![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
24 Cards in this Set
- Front
- Back
|
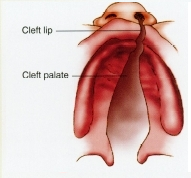
Cleft |
areopenings that pass through one or more structures that are normally closed
|
|
|
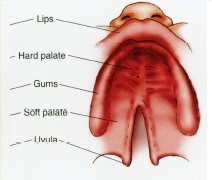
Hard Palate |
fused of two bones |
|
|
Velum |
Thevelum hangs down in the back of the oral cavity at the juncture of theoropharynx and the nasopharynx. |
|
|
Types of Cleft |
-Unilateral -Bilateral -Complete -Incomplete -Submucous Cleft -Congenital Palatopharyngeal Incomplete |
|
|
Unilateral Cleft |
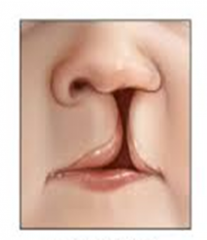
onone side of the nose |
|
|
Bilateral Cleft |
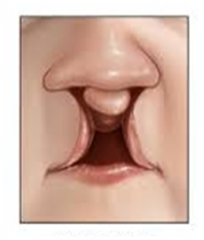
on both sides of the nose |
|
|
Complete Cleft |
-the two palatal shelves aretotally separated. |
|
|
Incomplete Cleft |
-the shelves are partially fused. |
|
|
Submucous Cleft |

the palate appears normal becausethe tissue covering the palate hides a cleft of the hard palate, the softpalate, or both. |
|
|
Congenital Palatopharyngeal Incomplete |
no cleft of any kind
-A condition in which the velopharyngealmechanism is not adequate to achieve velopharyngeal closure because: -Thenasopharynx is too deep, -or the hard palate is too short. -Musclesare of adequate bulk but still do not function to close the velopharyngealport. |
|
|
Craniofacial Anomalies |
abnormalities of the skull and face;
-facial clefts are a part ofthese anomalies. |
|
|
Nasal Emissions |
-friction noise created by the stream of air rushing out of the nasal passage.
|
|
|
Feeding/Swallowing Problems associated with Clefts |
-inadequate velopharyngeal mechanism, the opening in the hard palate, and a deformed upper lip create feeding problems. -food and fluids enter nasal cavity. -proper instructed, mothers are able to handle the feeding problems by careful and patient feeding. |
|
|
Hearing Impairment Problems associated with Clefts |
-Children suffer from otitis media (middle ear disease) -fluctuating mild to moderate hearing problem known as conductive hearing loss, cause language delay and speech problems. |
|
|
Dental Problems associated with Clefts |
Children with clefts of the alveolar ridge have more dental problems than do children with cleft of the hard and soft palates. -most common abnormalities include malocclusion, insufficient growth of the teeth and the gum tissue (hypoplasia), cross bite, protruding premaxilla in case of bilateral cleft, and the growth of extra teeth. |
|
|
Language Problems associated with Clefts |
-slow acquisition of language -smaller and less varied vocabulary -shorter and simpler sentences -limited spontaneous speech -delayed answers to questions -grammatical errors |
|
|
Articulation Problems associated with Clefts |
-distorted speech sounds -omission of speech sounds -substitution of speech sounds -nasal emission -Achild’s (or an adult’s) attempt to produce speech sounds in unusual ways(because of an organic defect) is called compensatory articulation. |
|
|
Pharyngeal flap Surgery |
-secondary operation may be necessary for children with wide and complete clefts. -who still have an inadequate velopharyngeal mechanism. -In this procedure, a muscular flap is raised from the back wall of the throat and attached to the velum. The flap helps close the velopharyngeal port |
|
|
Pharyngoplasty Surgery |
-changes the shape of the velopharyngeal space -surgeon makes incisions along each side of the throat in order to create two flaps of tissue. -pulled up and attached to the sides and back of the throat. -permanent ring of tissue that lines the walls of the upper throat and makes the velopharyngeal space smaller creates two holes near the sides of the throat for air to pass through, sphincter pharyngoplasty creates one hole in the middle of the throat surrounded by the new ridge of tissue. As the soft palate elevates during speech, it will make contact with this ridge to close the smaller velopharyngeal space. This procedure tends to work best for patients who have good soft palate movement and poor movement of the side walls of the upper throat. |
|
|
Cleft Palate Team |
-Agroup of specialists,plan and implement a treatment and rehabilitative program -plasticsurgeon -speech–languagepathologist -dentist -orthodontist -otologist(medically trained ear specialist) -audiologist -psychologist -pediatrician -socialworker -educationalspecialists |
|
|
Treatment of Language Disorder |
Slight delays in language, corrected by home language stimulation programs the parents conduct. -formal treatment, SLP uses language structures the child is not able to produce, including words, phrases, sentences, and aspects of syntax and morphological elements, are trained with standard procedures |
|
|
Treatment of Articulation Disorder |
directing the flow of air out of the mouth instead of the nose -producing speech with less force making gentle contact of articulators -opening the mouth wider during speech production -help reduce nasal resonance -treating the articulation disorders of the child with a cleft are not different from those described in Chapter 5. -maximum visual and auditory cues to the child, -teaches the sounds that are produced in the front of the mouth (e.g., /p/ and/b/) and then those produced in the back of the mouth (/k/ and /g/). In gradual steps, the training is shifted to more complex levels, including words,phrases, sentences, and conversational speech. |
|
|
Treatment of Voice and Resonance Problems |
-socially appropriate loudness and relaxed speech are targeted -to compensate for the inadequate velopharyngeal mechanism. -talk too softly or with excessive muscular effort to close the velopharyngealport. |
|
|
Treatment of Hypernasality Problems |
-clinician develops practice trials starting with the least nasal sounds and moving on to the most nasal sounds.The sounds are eventually produced in words and phrases. -Biofeedback instruments, such as the Nasometer, maybe used in treatment.
|