![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
68 Cards in this Set
- Front
- Back
|
Circulating blood is divided: |
45% cells: rbc, wbc, and platelets (aid in coag) 55% plasma |
|
|
Hematology |
diagnosis, monitoring and treatment of anemias, leukemias, and clotting disorders |
|
|
EDTA |
The only anticoag that doesnt destroy the composition |
|
|
Hematopoiesis |
the production of blood cells |
|
|
Multipotential cell |
give rise to all blood cells from multipotential cells arise stem cells stem cells proliferate and differentiate into the different cell lines |
|
|
Bone marrow |
Major center for hematopoiesis |
|
|
Lab tests done in Clinical Hematology |
1. counting the number of cells 2. determining the relative distribution of various types of cells 3, measuring biochemical abnormalities of the blood 4. determining abnormal appearance of cells |
|
|
Erythrocytes |

red blood cells |
|
|
Leukocytes |
white blood cells |
|
|
Thrombocytes |
platelets |
|
|
Reticulocytes |
young rbc |
|
|
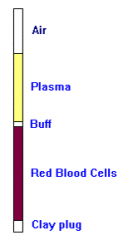
Normal blood |
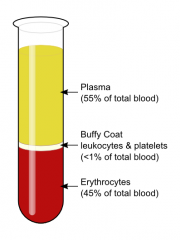
when whole blood stands components settle into 3 layers -sample should be mixed a min of 15 inversion before sampling |
|
|
Buffy coat |
wbc and platelets |
|
|
Erythrocytes |
-round, bioconcave -no nucleus or organelles -avg diameter: 7 um -life span: 120 days -90% of rbc is made up of hemoglobin |
|
|
Hemoglobin |
transport oxygen and remove metabolic waste |
|
|
Central pallor |
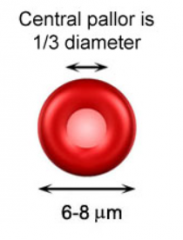
pallor is the concave portion and it is in one third of the cell |
|
|
Erythropoietin |
stimulates rbc production produced mostly in kidney and minimally in the lover |
|
|
Anemia |
-condition where either the number of rbcs or the amount of hemoglobin is below normal -rbc doesnt provide enough O2 to tissues |
|
|
anemia due to low rbc are classified by cause |
- excessive blood loss (trauma, bleeding) -defective hematopoiesis ( aplastic, low iron, low B12/folate) -excessive hemolysis (intravascular trauma) |
|
|
Hemoglobinopathies |
disorders of hemoglobin such as sickle cell or thalassemia |
|
|
test for anemia: RBC count |
-count the number of rbc per volume of blood -done by automated analyzers called cell counters -or done manually by using counting chamber called hemocytometers |
|

test for anemia: cyanmethemoglobin method |
-test done for hemoglobin concentration -uses Drabkin's reagent ( potassium ferricyanide and potassium cyanide) 1. lyses rbcs 2. potassium ferricyanide oxidizes iron in hemoglobin forming methemoglobin 3. potassium cyanide combines with methemoglobin to form cyanmethemoglobin 4. coloured complex is formed and measured spectrophotometrically (amt of colour= amt of Hb) |
|
|
test for anemia: Hematocrit |
-also known as Packed Cell Volume (PCV) -the amount of space rbcs take up in the blood -centrifuged to separate cellular components and then determine portion containing rbcs |
|
|
White cell count (WBC) |
the count of the number of white cells per volume of blood |
|
|
Leukocytosis |
- high wbc count it can be: - Reactive: secondary to infection, inflammation -Neoplastic: leukemia, lymphomas |
|
|
Leukopenia |
-low wbc count caused by: -radiation, chemo treatment -immune disorders -medications toxins |
|
|
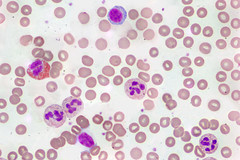
Leukocytes |

- characterized by number of nuclei present and granules in the cytoplasm - divided into : 1. Polymorphonuclear Granulocytes: -Neutrophils -Eosinophils -Basophils 2. Mononuclear Agranulocytes : -Monocytes -Lymphocytes |
|
|
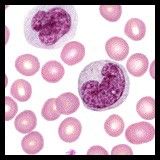
Polymorphonuclear Granulocytes: Neutrophils |
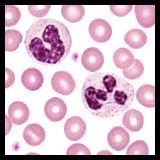
- Function: engulfs bacteria (phagocytosis) and cellular debris -light pink granules in cytoplasm -Contain a multilobed nucleus - 37-77% |
|
|
Polymorphonuclear Granulocytes: Eosinophils |
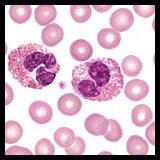
- Function: parasitic infections, allergic response -large, reddish granules in the cytoplasm -Have a characteristic bi-lobed nucleus and a cytoplasm that is packedwith large granules of uniform size - 1-7% |
|
|
Polymorphonuclear Granulocytes: Basophils |
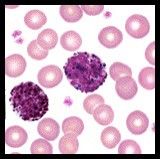
-hypersensitivity, release Histamine (mast cells in tissue) -large dark blue/purple granules in cytoplasm - 0-1.6% |
|
|
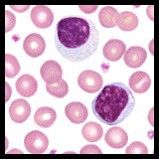
Mononuclear Agranulocytes: Monocytes |
- engulf cellular debris, antigen processing (becomes macrophages) - largest member of the white blood cell family. Theyare easily identified by a large nucleus that has the shape of a horseshoe - no granules - 2-10% |
|
|
Mononuclear Agranulocytes: Lymphocytes |
-produces antibodies, regulate the immune response - largest nucleus -light blue cytoplasm -no granules - 10-44% |
|
|
WBC source of production: Myeloid |
-WBC can be characterized by source of production -Myeloid: made in bone marrow *Neutrophils *Basophils *eosinophils *monocytes |
|
|
WBC source of production: Lymphoid |
- produced and stored in lymph tissue: - B-Lymphocytes - T-Lymphocytes |
|
|
B-Lymphocytes |
produces antibodies as part of humoral response |
|
|
T-Lymphocytes |
- helper or killer cells - directly destroy as part of cell mediated response |
|
|
Leukemia |
- malignant proliferation of cells of the blood and bone marrow any cell type can be involved but usually classified as: -Myelogenous (myeloid): involving granulocytes and their precursors -Lymphocytic (lymphoid): involving the lymphocytes and their precursors |
|
|
Leukemia: acute or chronic |
Acute: sudden onset, fatal w/in 2-3 months if intreated chronic: slower onset, survival 3-10 years if treated Malignant lymphomas: Hodgkin's disease, non- Hodgkin's lymphoma Plasma cell dyscrasias: MM (multiple myeloma), heavy chain disease, macroglobulinemia |
|
|
Can MLTs diagnose Leukemia |
Yes,we will be able to tell by looking at the slides.But we cannot tell the patients |
|
|
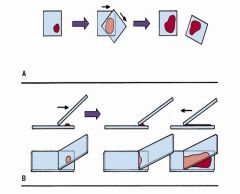
A: Coverglass Blood films B: Wedge Blood films |
|
|
|
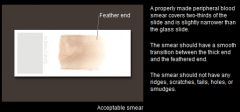
Properly made blood smear |
|
|
|
Staining the blood smear Wright's stain |
Wright's stain: consists of absolute methanol, eosin, and methylene blue |
|
|
Wright's stain: Absolute methanol |
fixes blood cells to the glass slide |
|
|
Wright's stain: Eosin |
is negatively charged and stains basic objects red |
|
|
Wright's stain: Methylene blue |
reacts with phosphate buffer (pH 6.6-6.8) and stains acidic objects blue |
|
|
correct interpretation of a blood film requires |
1. correct preparation of the blood film 2. proper staining 3. accurate examination we look for WBCs |
|
|
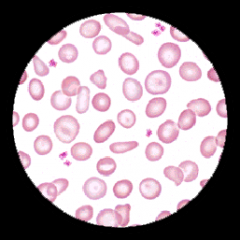
Examining the RBCs for alteration and variations |
Variation in colour or staining: Normochromic- normal color Hypochromia- increase in area of central pallor hyperchromia- dec in area of central pallor |
|
|
Examining the RBCs for Anisocytosis |
meaning alteration in size aniso: from greek word for unequal Macrocytosis- large rbcs microcytosis- small rbcs |
|
|
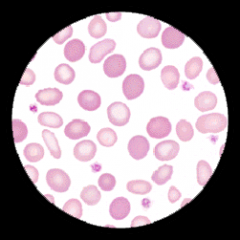
Hypochromic |
decreased hemoglobin concentration in pale cells |
|
|
Normochromic |

normal area of central pallor should be about 1/3 of the cell's diameter |
|
|
Anisochromia |
Pale and filled cells can both be seen following blood transfusion |
|
|
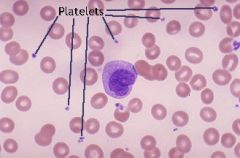
Morphologic changes (platelet count) |
estimate platelet count and evaluate normally 6 to 20 platelets per oil immersion field rep a normal platelet of 150-450 |
|
|
Morphologic changes: Differential count of white cells |

-Determine the fraction of each wbc type - individual level of each types of wbc helps to determine diseases -minimum of 100 consecutive wbc are counted, classified, and reported as precentages of total wbc counted |
|
|
How to identify WBC |
identification based on differences in: -nucleus -nucleolus -cytoplasm |
|
|
Hemostasis |
- sub discipline of hematology - hemostasis: the ending of blood flow from an injured vessel or the process whereby the body retains the blood within the vascular system |
|
|
Thrombocytes |
-platelets (thrombo) required for normal hemostatasis |
|
|
Thrombocytosis |
increased platelets |
|
|
Thrombocytopenia |
decreased platelets can result in: -Petechiae -Purpura it can result from many condition and is associated with heparin therapy, DIC, deep vein thrombosis, cerebralthrombosis, MI, alcoholic liver disease, etc -severe morbidity and mortality |
|
|
Petechiae |

small purplish hemorrhage spots on skin |
|
|
Purpura |

extensive areas of red, dark purple discoloration |
|
|
Coagulation (clotting) |
-mechanism that allows plasma proteins, coagulation factors, tissue factors, and calcium (factor IV) to work together on the surface of platelets to form a fibrin clot -nonfunctioning factor leads to hemorrhaging |
|
|
Hemophilia A Hemophilia B Von Willebrand Disease |
Lab coag tests for which factors are not functioning •Hemophilia A: FactorVIII:C, Antihemophilic factor (AHF) •Hemophilia B: FactorIX •Von WillebrandDisease: FactorVIII:vWFt |
|
|
Bleeding time |
-perform a capillary puncture and measure time required for bleeding to stop -it is a screening test for platelet defects |
|
|
Bleeding time: Positive |
-meaning elevated BT -positive in vWD, thrombocytopenia purpura, capillary inferiority, aspiring ingestion |
|
|
Bleeding time: normal |
normal in hemophilia, other clotting disorders |
|
|
PT (Prothrombin Time) |
-a screening test for defects in coagulation cascade - measures function of extrinsic pathway -used to monitor Warfarin, Coumadin (blood thinners) therapy ( example: to prevent post operative thrombosis, pulmonary embolism) |
|
|
APTT (Activated Partial Thromboplastin Time) |
-a screening test for defects in coagulation cascade -measures function of intrinsic pathway (elevated in hemophilia) -used to monitor patients on heparin therapy |
|
|
What tube is required for PT and APTT test? |
blue top tube |