![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
Ipsilateral Reciprocal Inhibition:
|
Good thing:
SAME SIDE: -Co-contraction: Stimulation to both limb F and E muscles which stabilize a joint (restrict movement) -RI about a joint: Flexor group contracts, and extensor group is reciprocally inhibited (relaxes)
|
|
|
Contralteral Reciprocal Inhibition |
GOOD thing:
OPPOSITE SIDE: -Ipsilateral flexor contraction triggers reflex inhibition of the contralateral flexor -Increased contraction causes increased RI = the harder the muscle contracts, the more it inhibits its antagonist -Sustained contraction on an agonist (such as this a chronic facilitated state) causes inhibition of the antagonist, which becomes weakened |
|
|
cc: |
a tight, sustained hypertonic muscle will inhibit both the ipsilateral antagonist, as well as the contralateral agonist |
|
|
Slow-twitch muscle
|
HIPRATT slowly twitched and tighted
Upper-crossed Syndrome
-Oxidative metabolism
-High capillary density (red color)
-Tonic/postural functioning
-shorten and tighten when disturbed |
|
|
Fast Twitch muscle
|
FAST, VAST, ASS
Lower-crossed Syndrome
-Glycolytic metabolism
-Low capillary density (white color)
-Fatigue rapidly
-Dynamic/Phasic function
-weaken when disturbed |
|
|
Upper Crossed Syndrome (shoulder girdle) |
-Tonic/Postural muscles facilitated: Levator scapulae, Upper trap, SCM, Scalenes, Pectorals, Flexors of UE ***Remember that Tonic/Postural muscles get tight
WEAK: hypotonic -Dynamic/Phasic muscles inhibited: Middle/lower trap, Serratus anterior, Rhomboids, Supraspinatus, Infraspinatus, Deltoid, Deep neck flexors, Extensors of UE
|
|
|
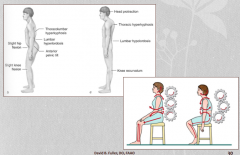
Lower Crossed Syndrome (pelvic girdle) |
Characteristics: Dynamic/Phasic -Weak glutes : Tight/Short hip flexors -Weak abdominals : Tight/Short thoraco-lumbar extensors -Anterior pelvic tilt and Increased lumbar lordosis -Hypermobility at L4-S1 -Difficult sitting up from supine (forward flexion)
weak: butt |
|
|
Psoas |
Tonic/Postural: Slow twitch; get tight when disturbed
Sx: Hip flexed, T12-L2 dysfunction, facilitation
Tx: Lumbar tenderpoints, ME to lengthen psoas, home stretches |
|
|
Piriformis |
Tonic/Postural: Slow twitch; get tight when disturbed
|
|
|
Hamstrings |
Tonic/Postural: Slow twitch; get tight when disturbed |
|
|
Upper Trapezius* |
Upper Crossed Syndrome Postural/Tonic: Slow twitch; shorten and tighten when disturbed
"Facilitated" |
|
|
Lower Trapezius* |
Upper Crossed Syndrome Dynamic/Phasic: Fast twitch; weaken when disturbed
"Pseudoparesis"/ hypotonic |
|
|
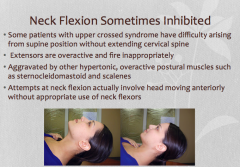
Neck Flexors |
|
|
|
Normal sequence of muscle firing patterns in hip extensions*** |
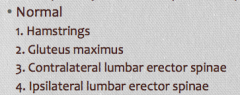
Normal firing pattern is most efficient and effective use of muscles
|
|
|
Abnormal sequence of muscle firing patterns in hip extensions** |
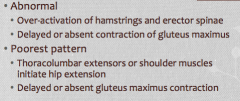
Abnormal firing patterns compensate and still accomplish the required motion, but in a dysfunctional way
Leads to: 1)Anterior Pelvic Tilt 2) Lumbar hyperlordosis with hip extension 3)Inability to maintain knee extension 4)Hypertonic hamstrings, thoracolumbar extensors 5)Atrophy of gluteus maximus |
|
|
What postural changes emerge from crossed syndrome dysfunctional patterns |
|
|
|
Design proper treatment sequences for patients presenting with symptoms related to underlying muscle imbalances |
-Core retraining: balance and proprioceptive training (standing on one foot)
-Stretch: lengthen the hypertonic postural muscles
-Activate and strengthen previously inhibited dynamic/phasic muscles after realigned
-Gentle aerobic exercise |
|
|
How do tonic/postural muscles respond to dysfunction? |
Facilitation, hypertonicity, shortening. |
|
|
How do dynamic/phasic muscles respond to dysfunction? |
Inhibited, hypotonic, and weak (PSEUDOPARESIS) |