![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
13 Cards in this Set
- Front
- Back
|
Maintenance dosing |
Goal is to reach and maintain target "steady state" plasma concentration (Css) in therapeutic range. Can apply to continuous intravenous infusion, intravenous interval dosing, or oral interval dosing. |
|
|
What is time to steady state dependent on? |
Dependent only on half life. This is called the "plateau principle". |
|
|
How much of steady state concentration is reached after 1, 2, 3, and 4 half lives? |
1 - 50% 2 - 75% 3 - 87.5 4 - 93.75 |
|
|
What is the effect of varying rate of infusion or half life on steady state concentration? |
Steady state concentration is directly proportional to rate of infusion and half-life and inversely proportional to clearance. Remember that time to steady state is dependent only on half life. |
|
|
Concept of loading dose |
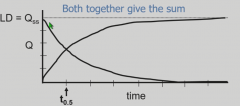
Since can take too much time to reach steady state with constant infusion, can administer a loading dose at the steady state concentration that decays at the same rate (dependent on half life) that the infusion takes to reach steady state. Works for constant infusion and intermittent dosing. |
|
|
Difference between IV and Oral doses |
Fluctuations of concentration in oral dose are blunted and cannot be estimated with simple model. Can estimate fluctuations from intermittent IV dosing. |
|
|
What happens to maintenance dosing or loading dose if bioavailability is less than 100%? |
Would have to be adjusted upwards |
|
|
If dose interval is equal to half life, then what is the fluctuation for intermittent IV doses? |
Qmax/Qmin = 2 There would be a two-fold fluctuation in plasma concentration |
|
|
Adjustments to maintenance dosing using renal function |
Monitor renal dysfunction and renal drug clearance by declining creatinine clearance (CLcr) |
|
|
Adjustments to maintenance dosing using hepatic function |
Induction of liver enzymes or impairment of live metabolism have unpredictable effects on hepatic drug clearance - no simple formula |
|
|
Cockroft-Gault formula |
Estimates creatinine clearance from measu red level of serum creatinine. Takes into account age, ideal body weight (adjusted downwards for obese patients), and serum creatinine. |
|
|
Dose-adjustment factor for renally-excreted drug for patient with renal insufficiency |
Dose adjustment factor = Creatinine clearance of patient / Normal creatinine clearance |
|
|
Applying dose adjustment factor to maintenance dosing regimen |
Adjusted dose = usual dose x DAF Adjusted interval = usual interval/DAF |