolateral membrane of the tubular cell to enter interstitial fluid 4) diffuse through interstitial fluid 5) penetrate capillary wall to enter blood plasma |
|
|
How much of urea is reabsorbed? Phenol? Water, sodium, glucose? |
50, 0, 99, 99.5, 100 |
|
|
What is the difference between passive and active tubular reabsorption? |
Passive requires no energy, occurs down electrochemical or osmotic gradients. Active reabsorption requires energy as movement occurs against electrochemical or concentration gradient. |
|
|
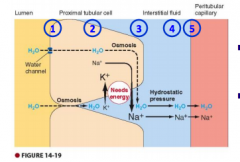
Describe the active Na reabsorption process |
Sodium potassium pump in basolateral membrane is essential for Na reabsorption. 80% of total energy spent by kidneys is used for Na transport. Water follows reabsorbed Na by osmosis. Mainly affects blood volume and pressure. |
|
|
Picture of Na reabsorption |
|
|
|
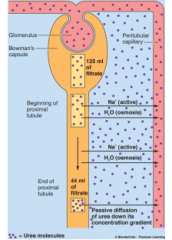
Describe proximal tubule water reabsorption |
Water follows reabsorbed Na by Osmosis; mainly affects blood volume and pressure. Hypertonicity in lateral spaces, established by active extrusion of Na, is the force for water reabsorption. |
|
|
Picture of water reabsorption |
|
|
|
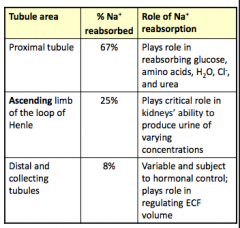
Sodium absorption. How much is absorbed in the proximal tubule, the ascending limb, and the distal collecting tubes? What is the role of Na reabsorption in each section? |
|
|
|
What really controls Na reabsorption? |
Hormones. Renin is secreted by Juxtaglomerular granular cells in response to low NaCl. Complicated system (slide 32) |
|
|
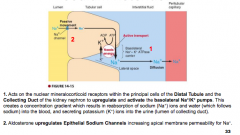
How does Aldosterone increase sodium retention? |
|
|
|
What does Atrial Natriuretic Peptide (ANP) do? |
Inhibits Na reabsorption; secreted by specialized cells in the Atria in response to stretch caused by expansion of ECF (caused by Na retention) and increased arterial pressure. ANP release prompts additional effects (natriuretic, diuretic, hypotensive) that help correct original stimulus. |
|
|
What do natriuretic, diuretic mean? |
Natriuresis: discharge of sodium through urine Diuretic: Elevates discharge of urine |
|
|
How can ANP increase Sodium excretion? |
Dilates the Afferent glomerular arteriole, constricts the Efferent glomerulararteriole, and relaxes the mesangial cells (this increases pressure in the glomerularcapillaries, thus increasing the glomerular filtration rate (GFR), resulting in greaterexcretion of sodium and water) |
|
|
How else can ANP increase sodium excretion? |
Increases blood flow through the vasa recta, which will wash the solutes (NaCl andurea) out of the medullary interstitium (the lower osmolarity of the medullaryinterstitium leads to less reabsorption of tubular fluid and increased excretion)-decreases sodium reabsorption in the Distal convoluted tubule and collecting ductby inhibiting the Epithelial Sodium Channel-Inhibits Renin secretion, thereby inhibiting the Renin–Angiotensin–Aldosteronesystem |
|
|
Discuss glucose reabsorption (Active) |
Some glucose is filtered and ends up in Bowman's capsule; but completely reabsorbed through Sodium Glucose Co-Transport proteins (SGLT) |
|
|
How is Urea passively reabsorbed? |
Firstly, urea is a nitrogen-containing waste product from the breakdown of protein in the liver. Reabsorption occurs mainly at Collecting Duct (50%). Indirectly linked to active Na reabsorption (Osmotic reabsorption of H2O in theproximal tubule produces a [gradient] forpassive reabsorption of urea) |
|
|
Picture of Urea Reabsorption |
|
|
|
What is tubular secretion? |
Transfer of substances from peritubular capillaries into the tubular lumen for eventual excretion. |
|
|
Where is most K reabsorbed? |
In the proximal tubule; at the distal tubule only 5-10% of filtered load remains, mostly secreted at the distal tubule. |
|
|
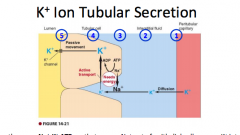
Picture of K ion tubular secretion |
|
|
|
How does K ion tubular secretion work? |
the same Na+-K+ ATPase that pumps Na+ out of epithelial cells pumps K+intothe cells; K concentration gradient allow diffusion of K into the lateral spaces, andpassive movement into the tubules for excretion |
|
|
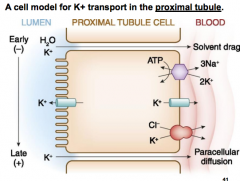
Another picture of K transport in the proximal tubule |
|
|
|
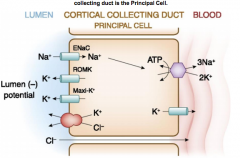
A picture of K transport in the cortical collecting duct (the principal cell) |
|
|
|
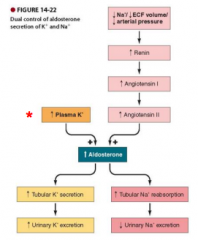
What regulates K secretion? |
Aldosterone from the adrenalcortex is most importantregulator of K+secretion; Simultaneous Reabsorption ofNa+ and Secretion of K+ |
|
|
Picture of Aldosterone regulating K secretion |
|
|
|
H+ - Important tubular secretion systems |
Important in regulating acid-base balance Secreted at proximal, distal, and collecting tubules |
|
|
K+ - Important tubular secretion systems |
Plasma [K+] kept at appropriate levels to maintain normal membraneexcitability in Muscles and Nerves Secreted only at the Distal and Collecting tubules under control ofaldosterone (an adrenal hormone) |
|
|
Organic Ions - Important tubular secretion systems |
Secreted only at the proximal tubule Includes blood-borne chemical messengers (i.e. histamine, NE);insoluble molecules initially bound to proteins; foreign organicmolecules such as drugs, food additives, pollutants, etc., etc. |
|
|
Why do Juxtamedullary nephrons have long loops of Henle? |
Important to establish Osmotic gradients. |
|
|
Flow through the nephron, specifically the loop of Henle, is influenced by.... |
The gradient of osmolarity, which increases with toward the distal end of the loop of Henle. |
|
|
Picture of Loop of Henle reabsorption |

|
|
|
What happens in the descending tube? |
Descending loop is highly permeable toH2O, but does not reabsorb Na+(Concentrates urine) -Osmotic pressure favors waterreabsorption |
|
|
What happens in the ascending tube? |
The Ascending limb actively transportsNa and Cl out of the tubular lumen intosurrounding ECF, but is impermeable toH2O (Dilutes urine) |
|
|
What is partially responsible for selective water reabsorption? |
Aquaporins (selective water channels) |
|
|
How can the GFR be regulated? |
By adjusting the glomerular capillary BP to suit the bodies needs. Two types: autoregulation (prevents spontaneous changes in GFR 1a, 1b) and extrinsic sympathetic control 2a, 2b (long term regulation of arterial BP) |
|
|
1a How does myogenic autoregulation work? |
kidneys can 'auto-regulate' blood flow to glomerular capillaries; arteriolar resistance is adjusted locally (vasoconstriction or dilation); occurs due to the myogenic properties (originating in muscle tissue) of the arterioles |
|
|
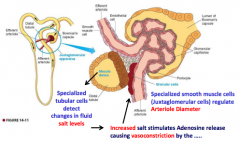
1b What about autoregulation via the Juxtaglomerular apparatus? |
The twisted configuration of the nephron causes the final portion of theAscending loop of Henle to pass between the Afferent and Efferentarterioles. |
|
|
How does this work? |
A decrease in sodium chloride concentration initiates asignal from the Macula Densa that has two effects: (1) it decreases resistance to blood flow in the AfferentArterioles, which raises glomerular hydrostaticpressure, and (2) it increases Renin release from the Juxtaglomerularcells of the afferent arterioles |
|
|
Picture of Tubuloglomerular feedback |
|
|
|
2a) What is the importance of extrinsic regulation? |
Fight or flight; GRF can be changed due to vasoconstriction and decreased renal blood flow; mediated by SNS input to afferent arterioles of glomerulus |
|
|
Is there any parasympathetic input to the kidneys? |
NO. |
|
|
2b) Baroreceptor Regulation |
long term regulation of arteriole blood pressure; changes in BP are detected by aortic and carotid baroreceptors; mechanoreceptors are sensitive to changes in arterial pressure = pressure mechanoreceptors. |
|
|
What does the solute concentration of urine depend on? |
The body's state of hydration; too much water in the ECF establishes a hypotonic EFC (less concentrated urine) whereas a water deficit established a hypertonic ECF (more concentrated urine) |
|
|
How much blood plasma is filtered daily? |
~ 125 ml/min males, 115 females so about 180 L per day, 166 L day in females |
|
|
What percentage of 180L is reabsorbed? |
99% - the body would rapidly dehydrate if reabsorption didn't occur. ~1.5 L of urine is excreted daily. |
|
|
How many times per day is overall plasma filtered? |
60x. |
|
|
What is renal failure? |
Kidney function Decreases with Age GFR declines at a rate of ~10 mL/min/1.73 m2for each decade beyondthe age of 30 |
|
|
What are some causes of renal failure? |
infectious organisms• toxic agents• inappropriate immune responses• obstruction of urine flow• an insufficient renal blood supply |
|
|
What are some engineering solutions? |
Hemodialysis; kidney transplant; bioengineered kidney. |