Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
27 Cards in this Set
- Front
- Back
|
1. Define and describe the pleural cavity.
Pleural cavity |
»In the adult, the pleural cavity is small, having been nearly obliterated by the lung that expanded into it during development.
»The pleural cavity is the space b/w the visceral pleura that is tightly applied to the lung itself, and the parietal pleura which is applied to the body wall. |
|
|
(Define and describe the pleural cavity)
Parietal pleura |
Parietal pleura - applied to the body wall
»Subdivided according to the areas it covers: (i)Costal (ii)Mediastinal (iii)Diaphragmatic (iv)Pleural cupula »The inferior part of the costodiaphragmatic recess is not invaded by the lungs. |
|
|
(Define and describe the pleural cavity)
Blood supply |
1) Segmental vessels of the thoracic wall (intercostal aa.):
SUPPLIES - Costal pleura. 2) Bronchial aa. - branch from the aorta (3rd intercostal a. on right side) SUPPLIES - (i)Visceral pleura and (ii)lung tissue. |
|
|
(Define and describe the pleural cavity)
Visceral pleura vs. Parietal pleura sensitivity. |
»Visceral pleura is not sensitive to sharp (somatic) pain, but the parietal pleura is very sensitive.
»Irritation of costal pleura causes pain to be referred to the chest wall, but pain originating from diaphragmatic or mediastinal pleurae is usually referred to the neck because of the common segmental origins of the supraclavicular (C3, 4) and phrenic nn (C3,4,5). |
|
|
(Define and describe the pleural cavity)
Pneumothorax |
»Occurs when air enters the pleural cavity.
»This causes a loss of the negative pressure which is normally present in this "potential" space. Collapse of the lung ensues due to its elasticity. |
|
|
(Define and describe the pleural cavity)
Hemothorax |
»Occurs when blood collects in the pleural cavity.
|
|
|
(Define and describe the pleural cavity)
Extent of Pleura |
»Rises as far superiorly as the neck of the first rib.
E.g. above the level of the jugular notch. »The costodiaphragmatic recess is quite extensive - this, in keeping with the domed shape of the diaphragm. |
|
|
2. Describe the lungs.
Surfaces |
»Each lung has three surfaces:
(i) Costal (ii) Medial (including both mediastinal and vertebral). (iii) Diaphragmatic |
|
|
(Describe the lungs)
Right vs. Left lung |
Right lung:
Lobes - 3 (superior, middle, inferior) Fissures - Oblique & horizontal Left lung: Lobes - 2 (superior, inferior) Fissures - Oblique NOTE: i)Oblique fissures define the lower (basal) lobes. ii)Horizontal fissure of the right lung defines the upper and middle lobes. |
|
|
(Describe the lungs)
Lingula |
»"Tongue of the lung" of the upper lobe of the left lung; it is in the same general position as the middle lobe of the right lung.
|
|
|
(Describe the lungs)
How do lungs receive air? |
»Each lung receives air via a branch of the trachea. That branch of the trachea is called a primary bronchus.
Note: Primary bronchus of the right lung is larger and more vertical than the left primary bronchus. »As a result, inhaled foreign objects usually pass into the right lung. |
|
|
(Describe the lungs)
Subdivisions of Primary bronchus. |
»Each primary bronchus divides into secondary (lobar) bronchi.
»Secondary (lobar) bronchi subdivides into tertiary (segmental) bronchi. Note: Tertiary (segmental) bronchi have usually 10 on the right, 8 on the left. |
|
|
(Describe the lungs)
Characteristic of arteries. |
»Arteries always carry blood away from the heart, regardless of the blood oxygen's content.
|
|
|
(Describe the lungs)
Structures that enter and leave the lung. |
»Structures that enter and leave the lung form its root.
»The root joins the lung at the hilus. »At the hilus the usual arrangement is as follows: (i)Bronchus - lies posteriorly (ii)Pulmonary artery - superior (iii)Pulmonary veins - inferior ("Bronchi to the back, aa. above vv.") »Below the root, the pulmonary ligament further tethers the lung to the mediastinal pleura. |
|
|
(Describe the lungs)
Removal of lung. |
»In the laboratory, the pulmonary ligament must be severed before the lung can be removed for further study.
|
|
|
(Describe the lungs)
How does the bronchopulmonary segment of lungs receive air? |
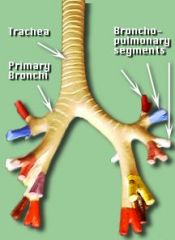
»Each bronchopulmonary segment receives air via its own segmental bronchus.
|
|
|
(Describe the lungs)
Bronchopulmonary segment: a) How does it receive de-oxygenated blood? b) How does it send back oxygenated blood? |
a) Via its own branch of the pulmonary artery.
b) Oxygenated blood is sent back toward the left atrium via pulmonary veins which often drain more than one bronchopulmonary segment. |
|
|
(Describe the lungs)
Major contact impressions of the lungs. |
Right lung:
(i) Groove for the esophagus (ii) Cardiac impression (iii) Grooves for the brachiocephalic v. (iv) Grooves for superior vena cava (v) Arch of the azygos v. Left lung: (i) Groove for the subclavian a. (ii) Groove for the aorta (iii) Cardiac impression |
|
|
3. Describe ventilation.
How is air brought into the lungs? |
»Air is brought into the lungs by development of negative pressure within the pleural cavities.
|
|
|
(Describe ventilation)
Innervation |
»Each half of the diaphragm is innervated by a phrenic n. which arises from ventral rami C3-5 (mostly C4).
»Phrenic nn. therefore course through the neck where they rest on the anterior surfaces of the (i)anterior scalenes and (ii)thorax, where each lies b/w mediastinal pleura and parietal pericardium. |
|
|
(Describe ventilation)
Articulations |
»Except for the articulation between the first costal cartilage and the sternum (which is a synchondrosis), the ribs articulate with the vertebrae and with the sternum at synovial joints.
»Accordingly, ventilatory movements are readily permitted at these joints. |
|
|
(Describe ventilation)
Joint ventilating movements |
»Analysis of movements at the costotransverse joints suggests that:
1) Upper ribs - carry the sternum anteriorly during inspiration, increasing the A-P dimension of the chest via a so called "pump-handle" mechanism. 2) Lower ribs - flare out during inspiration, increasing the lateral dimension of the chest via a so called "bucket-handle" mechanism. |
|
|
(Describe ventilation)
How is quiet inspiration achieved? |
»Quiet inspiration is largely accomplished by contraction of the diaphragm, a dome-like sheet of skeletal muscle that tends to flatten as it contracts.
Thus: 1) Diaphragm (produces 80-85% of tidal volume) 2) Scalenes (Note: anterior & middle scalenes attach 1st rib, where posterior attaches at 2nd rib). 3) Parasternal (internal) intercostals |
|
|
(Describe ventilation)
How is forced inspiration achieved? |
"Forced inspiration" is achieved by the 3 "quiet inspiration" structures PLUS the following accessory mm of inspiratory ventilation:
1) Upper trapezius 2) Sternocleidomastoid 3) Scapular stabilizers* 4) Serratus posterior superior 5) Levators costarum |
|
|
(Describe ventilation)
Scapular stabilizers |
E.g. (i)Levator scapulae, (ii)rhomboids, and (iii)trapezius.
Note: Postures typically assumed by runners who are short of breath after a race or by patients with chronic obstructive pulmonary disease »They tend to lean forward slightly and prop their upper limbs on something to stabilize and elevate their scapulae. |
|
|
(Describe ventilation)
Rapid inspiration |
»Tracheal cartilages help to prevent collapse of the airway during rapid inspiration.
|
|
|
(Describe ventilation)
Expiration: Passive and Forced. |
»Expiration is usually a "passive" process associated with elasticity of the lungs and chest wall.
»During forced expiration, (i)abdominal mm. assist in increasing intra-abdominal and intrathoracic pressures which force air out of the lungs. »(ii)Serratus posterior inferior probably also contributes. »Consider the importance of the coughing mechanism to patients with pulmonary disease. |