Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
276 Cards in this Set
- Front
- Back
|
Pneumonia- general characteristics
1. two types |
1. Community-acquired - occurs in the community setting or within 72 hours of hospitalization. Can be typical or atypical. Most common bacterial pathogen is S. Pneumoniae
2. Nosocomial pneumonia- occurs during hospitalization after first 72 hours. Most common bacterial pathogens are gram negative rods (E. coli, pseudomonas) and s. aureus |
|
|
Two recommended methods of prevention for pneumonia
|
1. Influenza vaccine- give yearly to people at increased risk for complications and to health care workers
2. pneumococcal vaccine- for patients > 65 years and younger people at high risk (those with heart disease, sickle cell disease, pulmonary disease, diabetes, alcoholic cirrhosis or asplenic individuals) |
|
|
Typical Community Acquired Pneumonia (CAP)
1. common agents 2. symptoms |
1. s. pneumo (60%), h. flu (15%), aerobic gram-negative rods (6-10%), klebsiella (and other enterobacteriaceae), S. aureus (2-10%).
2. Acute onset of fever and shaking chills, cough productive of thick, purulent sputum. Pleuritic chest pain (suggests pleural effusion), dyspnea |
|
|
Signs of typical CAP (pneumonia)
|
1. tachycardia
2. tachypnea 3. late inspiratory crackles, bronchial breath sounds 4. increased tactile and vocal fremitus 5. dullness to percussion 6. pleural friction rub (if pleural effusion) |
|
|
Chest xray findings in typical CAP - pneumonia
|

1. lobar consolidation
2. multilobar consolidation is indicative of very serious illness |
|
|
Atypical Community-Acquired Pneumonia - common agents
|
1. Mycoplasma pneumoniae (most common),
2. chlamydia pneumoniae, 3. chlamydia psittici, 4. coxiella burnetii (Q fever), 5. legionella spp., 6. viruses - influenza (A and B), adenoviruses, parainfluenze, RSV |
|
|
Clinical features (signs and symptoms) of atypical CAP - pneumonia
|
1. symptoms - insidious onset - headache, sore throat, myalgias, dry cough, fever (chills are uncommon)
2. signs - pulse- temperature dissociation - normal pulse in the setting of high fever is suggestive of atypical CAP. Wheezing, rhonchi, crackles |
|
|
Chest x-ray appearance in atypical pneumonia
|

1. diffuse reticulonodular infiltrates
2. absent or minimal consolidation |
|
|
Diagnosis of pneumonia
|
1. PA and lateral CXR required to confirm diagnosis
- considered sensitive- if CXR findings are not suggestive of PNA, do NOT treat the patient with antibiotics - after treatment, changes evident on CXR usually lag behind clinical response by up to 6 weeks - changes include interstitial infiltrates, lobar consolidation and/or cavitation. - false-negative CXRs occur with neutropenia, dehydration, infection with PCP and early disease (< 24 hours) 2. pretreatment expectorated sputum for gram stain and culture- low sensitivity and specificity, but still worthwhile tests because antimicrobial resistance is an increasing problem |
|
|
If vital signs are entirely normal, what is the probability of pneumonia in outpatients?
|
less than 1%
|
|
|
What does "atypical" pneumonia refer to?
|
organisms not culturable on standard blood agar
|
|
|
A patient presents with a sudden chill followed by fever, pleuritic chest pain and a productive cough. What is the likely diagnosis?
|
Community-acquired pneumonia (CAP) - typical
|
|
|
What is the pathophysiology of most cases of community-acquired pneumonia?
|
aspiration of oropharyngeal secretions as the majority of organisms that cause CAP are normal inhabitants of the pharynx
|
|
|
What are the three most common causes of bacterial pneumonia?
|
1. S. pneumoniae - up to 66%
2. H. influenza 3. legionrlla spp. |
|
|
What is the general approach to the diagnosis of CAP?
|
- the first task is to differentiate lower respiratory tract infection from the other causes of cough and from upper respiratory infection
- If nasal discharge, sore throat or ear pain predominates then URI is more likely - one Lower respiratory tract infection is suspected, the next task is to differentiate between pneumonia and acute bronchitis. Unfortunately, clinical features (cough, sputum, fever etc) are no reliable in differentiating the two - CXR is the only reasonable method of differentiating pneumonia from acute bronchitis |
|
|
The value of sputum culture in CAP
|
- the value of gram stain and culture is controversial. It should probably be performed in ALL patients HOSPITALIZED for CAP
- a good sputum specimen has > 25 PMNS and <10 epithelial cells per low power field - commonly contaminated with oral secretions - a good specimen has sensitivity of 60% and specificity of 85% for identifying gram-positive cocci in chains (S. pneumo) |
|
|
What steps should be taken in patients admitted to the hospital with suspected pneumonia?
|
1. CXR (PA and lateral)
2. laboratory tests - CBC with diff, BUN, creatinine, glucose, electrolytes 3. O2 saturation 4. two pretreatment blood cultures from different sites- positive in 5-15% of cases 5. gram stain and culture of sputum 6. antibiotic therapy - consider antibiotic sensitivities |
|
|
What type of pneumonia should you think of...
a. in alcoholics? b. in immigrants c. nursing home residents d. HIV-positive patients e. organ tranplant patients, patients with renal failure, patients with chronic lung disease and smokers |
a. Klebsiella pneumonia
b. TB c. nosocomial pathogens and predilection for upper lobes (pseudomonas) d. Pneumocystis carinii (PCP) and mycobacterium tuberculosis-- but still more likely to have typical infectious agent e. Legionella pneumonia- rare in healthy children and young adults |
|
|
Special stains for diagnosis pneumonia etiologic agent?
|
1. acid fast stain- mycobacterium spp- if TB is suspected
2. silver stain (fungi, PCP) for HIV, immunocompromised patients |
|
|
Lab test for legionella pneumophila?
|
urinary antigen assay - this test is very sensitive. The antigen persists in the urine for weeks (even after treatment has started)
|
|
|
Decision to hospitalize in treatment of CAP
|
- most important decision and is based on severity, stratified into five classes based on the Pneumonia Severity Index-- but clinical judgement reigns
- if hypoxic or hypotensive then hospitalize - look at labs (pH, electrolytes), comorbid illnesses, physical exam (AMS, RR, SBP, temp, HR), age, resident of nursing home? - the higher the number/score the higher the mortality and thus the need to hospitalize. generally classes III-V should be hospitalized |
|
|
Antimicrobial therapy for the treatment of CAP
|
- because the specific agent is usually not determined on initial exam, empiric therapy is often required
- in people younger than 60- the most common agents are s. pneumo, mycoplasma, chlamydia and legionella. Macrolides (azithromycin or clarithromycin) or doxycycline cover all these organisms and are first line. Fluoroquinolones are alternatives. Penicillins and cephalosporins do NOT cover the atypical organisms in this age group - in older adults and patients with comorbidities (more likely to have typical CAP) or those treated with antibiotics in the last 3 months, a fluoroquinolone is the first-line agent (levofloxacin, moxifloxacin). A second or third line generation cephalosporin is second line - for outpatients -- treatment is continued for five days. Do NOT stop treatment until the patient has been afebrile for 48 hours!!! |
|
|
General antibiotic guideline for treatment of uncomplicated CAP
1. no comorbidities 2. with comorbidities |
1. azithromycin or clarithromycin
2. fluoroquinolone (levofloxacin, moxifloxacin) |
|
|
Antibiotic therapy for patients hospitalized with pneumonia
|
A fluoroquinolone alone (levofloxacin) or a third generation cephalosporin plus a macrolide (ceftriaxone plus azithromycin)
|
|
|
Treatment of hospital-acquired pneumonia
|
1. Treatment is tailored toward gram-negative rods (any of the following 3 are appropriate)
a. cephalosporins with pseudomonal coverage: ceftazidime or cefepime b. carbapenems: imipenem c. piperacillin/tazobactam (zosyn) 2. Macrolides are NOT used (as they are in CAP) |
|
|
Complications of pnemonia
|

1. pleural effusion - "parapneumonic effusion" - can be seen in more than 50% of patients with CAP on routine CXR. Empyemia is infrequent in these patients. Most of these effusions have an uncomplicated course and resolve with antibiotic treatment of the pneumonia. Thoracentesis should be performed if the effusion is significant ( >1 cm on lateral decubitus film). Send fluid for gram stain, culture, pH, cell count, glucose, protein and LDH
2. pleural empyema (loculated pleural fluid) occurs in 1-2% of all cases of CAP and up to 7% of hospitalized patients with CAP 3. acute respiratory failure may occur in severe cases |
|
|
Ventilator-Associated Pneumonia
1. why at increased risk 2-3. findings to aid with the diagnosis 4. treatment (3 options) |
1. Patients on mechanical ventilation are at risk for developing pneumonia because the normal mucociliary clearance of the respiratory tract is impaired (cannot cough)
2. Findings to help with diagnosis: new infiltrate on CXR, purulent secretions from the endotracheal tube, fever, rising WBC count 3. Bronchoalveolar lavage (BAL)- bronchoscope passed into the lungs to get cultures 4. Treatment is a combination of the following three different drugs: a. cephalosporin (ceftazidime or cefepime) OR penicillin (piperacillin/tazobactam-- zosyn) b. aminoglycoside OR fluoroquinolone c. vancomycin or linezolid |
|
|
Lung abscess- general characteristics
1. definition |
1. Abscess in the lung parenchyma results when infected lung tissue becomes necrotic and forms suppurative cavitary lesions. The typical case is aspiration of a large volume of oropharyngeal contents or food, with resulting pneumonia and necrosis when adequate treatment is not administered. Most patients who aspiration pneumonia treated promptly and adequately do NOT develop an abscess
- by definition a lung abscess is formed by one or more cavities each > 2 cm in diameter |
|
|
An lung abscess can develop as a consequence of what 4 things?
|
1. aspiration of organisms
2. acute necrotizing pneumonia (gram-negative rods) 3. hematogenous spread of infection from distant site 4. direct inoculation with continguous spread |
|
|
What types of bacteria usually cause lung abscesses
|
Mainly bacteria that colonize the oropharynx
a. oral anaerobes - prevotella, peptostreptococcus, fusobacterim, bacteriodes spp b. other bacteria- S. aureus, S. pneumo, and aerobic gram-negative bacilli |
|
|
Epidemiology and risk factors for lung abscesses
|
1. the main risk factor is predisposition to aspiration. This may be seen in patients with alcoholism, drug addiction, CVA, seizure disorders, general anesthesia, or NG or endotracheal tubes
2. poor dental hygiene increases the content or oral anaerobes 3. endentulous patients are less likely to aspirate oropharyngeal secretions |
|
|
Clinical features of lung abscesses
|

1. The majority of cases have an indolent course, some present more acutely
2. Common symptoms and signs- cough- foul-smelling sputum consistent with anaerobic infection. It is sometimes blood tinged. SOB, fever, chills, constitutional symptoms (fatigue, weight loss, malaise) |
|
|
Diagnosis of lung abscess
|

1. CXR- this reveals thick-walled cavitation with air-fluid levels. Look for abscess in dependent, poorly ventilated lobes
2. CT scan may be necessary to differentiate between abscess and emypyema 3. Sputum gram stain and culture have low specificity and sensitivity 4. consider obtaining cultures via bronchoscopy or transtracheal aspiration rather than simple expectoration to avoid contamination with oral flora |
|
|
Treatment of lung abscess
|
1. Hospitalization is often required if lung abscess is found. Postural drainage should be performed
2. Antimicrobial therapy- antimicrobial regimens include coverage for the following: gram-positive cocci- ampicillin or amoxicillin-clavulanic acid, ampicillin/sulbactam, or vancomycin for S. aureus - anaerobes - clindamycin or metronidazole - if gram-negative organisms are suspected, add a fluoroquinolone or ceftazidime b. continue antibiotics until the cavity is gone or until CXR findings have improved considerably-- this may take months |
|
|
Tuberculosis - general characteristics
1. Microbiology 2. Transmission |
1. Most commonly caused by mycobacterium tuberculosis. Mycobacteria are acid-fast bacilli (AFB) - considered slow-growing but hardy organisms. Inhibited by the cellular arm of the immune system.
2. transmissions occurs via inhalation of aerosolized droplets containing the active organism. Only those people with active TB are contagious (e.g. by coughing or sneezing). People with primary TB are not contagious. |
|
|
Pathophysiology of tuberculosis- primary TB
|
1. Primary tuberculosis- bacilli are inhaled and deposited into the lung, then ingested by alveolar macrophages
- surviving organisms multiple and disseminate via lymphatics and bloodstream. Granulomas form and "wall off" the mycobacteria. Being in oxygen-rich areas allows the organisms to remain viable as they are aerobes. After the resolution of the primary infection, the organism remains dormant within the granuloma - any insult to the immune system may activate TB at any time - only 5-10% of individuals with primary TB develop active disease within their lifetime |
|
|
What is the most common cause of death due to infection worldwide?
|
Tuberculosis
|
|
|
Secondary TB
|
REACTIVATION
- occurs when the host's immunity is weakened (e.g. HIV infection, malignancy, immunosuppressants, substance abuse, poor nutrition) - usually manifests in the most oxygenated portions of the lungs-- the apical/posterior segments - produces clinical manifestations of TB - can be complicated by hematogenous or lymphatic spread, resulting in miliary TB |
|
|
Extrapulmonary tuberculosis
|
- individuals with impaired immunity may not be able to contain the bacteria at either the primary or the secondary state of the infection
- this may result in active disease throughout the body - it is common in patients with HIV because their cellular (t-cells) immunity is impaired |
|
|
Risk factors for TB infection
|
1. HIV positive patients
2. recent immigrants (within the past 5 years) 3. prisoners 4. health care workers 5. close contacts of someone with TB 6. alcoholics 7. diabetics 8. glucocorticoid use 9. hematologic malignancy 10. injection drug users |
|
|
Clinical features of TB
1. primary 2. secondary (active) |
1. primary- usually asymptomatic, pleural effusion may develop. If the immune response is incomplete, the pulmonary and constitutional symptoms of TB may develop. This is known as primary progressive TB
2. Secondary (active TB) - constitutional symptoms (fever, night sweats, weight loss and malaise), cough progresses from dry cough to purulent sputum. Hemoptysis suggests advanced TB. Apical rales may be present on exam |
|
|
Clinical features of extrapulmonary TB
|
- may involve ANY organ. The lymph nodes, pleura, GU tract, spine, intestine and meninges are some of the common sites of infection
- Miliary TB refers to hematogenous dissemination of the tubercle bacilli. May be due to reactivation of dormant, disseminated foci or a new infection. Also common in patients with HIV. May present with organomegaly, reticulonodular infiltrates on CXR, and choroidal tubercles in the eye |
|
|
Diagnosis of TB
|

1. CXR
2. Sputum studies (sputum acid-fast testing) 3. Tuberculin skin test (PPD test) - must have a high index of suspicions, depending on the patients risk factors * more notes on all of these tests in subsequent cards |
|
|
What makes the diagnosis of TB so difficult in HIV patients?
|
1. PPD skin test result is negative- because the portion of the immune system necessary to make a positive response is defective (type IV - delayed cell mediated hypersensitivity response- depends on T cells-- this is what the PPD takes 48-72 hours to turn positive)
2. patients have atypical CXR findings 3. sputums mears are more likely to be negative 4. granuloma formation may not be present in the late stages |
|
|
CXR findings in TB
|

- classic findings are upper lobe infiltrates with cavitations
- may see pleural effusions, Ghon's and Ranke's complexes- evidence of healed primary TB (- Ghon's complex- calcified primary focus with an associated lymph node - Ranke's comples- when Ghon's complex undergoes fibrosis and calcification) - atypical findings common in immunocompromised patients |
|
|
Sputum studies in diagnosis of TB
|
- definitive diagnosis is made by sputum culture- growth of m. tuberculosis
- obtain three morning sputum specimens- culture takes 4-8 weeks - PCR can detect specific mycobacterial DNA more rapidly - diagnosis is sometimes made by finding acid fast bacteria (AFB) on microscopic examination, but this is not definitive because other mycobacteria may colonize the airways |
|
|
Tuberculin (PPD) skin test
|
1. a tuberculin skin test is a screening test to test those who have been exposed to TB. It is not for a diagnosis of active TB, but rather latent (primary) TB (if positive, a CXR is used to diagnose active TB). PPD is not a screening test for everyone, only patinets with one or more risk factors. If patient is symptomatic or has abnormal CXR then order a sputum acid-fast test, not a PPD
- Inject PPD into the volar aspect of the forearm then measure the amount of induration 48-72 hours later. Cutoffs for a positive result differ depending on the patient |
|
|
PPD positive cutoffs
1. no risk factors 2. high risk population 3. immunocompromised |
1. For a patient with no risk factors : induration > 15 mm
2. high risk population (those who live in high-prevalence areas, immigrants in the last 5 years, homeless, prisoners, health care workers, nursing home resident, etc): induration > 10 mm 3. For patients with HIV, steroid users, organ transplant recipients, close contacts of those with active TB, or those with radiographic evidence of TB: induration > 5 mm is positive |
|
|
If patient has never had a PPD test before and they test negative, what should be done?
|
Repeat the test in 1-2 weeks as the first test may be a false negative. The results of the second test are used for management
|
|
|
What should be done when a patient has a positive PPD?
|
A CXR is needed to rule out active disease. Once active disease is excluded, 9 months of isoniazid treatment is initiated. A patient with a positive PPD has a 10% lifetime risk of TB, and this risk is reduced to 1% after after 9 months of INH
|
|
|
PPD and the Bacille Calmette-Guerin (BCG)vaccine
|
- Many persons born outside the US have been BCG-vaccinated, which may cause a positive PPD test, however this does NOT affect treatment decisions
- If a patient has a positive PPD test, isoniazid for 9 months is indicated, even if the patient had a prior BCG vaccine |
|
|
Treatment of active TB
|
1. Patients with active TB must be isolated until sputum is negative for AFB
2. First line therapy is a four-drug regimen: RIPE- Rifampin, Isoniazid, Pyrazinamide, Ethambutol or streptomycin 3. The initial treatment regimen consists of 2 months of the 4-drug regimen. After the initial 2-month phase, then 4 months of INH and rifampin is recommended |
|
|
Prophylactic Treatment for latent (primary TB)
|
- positive PPD
- treat with 9 months of INH AFTER active TB has been excluded by negative CXR, sputum or both |
|
|
What organ is most at risk with TB medications and what should be done about this?
|
- All TB medications can cause hepatotoxicity
- discontinue treatment only if liver transaminases rise to 3-5 times the upper limit of normal - limit other hepatotoxic drugs including alcohol |
|
|
Influenza- etiologic agent and types
|
- orthomyxovirus is transmitted via respiratory droplets, typically occurring during the winter months
- antigenic types A and B are responsible for the clinical syndrome known as the "flu" - annual epidemics are due to minor genetic reassortment and usually not life-threatening except in the very young, the very old, immunocompromised, and hosts with significant medical commorbidities - rarely occurring pandemics are due to major genetic recombination (shift) and often fatal even in young, otherwise healthy host |
|
|
Clinical findings of influenza
|
- rapid onset of fever, chills, malaise, headache, non-productive cough and sore throat
- nausea may also be present |
|
|
treatment of influenza
|
- treatment is largely supportive.
- antiviral agents are available but these are only indicate in patients with severe disease (requiring hospitalization) or at high risk of complication. Give abx only for secondary bacterial infections. - a neuraminidase inhibitor (zanamivir or oseltamivir) is the recommended antiviral agent if one is indicated |
|
|
Clinical features/triad of acute bacterial meningitis
|
1. fever
2. nuchal rigidity (stiff neck) 3. AMS |
|
|
Meningitis - definition
|
1. This refers to inflammation of the meningeal membranes that envelope the brain and spinal cord. It is usually associated with infectious causes, but non-infectious causes (such as medications, SLE, sarcoidosis and carcinomatosis) also exist.
|
|
|
Meningitis - pathophysiology
|
1. infectious agents frequently colonize the nasopharynx and respiratory tract
2. These pathogens typically enter the CNS via one of the following. a. invasion of the bloodstream, which leads to hematogenous seeding of the CNS b. retrograde transport along cranial (e.g. olfactory) or peripheral nerves c. contiguous spread from sinusitis, otitis media, surgery or trauma |
|
|
Classification of meningitis
|
1. acute or chronic- depending on the onset of symptoms
- acute meningitis - onset within hours to days - chronic meningitis- onset within weeks to months; commonly caused by mycobacteria, fungi, Lyme disease, or parasites |
|
|
Causes of acute bacterial meningitis by age group
1. neonates 2. children > 3 months 3. adults (18-50) 4. elderly (> 50) 5. Immunocompromised |
1. Group B strep, E. coli, Listeria
2. N. meningitidis, S. pneumo, H. influenza, 3. S. pneumo, N. meningitidis, H. influenza 4. S. pneumo, N. meningitidis, L. monocytogenes 5. L. monocytogenes, gram-negative bacilli, s. pneumo |
|
|
Complications of acute bacterial meningitis
|
- seizures, coma, brain abscess, subdural empyema, DIC, respiratory arrest
- permanent sequelae- deafness, brain damage and hydrocephalus |
|
|
Aseptic meningtis
|
- aseptic meningitis is caused by a variety of nonbacterial pathogens, frequently viruses such as enterovirus and herpes simplex virus (HSV). It can also be caused by certain bacteria, parasites and fungi
- it may be difficult to distinguish it clinically from acute bacterial meningitis. If there is uncertainty in the diagnosis, treat for acute bacterial meningitis - It is associated with a better prognosis than acute bacterial meningitis |
|
|
Clinical features of meningitis- signs and symptoms
|

1. symptoms - headache (may be more severe when lying down), fevers, nausea/vomiting, stiff/painful neck, malaise, photophobia, altered mental status (confusion, lethargy, coma)
2. signs- nuchal rigidity (stiff neck with resistance to flexion of the spine), rashes (maculopapular rash with petechiae--purpura is classic for N. meningitidis), vesicular lesions in varicella or HSV, increased ICP and its manifestations - e.g. papilledema, seizures. Cranial nerve palsies. Kernig's sign- inability to fully extend the knees when the patient is supine with hips flexed (90 degrees) - caused by irritation of the meninges, only present in approximately half of patients with bacterial meningitis |
|
|
Kernig's sign
|
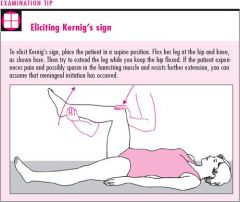
sign of meningitis
- inability to fully extend the knees when the patient is supine with hips flexed (90 degrees) - caused by irritation of the meninges, only present in approximately half of patients with bacterial meningitis - if sign is positive bilaterally it is more suggestive of meningeal irritation |
|
|
Brudzinski's sign
|
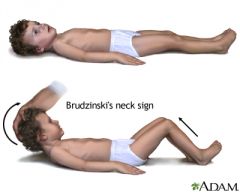
- sign of meningeal irritation
- flexion of the legs and thighs that is brought about by passive flexion of the patient's neck - present in half of patients with bacterial meningitis |
|
|
Diagnosis of meningitis
|
1. CSF Examination - LP - perform this if meningitis is a possible diagnosis unless there is evidence of a space-occupying lesion. Also note the opening pressure
a. examine the CSF. Cloudy CSF is consistent with pyogenic leukocytosis. CSF chould be sent for the following: cell count, chemistry (e.g. protein, glucose), gram stain, culture (including AFB) and cryptococcal antigen or India Ink 2. CT scan of the head is recommended before performing an LP if there are focal neurologic signs or if there is evidence of a space-occupying lesion with elevations in ICP 3. Obtain blood cultures before antibiotics are given |
|
|
CSF findings in acute bacterial meningitis
|
Pyogenic inflammatory response in CSF
- elevated WBC count - PMNs predominate - low glucose - high protein - gram stain- positive in 75% to 80% of patients with bacterial meningitis |
|
|
CSF findings in aseptic meningitis
|
Non-pyogenic inflammatory response in CSF
- there is an increase in mononuclear cells. Typically a lymphocytic pleocytosis is present - protein is normal or slightly elevated - glucose is usually normal - CSF may be completely normal |
|
|
Treatment of bacterial meningitis
|
1. Empiric antibiotic therapy- start immediately after LP is performed. If a CT scan must be performed or if there are anticipated delays in LP, give antibiotics first
2. IV antibiotics- initiate immediately if CSF is cloudy or if bacterial infection is suspected. begin empiric therapy according to the patient's age (e.g. adult -- ceftriaxone + vancomycin + ampicillin) 3. Steroids- of cerebral edema is present 4. Vaccination - vaccinate all adults > 65 yo for S. pneumoniae. Vaccinate asplenic patients for S. pneumo, N. meningitidis and H. flu (capsulated bugs). Vaccinate all ICH for n. meningitidis 5. Prophylaxis- (rifampin or ceftriaxone) - for all close contacts of patients with meningococcus, give 1 dose of IM ceftriaxone (rocephin) |
|
|
Treatment of aseptic meningitis
|
1. No specific therapy other than supportive care is required. The disease is self-limited
2. analgesics and fever reduction is appropriate |
|
|
Encephalitis - general characteristics
1. definition 2. general causes 3. risk factors 4. mortality |
1. diffuse inflammation of the brain parenchyma and is often seen simultaneously with meningitis
2. usually viral in origin. Non-viral causes must also be considered 3. Risk factors - AIDS (patients are at risk for toxoplasmosis when the CD4 count is < 200), other forms or immunosuppression, travel in underdeveloped countries, exposure to insect (mosquito) vector in endemic areas, exposure to certain wild animals (e.g. bates) in an endemic area for rabies 4. the overall mortality associated with viral encephalitis is approximately 10% |
|
|
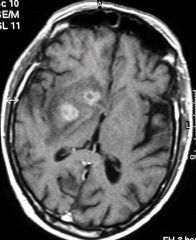
Causes of encephalitis
1. viral 2. nonviral infectious 3. Noninfectious causes |
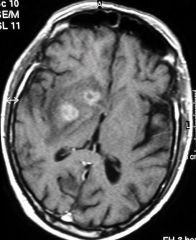
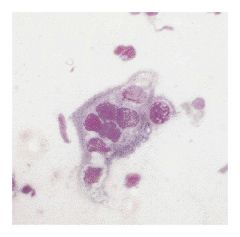
1. viral causes: HSV-1, arbovirus (e.g. eastern equine encephalitis, West nile virus), enterovirus (e.g. polio), less commonly: measles, mumps, EBV, CMV, VZV, rabies and prion diseases such as Cruetzfeldt-Jakob disease (spongiform encephalopathy)
2. toxoplasmosis, cerebral aspergillosis 3. metabolic encephalopathies, T-cell lymphoma * pic- toxoplasmosis* |
|
|
Differential diagnosis for patients with fever and altered mental status
|
1. sepsis, UTI/urosepsis, pneumonia, bacterial meningitis, intracranial abscess, subdural empyema
2. neuroleptic malignant syndrome (haloperidol, phenothiazines) 3. Delirium tremens 4. thyroid storm |
|
|
Clinical features of encephalitis
|
1. patients often have a prodrome of headache, malaises and myalgias
2. within hours to days, the patients become more acutely ill 3. patients frequently have signs and symptoms of meningitis (headache, fever, photophobia, nuchal rigidity) 4. patients often have altered sensorium, possibly confusion, delirium, disorientation, and behavior abnormalities 5. focal neurologic findings (hemiparesis, aphasia, cranial nerve lesions) and seizures may also be present |
|
|
Diagnosis of encephalitis
|
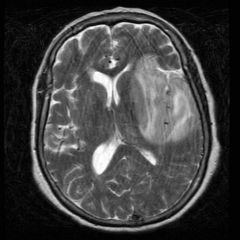
1. Routine laboratory tests (to rule out nonviral causes) include CXR, urine and blood cultures, urine toxicology screen and serum chemistries
2. Perform LP to examine CSF, unless the patient has signs of significantly increased ICP a. lymphocytosis (> WBC/mL) with normal glucose is consistent with viral encephalitis (similar CSF as in viral meningitis). CSF cultures are usually negative. CSF PCR is the most specific and sensitive test for diagnosing many various viral encephalitides, including HSV-1, CMV, EBV and VZV 3. MRI of the brain is the imaging study of choice. Can rule out focal neurologic causes such as abscess. Increased areas of T2 signal in the frontotemporal localization are consistent with HSV encephalitis 4. EEG can be helpful in diagnosing HSV-1 encephalitis- it would show unilateral or bilateraly temporal lobe discharges 5. brain biopsy is indicated in an acutely ill patient with a focal, enhancing lesion on MRI without a clear diagnosis * HSV encephalitis-pic* |
|
|
Treatment of encephalitis
|
1. Supportive care, mechanical ventilation if necessary
2. antiviral therapy - there is no specific antiviral therapy for most causes of viral encephalitis. HSV encephalitis-- acyclovir for 2-3 weeks, CMV encephalitis- ganciclovir or foscarnet) 3. Management of possible complications a. seizures- require anticonvulsant medications b. cerebral edema - treatment may include hyperventilation, osmotic diuresis and steroids |
|
|
Viral Hepatitis - general characteristics
1. definition 2. causes |
1. hepatitis simply means inflammation of the liver. There are many noninfectious types of hepatitis, such as alcoholic, drug-induced, and autoimmune hepatitis.
2. There are five well-understood, main categories of viral hepatitis. Hepatitis A, B, C, D, E. Other viruses that can cause one form or another of hepatitis are EBV, CMV, and HSV. These are not commonly associated with hepatitis in immunocompetent patients. |
|
|
Diseases associated with...
1. Hepatitis B 2. Hepatitis C |
1. Hep B- Polyarteritis Nodosa
2. Hep C- cryoglobulinemia |
|
|
Transmission methods
1. Hepatitis A 2. Hepatitis B 3. Hepatitis C 4. Hepatitis D 5. Hepatitis E |
1. Hep A- fecal-oral. More prevalent in developing countries
2. Hep B- parenterally and sexually. Perinatal transmission is also possible and is a significant health problem in parts of Africa and Asia 3. Hep C- main route of transmission is parenteral, and it is therefore most prevalent in IV drug users. Sexual and perinatal transmission are not common 4. Hep D- requires the outer envelope of HBsAg for replication and therefor can be transmitted only as a co-infection with HBV, or as a superinfection in a chronic HBV carrier 5. Hep E- fecal-oral. More prevalent in developing countries, especially India, Pakistan, Southeast Asia and parts of Africa |
|
|
Which types of hepatitis can progress to chronic disease
|
Hepatitis B, C, and D
|
|
|
Difference between acute and chronic viral hepatitis
|
Acute (< 6months of liver inflammation) or chronic (> 6 months of persistent liver inflammation)
|
|
|
General clinical features of acute viral hepatitis
|

- acute hepatitis can have a wide spectrum of clinical presentations, ranging from virtually asymptomatic to fulminant liver failure
- jaundice- look first in the sclera, because this may be the first place jaundice is detected, especially in black patients - dark-colored urine may be present (due to conjugated hyperbilirubinemia) - RUQ pain - nausea/vomting - fever and malaise - hepatomegaly may also be present - sometimes acute hepatitis may only presents with transient flu-like symptoms such as fever, myalgias and malaise. - Hep C does NOT typically cause a significant acute illness - Acute HBV may also present with serum sickness |
|
|
In severe cases, acute hepatitis can result in liver failure and it complication. This is known as fulminant hepatitis and is uncommon. What types of hepatitis is it most common in and what are its complications?
|
* this may be life-threatening
- complications include: hepatic encephalopathy- look for asterexis and palmar erythema. - hepatorenal syndrome - bleeding diathesis- this occurs only when liver function is very compromised |
|
|
Chronic hepatitis - clinical features
2. risk of chronic hepatitis in hep b and c 3. categorization of hepatitis severity 4. risk of developing cirrhosis and HCC with hep B and C |
- this has a wide variety of presentations
1. some patients are asymptomatic chronic carriers and may only present with late complications of hepatitis, such as cirrhosis or hepatocellular carcinoma (HCC) 2. Chronic hepatitis occurs after acute hepatitis in 1-10% of patients with HBV and > 80% of patients with HCV 3. It is categorized based on the grade of inflammation, stage of the fibrosis and etiology of the disease 4. The risk of developing cirrhosis or HCC is 25-40% in patients with chronic HBC and 10-25% in patients with chronic HCV |
|
|
Diagnosis of viral hepatitis
|
1. Serum serology- the presence of serum antigens and immunoglobulins is the most important factor in diagnosing viral hepatitis. There are helpful in determining the acuity or chronicity of illness as well as adequate immunity
2. PCR is used to detect viral RNA to diagnose HCV 3. LFTS- elevation of serum transaminases is NOT diagnostic, but LFTs are helpful. ALT is typically more elevated that AST in all forms of viral hepatitis (in contrast to alcoholic hepatitis). In acute hepatitis ALT is usually > 1,000. It is generally not as high as in drug-induced hepatitis. In chronic HBV, ALT can also be >1,000 but this varies. In chronic HCV, ALT is generally lower than this |
|
|
Treatment of viral hepatitis
|
1. Active (vaccine) and passive (immunoglobulin) immunization are available for both hepatitis A and B. It is the standard of care for infants and health care workers to be vaccinated for HBV
2. Travelers are often vaccinated for HAV. Passive immunization can be given for people who are exposed to the virus 3. Treatment for hep A and E is supportive 4. Chronic HBV- treatment with interferon-alpha. Alternatively, treat with lamivudine (nucleoside analogue) 5. Chronic HCV- treat with interferon alpha and ribavirin 6. Consider liver transplantation in advanced disease, although recurrence can occur after transplantation |
|
|
If liver transaminases are markedly elevated (>500) what diagnoses should you think of?
|
1. acute viral hepatitis
2. shock liver 3. drug-induced hepatitis |
|
|
Botulism - general characteristics
1. Causes |
- results from ingestion of preformed toxins produced by spores of Clostridium botulinum. Improperly stored food (e.g. home-canned foods) can be contaminated with these spores. Toxins can be inactivated by cooking food at high temperatures (e.g. 100 deg C for 10 minutes)
- wound contamination is another source |
|
|
Clinical features of botulism
|
- the severity of the illness ranges widely, from mild, self-limiting symptoms to rapidly fatal disease
- abdominal cramps, nausea, vomiting, and diarrhea are common - the hallmark clinical manifestation is symmetric, DESCENDING flaccid paralysis. - It starts with dry mouth, diplopia, and/or dysarthria. Paralysis of limb musculature occurs later |
|
|
Diagnosis of botulism
|
- The definitive diagnosis is identification of the toxin in serum, stool, or gastric contents (bioassay)
- Identifying C. botulinum alone in food is not a reliable diagnostic indicator |
|
|
Treatment of botulism
|
1. Admit the patient and observe respiratory status closely. Gastric lavage is helpful within several hours after ingestion of suspected food
2. If suspicion of botulism is high, administer antitoxin (toxoid) as soon as laboratory specimens are obtained (do not wait for results) 3. For contaminated wounds- in addition to the above- wound cleansing and penicillin |
|
|
Differential diagnosis of food-borne botulism
|
1. Gullain- Barre syndrome- characteristically ASCENDING paralysis, but on variety (FIscher) can be descending
2. Lambert-Eaton syndrome 3. Myasthenia gravis - EMG studies differentiate 4. Diptheria 5. Tick paralysis |
|
|
Intra-abdominal abscess
- causes - diagnosis - treatment |
- causes include spontaneous bacterial peritonitis, pelvic infection (tubo-ovarian abscess), pancreatitis, performation of the GI tract, and osteomyelitis of the verterbral bodies with extension into the retroperitoneal cavity
- usually polymicrobial in origin - diagnose using CT scan or ultrasound - Treatment typically involves drainage of the abscess - The antibiotic regimen should include broad coverage against gram-negative rods, enterococci and anaerobes |
|
|
Urinary Tract Infections- general characteristics
1. epidemiology 2. cause 3. common organisms |
1. UTIs are much more common in women than men (because of their short urethra). Up to 33% of all women experience a UTI in their lifetime. the most common UTI is uncomplicated acute cystitis
2. The majority of UTIs are caused by ascending infection from the urethra. Colonization the vaginal arena by pathogens from the fecal clora leads to ascension via the urethra into the bladder 3. common organisms- E. coli (the most common- 80% of cases). Other organisms- S. saphrophyticus, Enterococcus, Klebsiella, Proteus spp., pseudomonas, enterobacter and yeast (such as Candida spp) |
|
|
Risk factors for UTI
|
1. Female gender- greater risk due to the shorter female urethra and vaginal colonization of bacteria
2. sexual intercourse - often the trigger of a UTI in women- thus the term is "honeymoon cystitis". Use of diaphragms and spermicides increases the risk further by altering vaginal colonization 3. Pregnancy 4. indwelling urinary catheter- risk factor for hospitalized patients 5. personal history of recurrent UTIs 6. Host-dependent factors - increase the risk for recurrent or complicated UTIs - diabetes (risk for upper UTI), patients with spinal cord injury, immunocompromised state, any structural or functional abnormality that impeded urinary flow (e.g. incomplete voiding, neurogenic bladder BPH, vesicourethral reflux, calculi). - male risk factors- uncircumsized - bacterial colonization of the foreskin, anal intercourse, vaginal intercourse with a female colonized with uropathogens |
|
|
Clinical features of UTIs
|
1. dysuria - commonly expressed as burning on urination
2. frequency 3. urgency 4. suprapubic tenderness 5. gross hematuria is sometimes present 6. in lower UTIs, fever is characteristically ABSENT |
|
|
Diagnosis of UTI - dipstick UA
|
1. Dipstick urinanalyis - positive for urine leukocyte esterase test- presence of leukocyte esterase reflects pyuria. Positive nitrite test for presence of bacteria (gram-negative) - nitrite test is sensitive and specific for detecting Enterobacteriacceae. But it lacks sensitivity for other organisms, so a negative test should be interpreted with caution. Combining leukocyte esterase plus nitrites yields a sensitivity of 85% and specificity of 75%
|
|
|
Diagnosis of UTI - UA (clean-catch midstream specimen)
|
1. adequacy of collection- the presence of epithelial (squamous) cells indicates vulvar or urethral contamination. If contamination is suspected, perform a straight cath of bladder
2. Criteria for UTI: Bacteriuria > 1 organism per oil-immersion field. Bacteriuria without WBCs may reflect contamination and is not a reliable indicator of infection. Pyuria is the most valuable finding for diagnosis: greater than or equal to 10 leukocytes/microliter is abnormal - other findings - hematuria and mild proteinuria may be present. Hematuria in and of itself does not require extended therapy |
|
|
Urine gram stain -diagnosis of UTI
|
- a count of > 10^5 organisms/mL represents significant bacteriuria
- it is 90% sensitive and 88% specific |
|
|
Urine Culture - diagnosis of UTI
|
- confirms the diagnosis (high specificity). Obtaining a urine culture if symptoms are not characteristic of a UTI, if a complicated infection is suspected, or if symptoms persist despite prior antibiotic treatment
- traditional criteria: >/= 10^5 CFU/mL of urine from a clean-catch sample. Misses up to 1/3 of UTIs - colony counts as low as 10^2 to 10^4 CFU/mL are adequate for diagnosis if clinical symptoms are present - |
|
|
Diagnosis of UTI - blood cultures
|
- only indicated if the patient is ill and urosepsis is suspected
|
|
|
Diagnosis of UTI - IVP, cystoscopy, and excretory urography
|
NOT recommended unless a structural abnormality or obstruction is suspected
- if there are recurrent UTIs in a man this may be indicated |
|
|
Complicated UTI - definition
|
- Any UTI that spreads beyond the bladder (e.g. pyelonephritis, prostatitis, urosepsis) - risk factors for upper UTI infection: pregnancy, diabetes, and vesicoureteral reflux
- Any UTI caused by structural abnormalities, metabolic disorder, or neurologic dysfunction |
|
|
UTI during pregnancy
|
- increased risk of preterm labor (PTL), low birth weigh, and other complications, especially in advanced pregnancy
|
|
|
Recurrent UTIs
|
- usually due to infection with new organism, but sometimes is a relapse due to unsuccessful treatment of the original organism
- risk factors include impaired host defenses, pregnancy, vesicourethral reflux and sexual intercourse in women - generally the consequences are not significant unless the patient is at risk for upper UTI |
|
|
Treatment of uncomplicated cystitis (i.e. nonpregnant women)
|
1. Oral TMP/SMX : Bactrim for 3 days (1st line)
2. Nitrofurantoin: Macrobid (5-7 days) - do not give if early pyelonephritis is suspected. 3. Fosfomycin (single dose) - do not give if early pyelo is suspected 4. amoxicillin- less popular due to increasing abx resistance 5. fluoroquinolones- (ciprofloxacin 3 day regimen) is a reasonable alternative 6. treat presumptively for pyelonephritis if the condition fails to respond to a short course of antibiotics 7. Pyridium (phenazopyridine) is a urinary analgesic- it can be given for 1-3 days for dysuria- turns urine orange |
|
|
Treatment of UTI in pregnant women
|
1. Treat with amoxicillin, ampicillin or oral cephalosporins for 7-10 days
2. Avoid fluoroquinolones (can cause fetal arthropathy) |
|
|
Treatment of UTIs in men
|
- treat as with uncomplicated cystitis in women, but for 7 days
- perform a urologic workup if there are complications or recurrences, or if the initial treatment fails |
|
|
Recurrent UTIs
|
- If a relapse occurs within 2 weeks of cessation of treatment, continue treatment for 2 more weeks and obtain a urine culture
- Otherwise treat as for uncomplicate cystitis. If the patient has two or more UTIs per year, give chemoprophylaxis (single dose of TMP/SMX after intercourse or at the first signs of symptoms- or low dose prophylactic abx: Bactrim for 6 months) |
|
|
Pyelonephritis - general characteristics
|
1. an infection of the upper urinary tract. It is usually caused by ascending spread from the bladder to the kidney. Uncomplicated pyelonephritis is limited to the renal pyelocalyceal-medullary region. Vesicoureteral reflux facilitates this ascending spread.
|
|
|
Organisms responsible for pyelonephritis
|
1. E. coli (most common cause)
2. other gram-negative bacteria include Proteus, Klebsiella, Enterobacter and Pseudomonas 3. gram-positive bacteria (less common) include enterococcus faecalis and S. aureus |
|
|
Complications of pyelonephritis
|
- unusual
- sepsis occurs in 10-25% of patients with pyelonephritis. May lead to shock. - emphysematous pyelonephritis- caused by gas-producing bacteria in diabetic patients - chronic pyelonephritis and scarring of the kidneys- rare unless underlying renal disease exists |
|
|
Clinical features of pyelonephritis
1. symptoms 2. signs |
1. fever, chills, flank pain, symptoms of cystitis (+/-), nausea, vomiting, diarrhea (sometimes)
2. fever with tachycardia, patients generally appear more ill than patients with cystitis, CVA tenderness - unilateral or bilateral, abdominal tenderness may or may not be present |
|
|
Diagnosis of pyelonephritis
|
1. urinalysis- look for pyuria, bacteriuria, and leukocyte CASTS. As in cystitis, hematuria and mild proteinuria may be present
2. urine cultures- obtain in all patients with suspected pyelonephritis 3. blood cultures- obtain in ill-appearing patients and hospitalized patients 4. CBC- leukocytosis with left shift 5. Renal function- this is usually preserved. Impairment is usually reversible, especially with IV fluids 6. Imaging studies- perform these if treatment fails or in any patient with complicated pyelonephritis. Consider renal ultrasound, CT, IVP, or retrograde ureterogram |
|
|
Treatment of uncomplicated pyelonephritis
|
1. use outpatient treatment if the patient can take oral antibiotics- treat based on gram-stain:
- TMP/SMX (bactrim) or fluoroquinolone for 10-14 days is effective for most gram-negative rods. - amoxicillin is appropriate for gram-positive cocci (enterococci, S. saphrophyticus) - a single dose of cetriaxone or gentamycin if often given initially before starting oral treatment 2. repeat urine culture 2-4 days after cessation of therapy 3. If symptoms fail to resolve within 48 hours, adjust treatment based on urine culture 4. failure to respond to appropriate antimicrobial therapy suggests a functional or structural abnormality, perform a urologic investigation |
|
|
Treatment of pyelonephritis in a patient who is very ill, elderly, pregnant, unable to tolerate oral medication or has significant comorbidities-- or if urosepsis is suspected
1. first step in management 2. initial abx choices 3. if blood cultures are negative 4. if blood cultures are positive |
1. Hospitalize and give IV fluids
2. Treat with antibiotics - start with parenteral antibiotics (broad-spectrum) - ampicillin plus gentamycin or ciprofloxacin are common initial choices 3. If blood cultures are negative, treat with IV abx until the patient is afebrile for 24 hours, then give oral abx to complete a 14-21 day course 4. if blood cultures are positive (urosepsis), treat with IV antibiotics for 2-3 weeks |
|
|
Treatment of recurrent pyelonephritis
|
1. if relapse is due to the same organism despite appropriate treatment, treat for 6 weeks
2. if relapse is due to a new organism, treat with appropriate therapy for 2 weeks |
|
|
Prostatitis - general characteristics - acute bacterial prostatitis
|
1. less common than chronic bacterial prostatitis
2. occurs more commonly in younger men 3. Pathophysiology- ascending infection from the urethra and reflux of infected urine 4. may occur after urinary catheterization 5. other causes- direct of lymphatic spread from the rectum 6. hematogenous spread (rare) 7. gram-negative organisms predominate (e.g. E. coli, klebsiella, proteus, pseudomonas, enterobacter, serratia) |
|
|
General characteristics of chronic bacterial prostatitis
|
- more common than acute bacterial prostatitis, true prevalence is difficult to determine because many cases are asymptomatic and are diagnosed incidentally
- it most commonly affects men 40-70 years of afe - it has the same routes of infection as acute bacterial prostatitis. It may develop from acute bacterial prostatitis - organisms are similar to those in acute prostatitis (gram-negative organisms predominate (e.g. E. coli, klebsiella, proteus, pseudomonas, enterobacter, serratia) |
|
|
Clinical features of acute bacterial prostatitis
|
- fever, chills- patient may appear toxic
- irritative voiding symptoms- dysuria, frequency and urgency are common - perineal pain, low back pain, and urinary retention may be common as well |
|
|
Clinical features of chronic prostatitis
|
- patients may be asymptomatic. Patients do not appear ill. Fever is uncommon.
- patients frequently have recurrent UTIs with irritative voiding and/or obstructive urinary symptoms - there is dull, poorly localized pain in the lower back, perineal, scrotal or suprapubic region |
|
|
Diagnosis of prostatitis
|
1. Digital rectal exam - boggy and exquisitely tender in acute disease. in chronic disease, the prostate is enlarged and usually non-tender
2. UA- numerous (sheets of) WBCs are present in acute bacterial prostatitis 3. urine cultures- almost always positive in acute prostatitis 4. Chronic prostatitis - the presence of WBCs in expressed prostatic secretions suggests diagnosis. Urine cultures may be positive (chronic bacterial prostatitis) or negative (nonbacterial prostatitis) 5. obtain CBC and blood cultures if patient appears toxic or if sepsis if suspected |
|
|
Treatment of acute prostatitis
|
1. If it is severe and the patient appears toxic, hospitalize the patient and initiate IV antibiotics
2. if it is mild, treat on an outpatient basis with antibiotics - bactrim or a fluoroquinolone and doxycycline. treat for 4-6 weeks. the patient usually responds to therapy |
|
|
Treatment of chronic prostatitis
|
- treat with a fluoroquinolone. For chronic bacterial prostatitis, a prolonged course is recommended but does NOT guarantee complete eradication
- it is difficult to treat. recurrences are common. Recurrent UTIs are very common in these patients |
|
|
Acute vs chronic prostatitis
|
1. acute prostatitis is a more serious condition and urgent medical treatment is necessary
2. acute prostatitis is much more clinically obvious (fever, exquisitely tender prostate), whereas chronic prostatitis is difficult to diagnosis because the prostate may not be tender and findings are variable |
|
|
When doing an exam in a patient that has suspected acute bacterial prostatitis, what must be avoided?
|
prostatic massage so as to avoid triggering bacteremia. Rectal exam may be skipped entirely if the diagnosis is straightforward.
|
|
|
What is the most common bacterial STD?
|
Chlamydia - it is an intracellular organism
|
|
|
Chlamydia- general characteristics
|
1. most common bacterial STD. It is an intracellular organism
2. Many patients are co-infected with gonorrhea (up to 40% of women and 20% of men) 3. The incubation period if 1 to 3 weeks |
|
|
Clinical features of Chlamydia
|
1. many cases are asymptomatic (80% of women and 50% of men)
2. men who are symptomatic may have any of the following: dysuria, purulent urethral discharge, scrotal pain and swelling, and fever 3. Women who are symptomatic may have purulent urethral discharge, intermenstrual bleeding or postcoital bldding, and dysuria |
|
|
Diagnosis of chlamydia
|

1. Diagnostic tests include culture, enzyme immunoassay, and molecular tests such as PCR. Serologic tests are not used for Chlamydia
2. Molecular diagnostic tests are replacing culture as the screening test of choice due to higher sensitivity 3. sexually active adolescents (particularly females) should be screened for chlamydia infection even if they are asymptomatic |
|
|
Treatment of chlamydia
|
1. Azithromycin (oral one dose) or doxycycline (oral for 7 days)
2. Treat all sexual partners |
|
|
Gonorrhea - general characteristics
|
1. The responsible organism is Neisseria gonorrheae (a gram negative, intracellular diplococcal organism)
2. Gonorrhea is usually asymptomatic in women but symptomatic in men. Therefore complications more often occur in women due to undetected disease 3. it is almost always transmitted sexually (with the exception of neonatal transmission) 4. Co-infection with Chlamydia trachomatis is common (30% of patients) -- more common in women |
|
|
Clinical features of gonorrhea
1. in men 2. in women 3. disseminated gonococcal infection |

1. Gonorrhea is asymptomatic in up to 10% of carriers. These asymptomatic carriers can still transmit the disease. Most men have symptoms involving the urethra - e.g. purulent discharge, dysuria, erythema and edema of the urethral meatus, and frequency of urination
2. women- most women are asx. Women may have symptoms of cervicitis or urethritis - e.g. purulent discharge, dysuria, intermenstrual bleeding and dyspareunia. 3. disseminated disease- occurs in 1-2% of cases and is more common in women. Possible findings: fever, arthralgias, tenosynovitis (of hands and feet), migratory polyarthritis/septic arthritis, endocarditis or even meningitis. Skin rash (usually on distal extremities) |
|
|
Diagnosis of gonorrhea
|
1. gram stain of urethral discharge showing organisms within leukocytes is highly specific for gonorrhea
2. obtain cultures in all cases- in men from the urethra, in women from the endocervix. May treat empirically because culture results take 1-2 days to return 3. consider testing for syphillis and HIV 4. Obtain blood cultures if disease is disseminated |
|
|
Treatment of gonorrhea
|
1. Ceftriaxone (IM, one dose) is preferred because it is also effective against syphillis. Other options are oral cefixime, ciprofloxacin, or ofloxacin
2. ALSO GIVE AZITHROMYCIN (one dose) or doxycycline (for 7 days) to cover coexistent chlamydial infection 3. If disseminated, hospitalize the patient and initiate ceftriaxone (IV or IM for 7 days) |
|
|
HIV and AIDS- pathophysiology
|
1. The most common virus associated with HIV is the HIV type 1 human retrovirus.
2. The virus attaches to the surface of CD4+ T lymphocytes (targets HIV-1), it enters the cell and uncoats, and its RNA is transcribed to DNA by reverse transcriptase 3. Billions of viral particles are produced each day by activated CD4 cells. When the virus enteres the lytic stage of infection, CD4 cells are destroyed. It is the depletion of the body's arsenal of CD4 cells that weakens the cellular immunity of the host |
|
|
Transmission of HIV
|
- usually sexual or parenteral. Other than semen and blood, fluids that transmit the disease are breast milk and vaginal fluid
- risk of transmission: needle stick - 1 in 300, vaginal (male to female) - 1 in 1,000, vaginal (female to male) - 1 in 3,000, anal receptive - 1 in 100, moth to child - 1 in 3 without medications. With medications the risk is 2 in 100. Caesarian delivery is indicated if viral load is over 1,000 copies. If CD4 count is high (over 500) and viral load is low (under 1,000), c-section is not necessary |
|
|
HIV - mortality and high risk individuals
|
1. mortality is usually secondary to opportunistic infection, wasting or cancer
2. High-risk individuals: homosexual or bisexual men IV drug abusers, blood transfusion recipients before 1985, heterosexual contacts of HIV positive individuals, unborn and newborn babies of HIV positive mothers |
|
|
Clinical features of HIV/AIDS
1. primary infection 2. asymptomatic infection |
1. Primary infection - a mononucleosis-like syndrome about 2-4 weeks after exposure to HIV. Duration of the illness is brief (3 days to 2 weeks).
- symptoms include fever, sweats, malaise, lethargy, headaches, arthralgias/myalgias, diarrhea, sore throat, lymphadenopathy, and truncal maculopapular rash 2. asymptomatic infection (seropositive but no clinical evidence of HIV infection). CD4 counts are normal (> 500/mm3), longest phase (lasts 4-7 years but varies widely, especially with treatment) |
|
|
Clinical features of HIV - symptomatic HIV infection (pre-AIDS)
|
1. first evidence of immune system dysfunction
2. without treatment, this phase lasts about 1-3 years 3. Often you might see: persistent generalized lymphadenopathy, localized fungal infections (e.g. on the fingernails, toes, mouth), recalcitrant vaginal yeast and trichomonal infections in women, and oral hairy leukoplakia on the tongue. - skin manifestations that include seborrheic dermatitis, psoriasis exacerbations, molluscum, and warts - constitutional symptoms (night sweats, weight loss, and diarrhea) |
|
|
Clinical features of AIDS - pulmonary
|

- marked immune suppression leads to disseminated opportunistic infections and malignancies
- CD4 count is < 200 mm3 1. Community acquired bacterial pneumonia - recurrent bacterial pneumonia (two or more episodes per year) is 20 times more common 2. PCP - 70% of patients acquire PCP at some point, often the initial opportunistic infection, establishes the AIDS diagnosis. Leading cause of death in patients with AIDS. Occurs when the CD4 count is </= to 200mm3 3. tuberculosis- negative PPD test results are common because of immunosuppression 4. other infections- CMV or MAC - increased risk when CD4 count is < 50. Cryptococcus neoformans, histoplasma capsalatum, neoplasms (Kaposi's sarcoma) |
|
|
AIDS dementia
|
- progressive process in 33% of patients
- early stages : subtle impairment of recent memory and other cognitive deficits - later stages: changes in mental status, aphasia, motor abnormalities |
|
|
AIDS- toxoplasmosis
|
- usually a reactivation of a latent infection with Toxoplasmosis gondii
- symptoms both of a mass lesion (discrete deficits, headache) and of encephalitis (fever, altered mental status) - CT scan or MRI shows characteristics findings: multiple (more than three)- contrast enhances mass lesions in the basal ganglia and subcortical white matter |
|
|
AIDS- cryptococcal meningitis
|
- Diagnosed by identifying organisms in CSF by cryptococcal antigen, culture, or staining with India Ink
- treat with amphoteracin B for 10-14 days. Follow this with 8-10 weeks of oral fluconazole. Lifelong maintenance therapy with oral fluconazole |
|
|
CNS infections in AIDS patients
|
1. toxoplasmosis
2. cryptococcal meningitis 3. bacterial meningitis 4. histoplasmosis 5. CMV 6. progressive multifocal leukoencephalopathy (PML) 7. HSV 8. neurosyphilis, TB |
|
|
Non-infectious CNS diseases in AIDS patients
|
CNS lymphoma, CVA, metabolic encephalopathies, AIDS dementia
|
|
|
Clinical features of AIDS- GI
|
1. Diarrhea- most common GI complaint, caused by a variety of pathogens (E. coli, Shigella, salmonella, campylobacter, CMV, giardia, cryptosporidium, isospora belli, mycobacterium avium intracellulare). Antibiotic therapy is also a common cause
2. oral lesions- oral thrust (candidiasis), HSV or CMV (ulcers), oral hairy leukoplakia (EBV infection), Kaposi's sarcoma 3. esophageal involvement- candidiasis is the most common cause of dysphagia- also CMV and HSV- seen with CD4 counts < 100 4. anorectal disease - N. gonorrheae, C. trachomatis, syphilis, HSV |
|
|
Dermatologic features of AIDS
|

1. Kaposi's sarcoma- more common in homosexual men than in other groups. Painless, raised brown-black or purple papules (common sites: face, chest, genitals and oral cavity). Widespread dissemination can occur
2. HSV infections, molluscum contagiousum, secondary syphilis, warts, shingles, and many other skin conditions/infections occur with higher frequency |
|
|
CMV infection in an AIDS patient
|

- common cause of serious opportunistic viral disease
- disseminated disease is common and usually involves the GI or pulmonary systems - most important manifestation is retinitis- unilateral visual loss that can become bilateral if untreated (seen in 5-10% of AIDS patients) - colitis and esophagitis are other findings - treat with ganciclovir or foscarnet |
|
|
Mycobacterim Avium Complex (MAC) in an AIDS patient
|

- most common opportunistic bacterial infection in AIDS patients
- features include wasting syndrome (weight loss, fever), lymphadenopathy and anemia - MAC causes disseminated disease in 50% of AIDS patients. MAC occurs in patients with advanced AIDS and CD4 < 50 cells - diarrhea and weight loss are common |
|
|
HIV-1 wasting syndrome
|
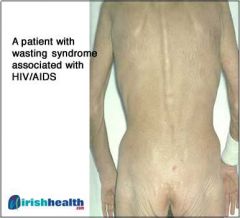
Profound involuntary loss of more than 10% of body weight in conjunction with either of the following
- chronic diarrhea (two or more stools per day for more than 1 month) - fever and persistent weakness for a similar period in absence of another cause |
|
|
Malignancies seen in AIDS patients
|
- Kaposi's sarcoma
- Non-hodgkin's lymphoma - rapidly growing mass lesion in CNS - primary CNS lymphoma |
|
|
Diagnosis of HIV
|
- PCR RNA viral load test - patients with acute HIV infection have very high levels of viremia. This test is repeated to assess effectiveness of therapy
- p24 antigen assay- less costly but less sensitive alternative to viral load test - seroconversion occurs 3-7 weeks after infection and confirms the diagnosis a. enzyme linked immunosorbent assay (ELISA) method- screening test for detecting antibody to HIV, becomes positive 1-12 weeks after infection. A negative ELISA essentially excludes HIV (99% sensitive) as long as the patient has not had subsequent exposure before the testing - if positive, western blot test should be done for confirmation (very specific) |
|
|
Diagnosis of AIDS
|
- depends primarily on the identification of an indicator condition or on finding in an HIV patient a CD4 count < 200
- there are many indicator conditions/AIDS defining illnesses |
|
|
Treatment of HIV/AIDs
|
1. Antiretroviral therapy- indicated in symptomatic patients regardless of their CD4 count and in asymptomatic patients with cd4 count < 500
2. Triple-drug regiments known as HAART- to target and prevent HIV replication at three different points along the replication process, use two nucleoside reverse transcriptase inhibitors and either a non-nucleoside reverse transcriptase inhbitor or a protease inhibitor - monitor response to treatment using plasma HIV RNA load-- the goal is to reduce the viral load to undetectable levels - it is generally recommended that HAART therapy be continued in pregnant patients with HIV - 100% adherence to the triple-drug regiment cannot be over-emphasized because even minor deviations can result in drug resistance. |
|
|
AIDS indicator diseases/AIDS defining illnesses (20)
|
1. candiasis, invasive
2. cervical cancer, invasive 3. coccidiomycosis, extrapulmonary 4. cryptococcus, extrapulmonary 5. cryptosporidiosis of > 1 month duration 6. CMV outside of lymphoreticular system 7. HIV related encephalopathy 8. HSV-1 infection of > 1 month duration 9. recurrent salmonella bacteremia 10. histoplasmosis, extrapulmonary 11. isosporiasis of > 1 month duration 12. Kaposi's sarcoma 13. lymphoma: primary CNS, immunoblastic or Burkitts 14. mycobacterial disease, disseminated or extrapulmonary 15. mycobacterium tuberculosis infection 16. PCP 17. pneumonia, recurrent (more than one episode in 1 yr) 18. PML 19. toxoplasmosis, cerebral 20. wasting syndrome due to HIV |
|
|
Opportunistic infection prophylaxis in AIDS patients - PCP
|
1. PCP (pneumocystic pneumonia, formely p. carinii, now p. jiroveci). Occurs in patients with AIDS when CD4 count is < 200 and patient is not on ppx. Dsypnea, dry cough and fever. Tests: CXR (bilateral, interstitial infiltrates), LDL levels (always elevated), ABG (hypoxia with inc A-a gradient), sputum stain for pneumocystis (specific but not sensitive), BAL (most accurate)
- TMP/SMX (bactrim is the preferred agent) |
|
|
TB prophylaxis in AIDS patients
|
- screen all patients with a yearly PPD test
- prescribe isoniazid plus pyridozine if the patient has a positive PPD - there may be false negatives on PPD due to immunocompromised state and T-cell dependent response to PPD |
|
|
Atypical mycobacteria - MAC prophylaxis in HIV patients
|
- start ppx when CD4 count is < 100
- clarithromycin and azithromycin as ppx |
|
|
Prophylaxis for toxoplasmosis in HIV patients
|
- give this to patients with CD4 count < 100
- TMP/SMX (Bactrim) is preferred agent |
|
|
Vaccination in HIV patients
|
- no live virus vaccinations!!!
- Pneumococcal vaccine (pneumovax) - q 5 to 6 years - infleunza vaccine q year - hep B vaccine (if not already Ab positive) |
|
|
Herpses Simplex Virus- general characteristics - two types
|
1. There are two types of HSV: HSV-1 and HSV-2. Both are very prevalent in the general population
2. HSV-1 is typically associated with lesions of the oropharynx 3. HSV-2 is associated with lesions of the genitalia 4. Both viruses, however, can cause either genital or oral lesions |
|
|
Pathophysiology of HSV
|
- after inoculation, the HSV replicates in the dermis and epidermis, then travels via sensory nerves up to the dorsal root ganglia. It resides as a latent infection in the DRG, where it can be reactivated at any time and reach the skin through the peripheral nerves
|
|
|
Transmission of HSV
|
- HSV is transmitted by contact with people who active ulcerations or shedding of the virus from mucous membranes. HSV-1 is typically associated with transmission through nonsexual contact (e.g. kissing) and HSV-2 through sexual contact
2. most people acquire HSV-1 in childhood, and more than 80% of adults have been infected with HSV-1 3. the incidence of HSV-2 has increased in recent years 4. Episodes of genital herpes frequently may be asymptomatic or may produce symptoms that often go unrecognized. Virus is still shed, and the infected person is still contagious. 5. contracting on form of herpes confers some degree of cross immunity- rendering primary infection with the other form of herpes less severe 6. Infection with genital herpes is associated with an increased risk of contracting HIV |
|
|
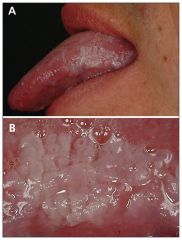
Clinical features of HSV-1
|

1. primary infection is usually asymptomatic and often goes unnoticed
2. when symptomatic, primary infection is associated with systemic manifestations (e.g. fever, malaise) as well as oral lesions 3. oral lesions involve groups of vesicles on patches of erythematous skin. Herpes labialis (cold sores) are most common on the lips (usually painful, heal in 2-6 weeks) 4. associated with bell's palsy |
|
|
Clinical features of HSV2
|

1. primary infection results in more severe and prolonged symptoms, lasting up to 3 weeks in duration
2. recurrent episodes are milder and of shorter duration, usually resolving within 10 days. There is also a decrease in the frequency of episodes over time 3. constitutional symptoms (e.g. fever, headache, malaise) often present with primary infection 4. HSV-2 presents with painful genital vesicles or pustules. Other findings are tender inguinal lymphadenopathy and vaginal and/or urethral discharge |
|
|
Disseminated HSV
|
- usually limited to ICH (immunocompromised host)
- may result in encephalitis, meningitis, keratitis, chorioretinitis, pneumonitis, and esophagitis - rarely, pregnant women may develop disseminated HSV, which can be fatal to both the mother and the fetus |
|
|
Neonatal HSV
|

- vertical transmission at the time of delivery is associated with congenital malformations, intrauterine growth retardation (IUGR), chorioamnionitis, and even neonatal death
|
|
|
Diagnosis of herpes
|
1. The diagnosis can be made clinically when the characteristic lesions are present
2. If there is uncertainty, perform the following tests to confirm the diagnosis: a. Tzanck smear- quickest test- perform by swabbing the base of the ulcer and staining with Wright's stain. This shows multinucleated giant cells. It does not differentiate between HSV and VZV b. Culture HSV is the gold standard of diagnosis- perform by swabbing the base of the ulcer. Results are available within 2-3 days c. cirect fluorescent assay with ELISA- 80% sensitive, results available within minutes to hours |
|
|
Treatment of herpes
|
1. There is no cure available for either type of herpes simplex. Antiviral treatment provides symptomatic relief and reduces the duration of symptoms
2. Mucocutaneous disease - treat with oral and/or topical acyclovir for 7-10 days. Valacyclovir and famciclovir have better bioavailability. oral acyclovir may be given as ppx for patients with frequent recurrences. Foscarnet may be given for resistant disease in ICHs - disseminated HSV warrants hospital admission. Treat with parenteral acyclovir |
|
|
Recurrences of HSV
|
- recurrences of HSV are associated with: stress, fever, infection and sun exposure
- recurrent episodes tend to become shorter in duration and less frequent over time |
|
|
Herpetic whitlow
|

- HSV infection of the finger caused by inoculation into open skin surface. Common in health care workers.
- painful vesicular lesions erupt at the fingertip - it may cause fever and axillary lymphadenopathy - treat with acyclovir. Do NOT mistake for paronychia (fungal or bacterial infection of skin around nails). Incision and drainage should NOT be done for herpetic whitlow |
|
|
Syphilis- general characteristics
1. cause 2. course |
1. It is caused by treponema pallidym spirochetes and transmitted by direct sexual contact with infectious lesions
2. It is a systemic illness with four stage (see next card). The late stages can be prevented by early treatment |
|
|
Clinical features of syphilis
1. primary stage 2. secondary stage 3. Latent stage 4. tertiary stage |
1. Primary stage- chancre - a painless, crater-like lesion that appears on the genitalia 3-4 weeks after exposure. Heals within 14 weeks even without therapy. Highly infectious- anyone who touches the lesion can transmit the infection
2. Secondary stage- this may develop 4-8 weeks after the chancre has healed. A maculopapular rash is the most common characteristic finding in this stage. Other possible sx: flu-like illness, aseptic meningits, hepatitis. Patients are contagious. About 1/3 of these patients develop latent syphilis 3. Latent stage- presence of positive of serologic test results in absence of clinical signs or symptoms. 2/3 of these patients remain asx, the other 1/3 develop tertiary syphilis. After 1 year patients are in late latent stage and are not contagious 4. tertiary syphilis- may occur up to 40 years after initial iinfxn. CV syphilis, neurosyphilis, and gummas (subcutaneous granulomas). Neurosyphilis is characterized by dementia, personality changes, tabes dorsalis |
|
|
Tabes dorsalis
|
- manifestation of tertiary syphilis/neurosyphilis--- posterior column degeneration
- loss of vibration, fine touch, and joint position sense - may have weakness, diminished reflexes paresthesia, loss of coordination and tabetic gait (high-stepping gait where the patient's feet slap the ground as they strike the floor - romberg sign- swaying of the body when the eyes are close - argyll robertson pupils- "prostitutes pupils" - pupils accomodate but don't react (get smaller with accomodation but do not react to light)- small constricted pupils bilaterally that do not constrict either directly or consentually with light. There is a mild constriction with accomodation, however. |
|
|
Argyll Robertson pupils
|

"prostitutes pupils" - pupils accomodate but don't react (get smaller with accomodation but do not react to light)- small constricted pupils bilaterally that do not constrict either directly or consentually with light. There is a mild constriction with accomodation, however.
- symptom of tertiary syphilis |
|
|
Diagnosis of syphilis
|
1. Dark-field microscopy- definitive diagnostic test- examines a sample of the chancre with visualization of spirochetes
2. Serologic tests- most commonly used tests a. nontreponemal tests- RPR, VDRL - high sensitivity, specificity is around 70%. If positive, confirmation is needed with specific treponemal test b. treponelam tests- FTA-ABS (fluorescent treponemal antibody), MHA-TP (microhemagglutination assay)- more specific than non-treponemal tests. NOT for screening for confirmation of a positive non-treponemal test 3. All patients should be tests for HIV infection |
|
|
Treatment of syphilis
|
1. Antibiotics are effective in early syphilis, but not so effective in late syphilis
2. Benzamine Penicillin G- one dose IM- is preferred agent. If the patient is allergic to penicillin, give oral antibiotics (doxycycline, tetracycline) for 2 weeks 3. If the patient has latent or tertiary syphilis- then give 3 IM doses once per week for 3 weeks 4. repeat nontreponemal tests every 3 months to ensure adequate response to treatment. Titers should decrease fourfold in 6 months. If they do not, that might treatment failure or re-infection. |
|
|
Chancroid
- cause - transmission - incubation period - clinical features - diagnosis - treatment - course |

- caused by hemophilus ducreyi, a gram negative rod
- transmission is through sexual contact - incubation period of 2-10 days - There are no systemic findings. Disseminated infections do not occur - clinical features- painful genital ulcer(s) that can be deep with ragged borders and with a purulent base, unilateral tender inguinal lymphadenopathy ("buboes") that appear 1-2 weeks after ulcer - diagnosis is made clinically. - r/o syphilis and HSV. May also want to test for HIV. No serologic tests are available and culture is not feasible because it requires a special media - treatment - oral azithromycin (one dose), ceftrixone (IM one dose) or al oral course of azithromycin, erythromycin, or ciprofloxacin - with treatment, most ulcers resolve within 1-2 weeks |
|
|
lymphogranuloma venereum
|
- a sexually transmitted disease caused by C. trachomatis
- clinical features- painless ulcer at the site of inoculation that may go unnoticed. A few weeks later, tender inguinal lymphadenopathy (usually unilateral) and constitutional symptoms develop - if untreated, proctocolitis may develop with perianal fissures and rectal stricture; obstruction of lymphatics may lead to elephantiasis of genitals - diagnosis is made by serologic tests (complement fixation, immunofluorescence). - the treatment is doxycycline (oral for 21 days) |
|
|
Pediculosis Pubis (Pubic Lice)
|

- pubic lice or "crabs" is a common STD caused by Phthirus pubis (the pubic or crab louse)
- It can be transmitted through sexual contact, clothing or towels - Severe pruritus in the genital region is characteristic. Other hairy areas of the body can be involved. - diagnosis is made by examination of hair under microscope (or possibly by the naked eye) - identification of adult lice or nits - Treatment with permethrin 1% shampoo (elimite)- apply to all hairy regions from the deck down and wash off after several hours. Sexual partner(s) should also be treated. Combs, clothing and bed linens should be washed thoroughly. |
|
|
Cellulitus - general characteristics
1. definition 2. causes 3. pathophysiology- route of infection 4. course/complications |
1. inflammatory condition of the skin and subcutaneous tissue.
2. it is caused by a wide variety of bacteria, the most common being group A streptococci or S. aureus 3. likely bacterial pathogens are based on patient histories. Bacteria gain entry through breaks in the skin: IV catheters, incisions, immersion in water and bites or wounds. Venous stasis diseases, lymphedema, and diabetic ulcers also are associated with cellulitis 4. If untreated, cellulitis may lead to potentially life-threatening bacteremia. Patients with cellulitis are predisposed to recurrences in the same area because of damage that occurs to the lymphatic vessels. |
|
|
Clinical features of cellulitis
|
1. classic findings of inflammation: erythema, warmth, pain and swelling
2. fever (may or may not be present) |
|
|
Diagnosis of cellulitis
|

1. the diagnosis is essentially clinical
2. obtain blood cultures if the patient has a fever 3. obtain tissue cultures if there is a wound, ulcer or site of infection 4. obtain imaging (plain film, MRI) if there is suspicion of deeper infection - spread of cellulitis to the face is a worrisome complication and any evidence of orbital involvement requires immediate evaluation by an ophthalmologist |
|
|
Treatment of cellulitis
|
1. Base treatment on suspected pathogens from the patient's history. Most patients require parenteral antibiotic therapy
2. Treat with staphylococcal penicillin (e.g. oxacillin, nafcillin) or a cephalosporin (e.g. cefazolin) 3. Continue IV antibiotics until signs of infection improve. Follow up with oral antibiotics for 2 weeks |
|
|
Common pathogens in cellulitis- likely pathogen by means of bacterial invasion
1. local trauma, breaks in skin 2. wounds, abscesses 3. Immersion in water 4. acute sinusitis |
1. group A streptococcus (s. pyogenes)
2. staph aureus 3. pseudomonas aeruginosa, aeromonas hydrophila, vibrio vulnificus 4. h. influenzae |
|
|
Erysipelas
- definition - cause - presentation - predisposing factors - complications - treatment - course |

- erysipelas- cellulitis that is usually confined to the dermis and lymphatics
- it is usually caused by group A streptococci (other forms of streptococci less commonly) - the classic presentation is well-demarcated, fiery red, painful lesion, most commonly on the lower extremities and the face. High fever and chills may be present. - predisposing factors include lymphatic obstruction (e.g. after radical mastectomy), local trauma or abscess, fungal infections, diabetes mellitus, and alcoholism - complications include sepsis, local spread to subQ tissues and necrotizing faciitis - treatment for uncomplicated cases is IM or oral penicillin or erythromycin- otherwise treat as for cellulitis - unfortunately, erysipelas has a high rate of recurrence |
|
|
Necrotizing faciitis
- definition - common bacterial causes - risk factors - clinical features - course |

- life threatening infection of deep soft tissues that rapidly tracks along fascial planes
- common bacterial causes include s. pyogenes and clostridium perfrigens - risk factors include recent surgery, diabetes, trauma and IV drug use - clinical features may include fever and pain out of proportion to appearance of skin in early stages, so a high index of suspicion is important. Extension of infection leads to thrombosis of microcirculation, resulting in tissue necrosis, discoloration, crepitus and cutaneous anesthesia - It may rapidly progress to sepsis, toxic shock syndrome (TSS) and multiorgan failure |
|
|
Differentiating DVT from Cellulitis
|
- like cellulitis, acute DVT presents with erythema, warmth, and tenderness in the affected extremity
- inflammation in DVT is usually restriction to the posterior calf - because homan's sign and the palpation of venous cords are not sensitive in detecting DVT, venous Doppler must sometimes be performed to differentiate between cellulitis and acute DVT |
|
|
Treatment of necrotizing faciitis
|
- antibacterial treatment alone is NOT sufficient. Rapid surgical exploration and excision of devitalized tissue is an absolute necessity
- broad spectrum parenteral antimicrobial therapy is warranted |
|
|
Lymphadenitis
|

- this is inflmmation of a lymph node (single or multiple) usually caused by local skin or soft tissue bacterial infection often hemolytic streptococci and staphylococci)
- it presents with fever, tender lymphadenopthy of regional lymph nodes and red streaking of skin from the wound or area of cellulitis - complications include thrombosis of adjacent veins, sepsis, and even death if untreated - helpful diagnostic studies include blood and wound cultures - it usually responds well to treatment. Treat with appropriate antibiotics (penicillin G, anti-staphyloccal penicillin, or cephalosporin) and warm compresses. Wound drainage may ultimately be necessary |
|
|
Tetanus- general characteristics
1. causes 2. risk factors |
1. It is caused by neurotoxins produced by spores of clostridium tetani (a gram-positive anaerobic bacillus)
- c. tetani proliferates and produces its exotoxin in contaminated wounds. The exotoxin blocks inhibitor transmitters at the neuromuscular junction 2. Patients at risk are those who have incomplete or no tetanus immunization |
|
|
Clinical features of tetanus infection
|
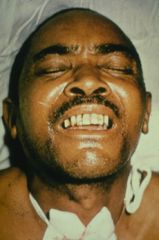
- the classic and earliest symptom is hypertonicity and contractions of the masseter muscles, resulting in trismus, or "lockjaw"
- progresses to severe, generalize muscle contractions, including: risus sardonicus- grin due to contraction of facial muscles, and opisthotonus- arched back due to contraction of back muscles - sympathetic hyperreactivity |
|
|
Diagnosis of tetanus infection
|

1. the diagnosis is clinical
2. obtain wound cultures, but they are not a reliable means of diagnosis - pic - opithotonus |
|
|
Treatment of tetanus infection
|
1. admit the patient to the ICU and provide respiratory support if needed.
2. give diazepam for tetany 3. Neutralize unbound toxin with passive immunization- give a single IM dose of tetanus immune globulin (TIG) 4. Provide active immunization with tetanus/diprtheria toxoid (Td) 5. Thoroughly clean and debride any wounds with tissue necrosis 5. Give antibiotics (metronidazole or penicillin G), although the efficacy is somewhat controversial |
|
|
Osteomyelitis - general characteristics
|
1. refers to inflammatory destruction of the bone due to infection
2. There are two main categories: a) hematogenous osteomyelitis (most common in children) - occurs secondary to sepsis, b) direct spread of bacteria from any of the following-- an adjacent infection (e.g. infected diabetic foot ulcer, decubitus ulcer), trauma (e.g. open fractures), vascular insufficiency 3. The most common organisms are S. aureus and coag-negative staph 4. osteomyelitis can involve any bone. Common locations include long bones (tibia, humerus, femur), foot and ankle and vertebral bodies |
|
|
risk factors for osteomyelitis
|
1. open fractures
2. diabetes mellitus (causes predisposition to infection and peripheral vascular disease) 3. use of illicit IV drugs 4. sepsis |
|
|
Clinical features of osteomyelitis
|
1. pain over the involved area of bone is the most common finding
2. localized erythema, warmth, or swelling may be present 3. systemic symptoms (e.g. fever, headache, fatigue) may be present, but are inconsistent findings 4. a draining sinus tract through the skin may form in chronic disease |
|
|
Diagnosis of osteomyelitis
|
1. WBC count- may or may not be elevated and is not useful in the diagnosis
2. ESR and CRP- these are fairly non-specific, but if these markers of inflammation are elevated in the appropriate clinical setting, seriously consider the diagnosis of osteomyelitis. Normal values do not r/o the disease. There are useful in the monitoring of response to therapy 3. Needle aspiration of infected bone or bone biopsy. Culture results can determine the specific antibiotic therapy 4. Plain xrays- the earliest radiographic changes (periosteal thickening or elevation) are not evident for at least 10 days. Lytic lesions are only seen in advanced diseased 5. radionucleotide bone scans- usually positive within 2-3 days of infection, but are relatively non-specific ( can be positive in metastatic bone disease, trauma or overlying soft tissue inflammation) 6. MRI is generally the most effective imaging study for diagnosis osteomyelitis and assessing the extent of disease process |
|
|
Risk factors of acute infectious arthritis
|
- prior joint damage (e.g. rheumatoid arthritis)
- joint prosthesis - diabetes mellitus |
|
|
Treatment of osteomyelitis
|
- Give IV antibiotics for extended periods (4-6 weeks). Initiate antibiotic therapy only after the microbial etiology is narrowed based on data from cultures.
- General guidelines: a) empiric therapy requires pencillase-resistant penicillin (e.g. oxacillin) or a first generation cephalosporin (e.g. cefazolin), b) add an aminoglycoside and possibly a beta-lactam antibiotic if there is a possibility of infection with a gram-negative organism, c) surgical debridement of infected necrotic bone is an important aspect of treatment |
|
|
Acute infectious arthritis - general characteristics- definition
|
1. acute infectious arthritis occurs when microorganisms (usually bacteria) invade the joint space (not the bone itself), where they release endotoxins and trigger cytokine release and neutrophil infiltration. These inflammatory reactions ultimately lead to erosion and destruction of the joint
|
|
|
Pathogenesis of acute infectious arthritis
|
- microorganism penetrate the joint via the following mechanisms:
1) hematogenous spread- most common route 2) contiguous spread from another locus of infection (e.g. osteomyelitis, abscess or cellulitis) 3) traumatic injury to the joint 4) iatrogenic (from arthrocentesis, arthroscopy) |
|
|
Organisms often implicated in acute infectious arthritis
|
- usually it is due to bacterial infection
- acute bacterial arthritis can be caused by any of the following: 1) s. aureus is the most common agent overall in adults and children. Various streptococcal species are also frequently involved. 2) an important gram-negative agent is N. gonorrhea. Gonococcal arthritis is the most common cause of acute infectious arthritis in your, sexually active adults 3) consider gram-negative organisms such as psedomonas aeruginosa or salmonella spp if there is a history of sickle cell, immunodeficiency or IV drug abuse |
|
|
Clinical features of acute infectious arthritis
|
1. The joint is swollen, warm, and painful
- the range of motion (active or passive is very limited) - an effusion can be palpated 2. Constitutional symptoms such fever, chills, and malaise are common |
|
|
Septic arthritis
1. joints most commonly involved 2. who has the worst prognosis |

1. the most common joint affected is the knee. The hip, wrist, shoulder and ankle may also be involved
2. patients with immunosuppression or connective tissue disease may have polyarticular arthritis - and a worse prognosis |
|
|
Gonococcal arthritis
1. presentation 2. joints commonly involved 3-4. other clinical features 5. treatment |
1. acute monoarthritis or oligoarthritis and often progresses within days in a migratory or additive pattern
2. knees, wrists, hands and ankles are the most commonly involved 3. tenosynovitis is often present in the hands and feet 4. fever, chills, and rash (macules, papules and/or pustules) are signs of disseminated gonococcal infection, If the patient has disseminated gonococcal infection, admit to the hospital 5. After the joint is initially aspirated, repeated aspiration is unecessary (unlike in other causes of septic arthritis) and antibiotics alone usually leads to improvement. Treat presumptively for chlamydial infection (e.g. doxycycline or azithromycin) - consider testings for HIV and syphilis. Educate the patient about safe sex |
|
|
Diagnosis of gonococcal arthritis
|
1. Perform a joint aspiration ("tap") and analyze the synovial fluid of all patients: WBC with diff (usually > 50,000 with >80% PMNs -most helpful, gram stain - 75% are gram positive, culture - aerobic and anaerobic, crystal analysis - keep in mind that acute gout may present like septic arthritis, PCR of synovial fluid- if gonococcal arthritis is suspected but gram stain and cultures are negative
2. Blood cultures are positive in > 50% of cases 3. other labs- leukocytosis in 1/2, elevated ESR and CRP 4. Imaging - plain films- generally not useful unless joint damage is severe. CT or MRI - helpful if the SI or facet joints are involved 5. obtain cultures from appropriate mucosal surfaces (GU) if gonococcal arthritis is suspected |
|
|
Treatment of acute infectious arthritis
|
1. Prompt antibiotic treatment - do NOT delay in initiating antimicrobial therapy when acute infectious arthritis is suspected
2. If the gram stain is negative but acute bacterial arthritis is still suspected, treat empirically until culture and sensitivities are available 3. drainage- daily aspiration of the affected joint as long as effusion persists is one treatment option. However, surgical drainage is recommended to prevent further damage to the articular cartilage that occurs with persistent infectious processes. Certain joints are amendable to arthroscopic drainage (shoulder, knee) whereas others are not (hip, wrist, elbow, ankle) and should be opened |
|
|
Complications of septic arthritis
|
- destruction of the joint and surrounding structures (e.g. ligaments, tendons) leading to stiffness, pain and loss of function
- avascular necrosis (if hip is involved) - sepsis |
|
|
Lyme Disease - general characteristics
1. endemic areas in the US 2. Incubation period 3. Transmission cycle |
1. three major endemic areas in the US: NE seaboard (Maine to Maryland), Midwest (north central states - Minnesota, Wisconsin) and West Coast (North California)
2. Incubation period - 3 to 32 days 3. Transmission cycle- caused by spirochete Borrelia burgdoferi. Transmitted by ticks, commonly the deer tick (ixodidae scapularis). The tick is hosted by white-footed mice (immature ticks), white-tailed deer (mature ticks) and briefly humans |
|
|
Clinical features of lyme disease - Stage 1 and 2
|

1. stage 1 - early, localized infection. a) erythema migrans is the hallmark skin lesion at site of the tick bite. Characteristically it is a large, painless, well-demarcated target-shaped lesion, commonly seen on the thigh, groin or axilla
2. Stage 2 - early, disseminated infection. Infection spreads via lymphatics and bloodstream within days to weeks after the onset of erythema migrans. Clinical features: intermittent flu-like symptoms, headaches, neck stiffness, fever/chills, fatigue, malaise, musculoskeletal pain. After several weeks, about 15% of patients develop one or several of the following (usually resolve within several months): Meningitis, encephalitis, cranial neuritis (often bilateral facial nerve palsy), peripheral radiculoneuropathy. Within weeks to months of onset of symptoms, about 8% will have cardiac manifestations (e.g. AV block, pericarditis, carditis). There usually only last for several weeks, but recurrence is common. |
|
|
Lyme Disease- clinical features - Stage 3
|

Late, persistent infection (months to years after initial infection)
a. arthritis - this occurs in 60% of untreated patients. It typically affects the large joints (especially the knees). Chronic arthritis will develop in some patients) b. Chronic CNS disease- subacute, mild encephalitis, transverse myelitis, or axonal polyneuropathy c. Acrodermatitis chronica atrophicans (a rare skin lesion) - reddish-purple plaques and nodules on the extensor surfaces of the legs |
|
|
Diagnosis of Lyme Disease
|
1. clinical diagnosis - In early, localized disease, document erythema migrans in a patient with history of tick exposure in an endemic area obviates the need for laboratory confirmation. Treat empirically.
2. Serologic tests- most important tests to confirm a clinical suspicion. ELISA is used to detect serum IgM and IgG antibodies during the first month. Western blot is used to confirm positive or equivocal results. |
|
|
Treatment of Lyme Disease
1. early localized disease 2. treatment of complications (e.g. facial nerve palsy, arthritis or cardiac disease) |
1. If it is confined to the skin- 10 days of antibiotic therapy is adequate. If there is any evidence of spread beyond the skin, then extend treatment to 20-30 days. For early disease- oral doxycycline for 21 days (contraindicated in pregnant woman and children </= 12 yo. Amoxicillin and cefuroxime are alternative agents. Erythromycin may be given to pregnant patients with penicillin allergies.
2. facial nerve palsy, arthritis or cardiac disease --> prolonged antibiotic therapy (30 - 60 days). for meningitis or other CNS complications- treat with IV antibiotics for 4 weeks |
|
|
Rocky Mountain Spotted Fever - general characteristics
1. cause 2. transmission 3. endemic areas |
1. caused by the intracellular bacteria Rickettsia rickettsii
2. Ticks feeding on various mammal serve as vectors for disease transmission 3. The major endemic areas include the southeastern, midwestern and western United States. Peak incidence is in the spring and summer months due to increased outdoor activityP |
|
|
Pathophysiology of Rocky Mountain Spotted Fever
|
- organisms enter the host cells via tick bites, multiply in the vascular endothelium and spread to different layers of the vasculature
- damage to the vascular endothelium results in increased vascular permeability, activation of complement, microhemorrhages and microinfarcts |
|
|
Clinical features of Rocky Mountain Spotted Fever
|
1. The onset of symptoms is typically 1 week after the tick bite
2. Classically it presents with a sudden onset of fever, chills, malaise, nausea, vomiting, myalgias, photophobia, and headache 3. Papular rash appears after 4 to 5 days of fever. Rash starts peripherally (wrists, forearmsn ankles and soles) but then spreads centrally (to the rest of the limbs, trunk and face). It becomes maculopapular and eventually petechial. 4. It may lead to interstitial pneumonitis |
|
|
Diagnosis of Rocky Mountain Spotted Fever
|
1. Diagnosis is primarily clinical. Laboratory abnormalities may include elevated LFTs and thrombocytopenia.
2. Acute and convalscent serology and immunofluorescent staining of skin biopsy are confirmatory tests |
|
|
Treatment of Rocky Mountain Spotted Fever
|
1. doxycycline - usually given for 7 days, given IV if the patient is vomiting
2. CNS manifestations or pregnant patients- give chloramphenicol |
|
|
Malaria - general characteristics
|
1. A protozoal infection caused by one of four organisms: a) plasmodium falciparum, b) plasmodium ovale, c) plasmodium vivax, d) plasmodium malariae.
2. Prevalent in tropical climates, parts of Africa and the Middle East 3. Transmitted via mosquito bite in endemic areas |
|
|
Clinical features of Malaria
|
- symptoms may include fever and chills, myalgias, headache, nausea, vomiting, and diarrhea
- Fever pattern varies depending on cause a. p. falciparum- fever is usually constant b. p. ovale and p. vivax - fever usually spikes every 48 hours c. p. malariae- fever usually spikes every 72 hours |
|
|
Diagnosis of Malaria
|
1. Identify organism on peripheral blood smear
2. Blood smear must have Giemsa stain |
|
|
Treatment of Malaria
|
1. Use chloroquine phosphate unless resistance is suspected. In many countries, chloroquine resistance is so prevalent that it should be assumed
2. If chloroquine resistance is suspected, give quinine sulfate and tetracycline. Alternative agents are atovaquone-proguanil and mefloquine. 3. P. falciparum infection may require quinidine and doxycycline 4. Relapses can occur in P. vivax and P. ovale hypnozoites in the liver. Add a 2-week regimen of primaquine phosphate for these types of malarial infection 5. ppx is important for travelers to endemic regions. Mefloquine is the agent of choice in chloroquine-resistant areas. Chloroquine can be used in areas where chloroquine resistance has not been reported |
|
|
Malaria prophylaxis
|
ppx is important for travelers to endemic regions. Mefloquine is the agent of choice in chloroquine-resistant areas. Chloroquine can be used in areas where chloroquine resistance has not been reported
|
|
|
Rabies- general characteristics
|
1. A devastating, deadly viral encephalitis
2. contracted from a bite or scratch by an infected animal. Infection from a corneal transplant has also been documented 3. more prevalent in developing countries where rabies vaccination of animals is not widespread |
|
|
clinical features of rabies infection
|
1. the incubation period typically ranges from 30-90 days but varies considerably
2. once symptoms are present, rabies is almost invariably fatal 3. Symptoms in progressive order: pain at site of bite, prodromal symptoms of sore throat, fatigue, headache, nausea and or vomiting, encephalitis (confusion, combativeness, hyperactivity, fever and seizures may be present), hydrophobia- inability to drink, laryngeal spasm with drinking, hyper-salivation ("foaming at the mouth"), usually progresses to coma and death - some patients may present with ascending paralysis |
|
|
Diagnosis of rabies
|
1. virus or viral antigen can be identified in infected tissue. Virus can be isolated in saliva as well
2. fourfould increase in serum antibody titers 3. identification of negri bodies histologically 4. PCR detection of virus RNA |
|
|
Treatment (postexposure management)
|
1. clean the wound thoroughly with soap
2. For wild animal bites (e.g. bat or raccoon), the animal should be captured if possible, killed and sent to a laboratory for immunofluorenscence of brain tissue. 3. If a patient was bitten by a health dog or can in an endemic area, the animal should be captured and observed for 10 days. If there is no change in the animal's condition, then it likely does NOT have rabies 4. For known rabies exposure, both of the following should be performed. 1) passive immunization - administer the human rabies immunoglobulin to patients, info the wound as well as in the gluteal region. 2) active immunization- administer the antirabies vaccine in three IM does into the deltoid or thigh over a 28-day period |
|
|
Pre-exposure rabies prophylaxis
|
Rabies vaccine is available for at-risk individuals (e.g. those with potential exposure, such as veterinarians, wildlife officials, and laboratory workers)
|
|
|
Candidiasis - general characteristics
|

1. candida species are oval, budding yeasts known for their formation of hyphae and long pseudohyphae. They normally colonize humans, and it is the overgrowht of these organism that results in the clinical pathology of candidiasis.
2. candida albicans is the most common cause of candidiasis |
|
|
risk factors for candidiasis
|
1. antibiotic therapy
2. diabetes mellitus 3. immunosuppressive therapy 4. immunocompromised hosts (increased risk for both mucocutaneous and system candidiasis) |
|
|
Clinical features of candidiasis
|

1. Typical presentation is the mucocutaneous growth. The most common affected areas are:
a. vagina - "yeast infection" - this results in a thick, white, "cottage cheese-like" vaginal discharge. The discharge characteristically is painless but does cause pruritus. b. mouth, oropharynx- "thrush" - this causes thick, white plaques that adhere to the oral mucosa. Usually they are painless. Unexplained oral thrush should raise suspicion of HIV infection c. cutaneous candidiasis- this causes erythematous, eroded patches with satellite lesions-- it is more common in obese diabetic patients and appears in skin folds, underneath breasts and in macerated skin areas d. GI tract- e.g. esophagus - candida esophagitis may cause significant odynophagia. It may also be asymptomatic. 2. Disseminated or invasive disease may occur in immunocomprimised hosts. Manifestations include sepsis/septic shock, meningitis and multiple abscesses in various organs |
|
|
Diagnosis of candidiasis
|
1. Mucocutaneous candidiasis diagnosis is primarily clinical; KOH preparation demonstrates yeast
2. Invasive candidiasis is diagnosed by blood or tissue culture |
|
|
Treatment of candiasis
|
1. remove indwelling catheters or central lines
2. acceptable treatments for oropharyngeal candiasis : clotrimazole troches (dissovle in the mouth) five times per day, nystatin mouthwash ("swish and swallow") three to five times per day; only for oral candiasis, oral ketoconazole for esophhagitis 3. vaginal candidiasis- miconazole or clotrimazole cream 4. cutaneous candiasis- oral nystatin powder, keeping skin dry 5. for systemic candidiasis, use amphoteracin B or fluconazole. New alternative antifungal agents include voriconazole and caspofungin |
|
|
Aspergillus- general characteristics
|

1. Aspergillus spp. spores are found everywhere in the environment. Typically, disease occurs when spores are inhaled into the lung.
2. Invasive aspergillosis is usually limited to severely immunocompromised patients. It should be considered in an immunocompromised patient with fever and respiratory distress despite use of broad-spectrum antibiotics 3. Three main types of clinical syndromes associated with aspergillus ( Allergic bronchopulmonary aspergillosis, pulmonary aspergilloma, invasive aspergillosis) |
|
|
Aspergillus - clinical features - allergic bronchopulmonary aspergillosis
|
- type I hypersensitivity reaction to Aspergillus (allergy- IgE mediated- fast response, mast cells degranulate and release histamine)
- It presents with asthma and eosinophilia. Recurrent exacerbations are common |
|
|
Aspergillus- clinical features - pulmonary aspergilloma
|

- pulmonary aspergilloma (fungus ball) is caused by inhalation of spores into the lung. Patients with a history of sarcoidosis, histoplasmosis, tuberculosis and bronchiectasis are at risk
- it presents with chronic cough, hemoptysis may be present as well - it may resolve spontaneously or invade locally |
|
|
Aspergillus- clinical features - invasive aspergillosis
|
- this occurs when hyphae invade the lung vasculature, resulting in thrombosis and infarction
- hosts are typically at-risk patients with acute leukemia, transplant recipients, and patients with advanced AIDS - It usually present with acute onset of fever, cough, respiratory distress and diffuse, bilateral pulmonary infiltrates - It is transmitted via hematogenous dissemintation and may invade the sinuses, orbits and brain |
|
|
Diagnosis of aspergillus
|
1. CXR reveals a dense pulmonary consolidation and sometimes a fungus ball.
2. definitive diagnosis of invasive aspergillosis is by tissue biopsy, but diagnosis is presumed when aspergillus is isolated from the sputum of a severely immunocompromised/neutropenic patient with clinical symptoms 3. blood cultures are usually NOT helpful because they are rarely positive |
|
|
Treatment of aspergillus infections
1. allergic bronchopulmonary aspergillosis 2. pulmonary aspergilloma 3. invasive aspergillosis 4. if brain involvement is suspected |
1. avoid exposure, corticosteroids may be helpful
2. if massive hemoptysis, patients may require lung lobectomy 3. IV amphoteracin B, voriconazole or caspofungin 4. emergent imaging, surgery may be needed |
|
|
Cryptococcosis - general characteristics
|
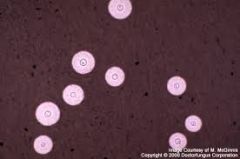
1. caused by cryptococcus neoformans, a budding, round yeast with a thick polysaccharide capsule
2. associated with pigeon droppings 3. most commonly seen in patients with advanced AIDS 4. infection is due to inhalation of fungus into lungs. Hematogenous spread may involve the brain and meninges |
|
|
Clinical features of cryptococcal infection
|
1. CNS disease - meningitis or meningoencephalitis. brain abscess is also possible. CNS disease is a life-threatening condition that requires aggressive treatment. It should always be on the differential diagnosis of an HIV-positive patient with fever and a headache. If untreated, it is almost invariably fatal
- symptoms include fever, headache, irritability, dizziness, confusion, and possibly seizures. Onset may be insidious. 2. isolate pulmonary infection may occur |
|
|
Diagnosis of cryptococcus
|
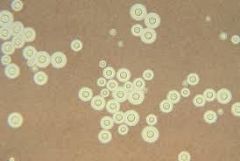
1. LP is absolutely essential if meningitis is suspected. Latex agglutination detects cryptococcal antigen in the CSF. India ink smear shows encapsulated yeasts.
2. tissue biopsy is characterized by lack of inflammatory response 3. The organism may also be present in urine and blood |
|
|
Treatment of cryptococcal infection
|
1. Use amphoteracin B with flucytosine for approximately 2 weeks, followed by oral fluconazole
2. the duration of therapy varies depending on follow-up CSF cultures |
|
|
Blastomycosis
|

- caused by blastomyces dermatitidis- dimorphic fungus
- transmission is via inhalation of spores from the environment - clinical features- disseminated infection-- chronic, indolent disease, constitutional symptoms, lymphadenopathy, pneumonia - dx- culture from urine, sputum, body fluids - tx: PO intraconazole x 6-12 months, Amphoteracin B for meningitis |
|
|
Histoplasmosis
|
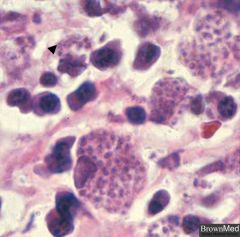
- caused by histoplasma capsulatum (dimorphic fungue with septate hyphae)
- transmitted via exposure to bird/bat droppings (endemic in Ohio and Mississippi river valleys) - clinical features: flu-like symptoms, erythema nodosum, hepatosplenomegaly - dx: demonstration of yeast in body fluids or skin - tx: PO itraconazole, amphoteracin B for severe infection or those who are immuocompromised - common in caves-- seen in spelunkers - Histo Hides in macrophages |
|
|
Coccidiomycosis
|
- caused by coccidiodes immitis (dimorphic fungus)
- transmitted via inhalation of spores - asymptomatic or non-specific respiratory symptoms, dissemination (focal CNS findings) - dx: visualization of fungus in fluids or skin - tx: PO fluconazole or itraconazole x 6 months, IV amphoteracin B for severe infection of immunocompromised patient |
|
|
Sporothricosis
|
- caused by sporothrix schenckii (dimorphic, cigar-shaped yeast)
- transmitted via invasion of the skin by thorn or other plant material (always think of in gardeners) - clinical features: lymphocutanous form (hard, subQ nodules that ulcerate and drain, disseminates form (pneumonia, meningitis) - dx: visualization of yeast in tissue or body fluids or serology - tx: potassium iodide x 1-2 mo, itraconazole x 3-6 mo, if disseminated: amphoteracin B |
|
This infection looks likes crushed ping pong balls on histology
|
Pneumocystis (PCP)
|
|
|
Fever of unknown origin (FUO) - definition
|
1. classically defined as having met these criteria: a) fever > 38.3 C (100F), b)continuing on several occasion for at least 3 weeks, c) no diagnosis over this time period despite 1 week of inpatient work-up
2. Because of changes in medical practice, this definition has been altered to include three outpatient visits in lieu of 1 week in the hospital |
|
|
Causes of fever of unknown origin
|
1. Infection - most common cause (TB and other mycobacterial infections, occult abscesses (hepatic, retroperitoneal), UTI/complicated UTI, endocarditis, sinusitis, HIV, infectious mononucleosis and other viruses, malaria and other parasitic infections
2. occult neoplasms (second most common cause)- especially Lymphoma (particulary Hodgkin's lymphoma), leukemia 3. Collagen vascular disease (SLE, Still's dz, PAN, temporal arteritis, PMR) 4. other causes - granulomatous disease (sarcoidosis, crohn's), drug fevers (sulfonamides, penicillin, quinidine, barbiturates), PE, hemolytic anemia, familial mediterranean fever, gout, subacute thyroiditis, factitious illnesses) |
|
|
Clinical features of fever of unknown origin
|
1. manifestations that may accompany fever but are not specific to any entity: chills, rigors (sever chills with pronounced shivering and teeth chattering), night sweats, change in mental status (especially at extremes of age)
2. Look for systemic manifestations of some of the most common causes (skin changes, constitutional symptoms, anemia, weight loss) |
|
|
Diagnosis of fever of unknown origin
|
1. careful history and physical exam- with attention to meds, travel history, immune system competency, and review of systems
2. lab tests- CBC with diff, UA, cultures of blood, sputum, CSF, urine, and stool, analysis and culture of abnormal fluid collections (e.g. joint, pleural), complement assay, PPD if TB on differential, LFTS, ESR, ANA, RF, TSH 3. imaging studies : CXR, CT chest and abdomen (to detect tumors and abscesses), tagged WBC scan, MRI, ultrasound and echo 4. LN biopsy, bone marrow of tissue biopsy if high suspicion of tumor or abscess 5. observation is sometimes necessary |
|
|
Treatment of fever of unknown origin
|
1. antibiotics and corticosteroids may mask the patterns of fever response. Base empiric treatment with antibiotics on severity of illness
2. If the patient is not acutely ill, observation alone may be all that is necessary to arrive at a specific diagnosis 3. In some cases of FUO, fevers may resolve spontaneously with no diagnosis ever made 4. the sense of urgency in determining the cause of fevers should be in proportion to the severity of illness and host's immune status |
|
|
Toxic Shock Syndrome - general characteristics
|
- most commonly associated with menstruating women and tampon use, but can occur in patients of all ages, male and female
- other risk factors include surgical wounds, burns, and infected insect bites - it can be caused by an enterotoxin of S. aureus or less frequently an exotoxin of group A streptococcus. Note that it is the toxin rather than the bacteria that causes the pathology associated with TSS |
|
|
Clinical features of Toxic Shock Syndrome (TSS)
|

- the onset of symptoms is abrupt
- symptoms may include: flu-like symptoms, high fever, headache, myalgias, diffuse macular, erythematous rash, hyperemic mucus membranes ("strawberry tongue"), warm skin due to peripheral vasodilation, hypotension, n/v, diarrhea 3. By definition there must be at least three organ systems involved (GI, renal, hematologic- dec platelets, MSK- inc CK, CNS 4. multisystem organ dysfunction or failure may occur 5. during the convalescent phase of illness, the rash usually desquamates over the palms and soles |
|
|
Diagnosis of TSS
|

1. a high index of suspicion is important
2. blood cultures are often negative 3. cultures may be taken from the suspected source, but the diagnosis is primary clinical * pic = strawberry tongue- may be seen in TSS, scarlet fever and kawasaki disease |
|
|
Treatment of toxic shock syndrome
|
1. hemodynamic stabilization should be the first concern and may require aggressive fluids and even vasopressors
2. the source of toxin (e.g. tampon) should be removed immediately. Wounds may require drainage and debridement 3. give anti-staphylococcal therapy such as naficillin, oxacillin or vancomycin in a very ill patient. clindamycin is sometimes used as an adjunct. |
|
|
Catheter-Related Sepsis
- most common organisms implicated - risk factors - clinical features - treatment |
- Central venous catheters are a common cause of fever and sepsis in the hospital, especially in the ICU
- the most common organisms are s. aureus and s. epidermidis - risk factors are emergent placement, femoral lines, and prolonged indwelling of the line - only half of all patients with catheter-related sepsis have clinical evidence of infection AT the site of insertion (i.e. erythema, purulence). Therefore a high index pf suspicion is required. - If you suspect catheter-related sepsis, promptly remove the catheter and send the tip for culture. This alone typically leads to resolution of the fever and decreased leukocytosis. Antibiotics are usually initiated. Narrow the spectrum once the organism is identified. |
|
|
Neutropenic Fever- common causes
|
- common causes include bone marrow failures (e.g. due to toxins, drugs), bone marrow invasion (e.g. hematologic malignancy, metastatic cancer) and peripheral causes (e.g. hypersplenism, SLE, AIDS). Isolated neutropenia (agranulocytosis) is commonly caused by drug reactions
|
|
|
Neutropenic fever
- pathophysiology - most common infections |
- because neutropenia severely compromises the patient's ability to mount an inflammatory response, fever may be the only manifestation of a raging infection
- the most common infections seen in neutropenic individuals are septicemia, cellulitis and pneumonia |
|
|
Neutropenic fever
- what tests should be ordered? - Treatment? If no response? |
- obtain the following for any neutropenic patient with a fever: CXR, panculture (blood, urine, sputum, line tips, wounds), CBC, complete metabolic panel
- place the patient on reverse isolation (positive pressure room, masks and strict handwashing) - give broad-spectrum antibacterial agents immediately after cultures are drawn - if fever persists beyond 4-5 days despite broad-spec abs, give antifungal agents such as IV amphoteracin B. - consider G-CSF |
|
|
Infectious Mononucleosis - general characteristics
1. infectious agents implicated? 2. epidemiology? who is most commonly affected? |
1. caused by EBV (rarely by CMV which causes a similar clinical picture but it milder)
2. It is most commonly seen in adolescents and young adults, especially college students and military recruits (but may occur at any age). Infected children often experience milder symptoms or no symptoms. |
|
|
Infectious mononucleosis- general characteristics
1. differential diagnosis in patients with fever, lymphadenopathy and pharyngitis 2. transmission |

1. acute HIV infection, streptococcal infection, CMV or toxoplasma infection. In pregnant patients, iti important to perform diagnostic tests such as HIV, CMV and toxoplasma-- as these infections can have adverse affects on the fetus
2. the usual mode of transmission is through infected saliva (e.g. kissing, sharing food). Most adults (90%) have been infected with EBV and are carriers but infectious mononucleosis is uncommon in adults. One infection usually confers lifelong immunity. The incubation period is typically 2-5 weeks |
|
|
Clinical features of infectious mononucleosis
1. symptoms 2. signs |

1. fever- temperatures may be as high as 40C, fever usually resolves within 2 weeks. Sore throat, malaise, myalgias, weakness-may linger for several months
2. lymphadenopthy- this is found in > 90% of patients. Tonsillar or cervical (especially posterior cervical) lymph nodes may be quite enlarged, painful and tender. - pharyngeal edema and/or exudate - frequently present - splenomegaly - present in half of patients - maculopapular rash- present in approximately 15% of patients, but higher if ampicillin is given - hepatomegaly- in 10% of cases - palatal petechiae and eyelid (periorbital) edema- may occur in minority of cases |
|
|
Diagnosis of infectious mononucleosis
|
1. serology- monospot test- for detection of heterophile antibody. Heterophile antibodies are positive within 4 weeks of infection with EBV mononucleosis and are undetectable by 6 months. Thus a positive monospot test indicates acute infection with EBC mononucleosis. This will not be seen in CMV mono
- rapid heterophile tests are highly sensitive and specific, particularly in adolescents 2. EBV -specific antibody testing- perform in cases in which diagnosis is not straightforward (usually done by indirect immunofluorensence microscopy or ELISA) 3. peripheral blood smear- usually reveals lymphocytic leukocytosis with large, atypical lymphocytes 4. Throat culture- perform if pharyngitis is present to rule out a secondary infection with beta-hemolytic streptococci |
|
|
Complications of infectious mononucleosis
|
1. hepatitis
2. neuro complications (rare): meningoencephalitis, Guillain-Barre syndrome, Bell's palsy 3. splenic rupture- rare 4. thrombocytopenia, hemolytic anemia 5. upper airway obstruction due to lymphadenopathy - rare |
|
|
Treatment of infectious mononucleosis
|
1. Generally there is NO specific treatment as most people completely recover within 3-4 months. Supportive care - rest, fluids, avoidance of strenuous activities until splenomegaly resolves to prevent splenic rupture, analgesics to reduce temperature and pharyngeal pain- NSAIDS and acetaminophen
2. Give a short course of steroids if there is airway compromise. Steroids have also been effective in patients with thrombocytopenia or hemolytic anemia. Steroids are NOT recommended routinely 3. when to return to sports: concern is splenic rupture. Patients should wait 3-4 weeks from symptom onset before returning to sports as splenic rupture is very rare after 4 weeks |
|
|
Common organisms in pneumonia
1. typical 2. atypical 3. nosocomial 4. aspiration |
1. strep pneumoniae, H. influenzae, Moraxella catarrhalis
2. Atypical- mycoplasma spp, chlamydia spp, legionella spp 3. Nosocomial - staph aureus, gram neg rods 4. aspiration- oral anaerobes, gram neg rods, s. aureus |
|
|
common organisms in UTIs
|
E. coli, s. saphrophyticus, enterococcus, klebsiella, proteus, pseudomonas, enterobacter, yeast
|
|
|
common organisms in osteomyelitis and septic arthritis
|
s. aureus, s. epidermidis, streptococcys spp, gram negative rods.
- consider n. gonorrheae in septic arthritis in adolescents |
|
|
common organisms in skin and soft tissue infections
1. surgical wound 2. diabetic ulcer 3. intravenous catheter site 4. cellulitis 5. necrotizing faciitis |
1. s. aureus, gram neg rods
2. s. aureus, gram neg rods, anaerobes 3. s. aureus, s. epidermidis 4. s. aureus, group A streptococci 5. clostridium perfringens, group A streptococci |
|
|
Common organisms in upper respiratory infections
1. pharyngitis 2. acute bronchitis 3. acute sinusitis 4. chronic sinusitis |
1. viral, group A strep
2. viral 3. viral, s. pneumo, h. influenzae, m. catarrhalis 4. s. aureus, anaerobes |