Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
409 Cards in this Set
- Front
- Back
|
The brain stem and spinal cord have:
|
-Alar plate-gives rise to sensory neurons
-basal plate-gives rise to motor neurons |
|
|
Neural tube gives rise to
|
three primary vesicles, which develop into five secondary vesicles
|
|
|
AFP
|
-Alpha-fetoprotein
-found in the amniotic fluid and meternal serum. It is an indicator of neural tube defects (spina bifida, anencephaly). AFP levels are reduced in mothers of fetuses with Down Syndrome |
|
|
Middle meningeal artery
-branch of -enters cranium through -supplies -laceration results in |
-maxillary artery
-foramin spinosum -most of the dura -epidural hemorrhage (hematoma) |
|
|
Vertebral Artery
-branch of -gives rise to |
-subclavian artery
-anterior spinal artery and the posterior inferior cerebellar artery |
|
|
PICA
-supplies |
-The dorsolateral quadrant of the medulla. This quadrant includes the nucleus ambiguus (CN IX, X, and XI) and the inferior surface of the cerebellum
|
|
|
Pontine Ateries
-supply |
-The base of the pons, which includes the corticospinal fibers and the exiting root finbers of the abducent nerve (CN VI)
|
|
|
Labyrinthine Artery
-arises from |
-Basilar artery in 15% of people
-Ainterior Inferior Cerebellar Artery in 85% of people |
|
|
AICA
-supplies |
-The caudal lateral pontine tegmentum, including CN VII, the spinal trigeminal tract of CN V, and the inferior surface of the cerebellum
|
|
|
Anterior Spinal Artery
-supplies |
-Anterior 2/3 of the spinal cord
-in the medulla, the anterior spinal artery supplies the pyramid, medial lemniscus, and root fibers of CN XII |
|
|
Posterior Communicating Artery
-supplies -aneurysm |
-Hypothalamus and ventral thalamus
-An aneurysm of this artery is the second most common aneurysm of the circle of Willis. It commonly results in third-nerve palsy. |
|
|
Anterior Choroidal Artery
-arises from -supplies |
-Internal Carotid
-lateral geniculate body, globus pallidus, and posterior limb of the internal capsule |
|
|
Anterior Cerebral Artery
-supplies |
-The medial surface of the hemisphere from the frontal pole to the parieto-occipital sulcus
|
|
|
Anterior Communicating Artery
-connects -aneurysm |
-The two Anterior Cerebral Arteries.
-It is the most common site of aneurysm of the circle of Willis, which may cause bitemporal lower quadrantanopia |
|
|
Medial Striate Arteries
-are the -supply |
-The penetrating arteries of the anterior cerebral artery.
-They supply the anterior portion of the putamen and caudate nucleus and the anteroinferior part of the internal capsule |
|
|
Middle Cerebral Artery
-supplies |
-Broca's and Wernicke's speech areas
-The face and arm areas of the motor and sensory cortices -The frontal eye field |
|
|
Lateral striate arteries
-are the -they are -supply |
-The penetrating branches of the middle cerebral artery.
-They are the arteries of stroke -supply the internal capsule, caudate nucleus, putamen, and globus pallidus |
|
|
Cavernous sinus
-contains |
CN III, IV, V-1, V-2, VI, postganglionic sympathetic fibers, and the siphon of the internal carotid artery
|
|
|
Hydrocephalus
-is |
-dilation of the cerebral ventricles caused by blockage of the CSF pathways. It is characterized by excessive accumulation of CSF in the cerebral ventricles or subarachnoid space.
|
|
|
Noncommunicating Hydrocephalus
-results from |
-Obstruction within the ventricles (congenital aqueductal stenosis)
|
|
|
Communicating hydrocephalus
-results from |
-Blockage within the subarachnoid space (adhesions after meningitis)
|
|
|
Normal-pressure hydrocephalus
-occurs when |
-The CSF is not absorbed by the arachnoid villi. It may occur secondary to posttraumatic meningeal hemorrhage.
-Characterized by the triad of progressive dementia, ataxic gain, and urinary incontinence -Remember: wacky, wobbly, and wet |
|
|
Hydrocephalus ex vacuo
-results |
-From a loss of cells in the cuadate nucleus (Huntington's disease)
|
|
|
Pseudotumor cerebri
-is -results from -occurs in -is characterized by |
-a benign intracranial hypertension
-from increased resistance to CSF outflow at the arachnoid villi. -obese young women -papilledema without mass, elevated CSF pressure, and deteriorating vision. The ventricles may be slit-like |
|
|
The two lateral ventricles communicate with the third ventricle through the
|
interventricular foramina of Monro
|
|
|
The third ventricle
-located -communicates with |
-between the medial walls of the diencephalon.
-communicates with the fourth ventricle through the cerebral aqueduct |
|
|
The fourth ventricle
-communicates |
with the subarachnoid space through three outlet foramina
-2 lateral foramina of Luschka -1 medial foramen of Magendie |
|
|
Common causes of bacterial meningitis
-in newborns (<1 month) |
-Group B strep (Streptococcus agalactiae)
-E. coli -Listeria monocytogenes |
|
|
Common causes of bacterial meningitis
-older infants and young children (1-23 months) |
Strep pneumoniae
|
|
|
Common causes of bacterial meningitis
-young adults (2-18 years) |
Neisseria meningitidis
|
|
|
Common causes of bacterial meningitis
-older adults (19 years and older) |
Streptococcus pneumoniae
|
|
|
The Neural Crest
-Gives rise to |
-PNS (peripheral nerves and sensory and autonomic ganglia)
-Psuedounipolar ganglion cells of the spinal cand cranial nerve ganglia, Schwann cells, Multipolar ganglion cells of autonomic ganglia, Leptomeninges (pia-arachnoid-envelop the brain and spinal cord), Chromaffin cells (of suprarenal medulla-elaborate Epi), Pigment cells (melanocytes), Odontoblasts (elaborate predentin), Aorticopulmonary septum of the heart, Parafollicular cells (calcitonin-producing C-cells), Skeletal and Connective Tissue Components of the pharyngeal Arches |
|
|
Anterior Neuropore
-gives rise to -failure to close results in |
-The lamina terminalis
-Anencephaly (failure of the brain to develop) |
|
|
Posterior Neuropore
-failure to close results in |
Spina bifida
|
|
|
Microglia
-arise from the |
monocytes
|
|
|
Spina bifida occulta
-see |
-tuft of hairs
-failure of vertebral column to close -no bulging |
|
|
Meningocele
-see |
-failure of vertebral column to close
-failure of dura to close -subarachnoid space bulging -spinal cord in normal spot |
|
|
Meningomyelocele
-see |
-failure of vertebral column to close
-failure of dura to close -subarachnoid space and spinal cord bulging |
|
|
Conus Medullaris ends at
-in newborn -in adult |
-L3
-L1 |
|
|
Optic Nerve and Chiasma
-derived from -The optic nerve fibers occupy -failure of this fissure to close results in |
-the Diencephalon
-The optic nerve fibers occupy the choroid fissure -failure of this fissure to close results in coloboma iridis |
|
|
Adenohypophysis
-derived from -remnants |
-ectodermal diverticulum of the primitive mouth cavity, which is also called Rathke's pouch.
-Remnants of Rathke's pouch may give rise to a congenital cystic tumor, a craniopharyngioma |
|
|
Neurohypophysis
-develops from |
-A ventral evagination of the hypothalamsu (neuroectoderm of the neural tube)
|
|
|
Fetal alcohol syndrom
-is -includes -most severe manifestation |
-the most common cause of mental retardation
-includes microcephaly and congenital heart disease -holoprosencephaly |
|
|
Holoprosencephaly
-results from |
-Failure of midline cleavage of the embryonic forebrain.
-The telencephalon contains a singular ventricular cavity -is seen in trisomy 13 (Patua syndrome) -The corpus callosum may be absent -is the most severe manifestation of the fetal alcohol syndrome |
|
|
The 3 Primary Brain Vesicles
|
-Forebrain (prosencephalon)
-Midbrain (mesencephalon) -Hindbrain (rhombencephalon) |
|
|
Forebrain (prosencephalon)
-gives rise to |
-Telencephalon
-Diencephalon |
|
|
Midbrain (mesencephalon)
-gives rise to |
-Mesencephalon
|
|
|
Hindbrain (rhombencephalon)
-gives rise to |
-Metencephalon
-Myelencephalon |
|
|
Telencephalon
-adult derivatives of -Walls -Cavities |
Walls-Cerebral hemispheres
Cavities-Lateral ventricles |
|
|
Diencephalon
-adult derivatives of -Walls -Cavities |
Walls-Thalamus
Cavities-Third Ventricle |
|
|
Mesencephalon
-adult derivatives of -Walls -Cavities |
Walls-Midbrain
Cavities-Aqueduct |
|
|
Metencephalon
-adult derivatives of -Walls -Cavities |
Walls-Pons and Cerebellum
Cavities-Upper part of 4th ventricle |
|
|
Myelencephalon
-adult derivatives of -Walls -Cavities |
Walls-Medulla
Cavities-Lower Part of 4th ventricle |
|
|
Arnold-Chiari Malformation
-Common Anomalies |
-beaking of the tectal plate
-aqueductal stenosis -kinking and transforaminal herniation of the medulla into the vertebral canal -herniation and unrolling of the cerebellar vermis into the vertebral canal -an accompanying meningomyelocele is common |
|
|
Dandy-Walker Malformation
-get -common anomalies |
-Enormous Dilation of the 4th ventricle results from failure of the foramina of Luschka and Magendie to open
-Associated with occipital meningocele, elevation of the confluence of sinuses, agenesis of the cerebellar vermis, and splenium of the corpus collosum |
|
|
Psuedounipolar neurons
-located |
-In the spinal dorsal root ganglia and sensory ganglia of cranial nerves V, VII, IX, and X
|
|
|
Olfactory Neurons
-are |
bipolar and unmyelinated
|
|
|
Auditory Neurons
-are |
bipolar and myelinated
|
|
|
Dorsal root ganglion cells
-are |
pseudounipolar and myelinated
|
|
|
Motor Neurons
-are |
multipolar and myelinated
|
|
|
Bipolar neurons
-found in |
cochlear and vestibular ganglia of CN VIII, in the olfactory nerve (CN I), and in the retina
|
|
|
Fast Anterograde Axonal Transport
-responsible -rate -mediated by |
-For transporting all newly syntehsized membranous organelles (vesicles) and precursors of neurotransmitters
-200 to 400 mm/day -neurotubules and kinesis (fast transport is neurotubule-dependent) |
|
|
Slow Anterograde Transport
-responsible -rate |
-For transporting fibrillar cytoskeletal and protoplasmic elements
-1 to 5 mm/day |
|
|
Fast Retrograde Transport
-responsible -rate -transports -mediated by |
-Returns used materials from the axon terminal to the cell body for degradation and recycling
-100 to 200 mm/day -Nerve growth factor, neurotropic viruses, and toxins, such as herpes simplex, rabies, poliovirus, and tetanus toxin -neurotubules and dynein |
|
|
Wallerian Degneration
-is -occurs |
Is anterograde degeneration characterized by the disappearance of axons and myelin sheaths and the secondary proliferation of Schwann cells
-In the Central Nervous System and the Peripheral Nervous System |
|
|
Chromatolysis
-is -occurs |
-The result of retrograde degeneration
-in neurons of the CNS and PNS -There is a loss of nissl substance after axotomy |
|
|
Why regeneration doesnt occur in the CNS
|
-there are no basement membranes or endoneural investments surrounding the axons of the CNS
|
|
|
Regeneration of Nerve Cells
-In -Process -Rate |
In PNS
-The proximal tip of a severed axon grows into the endoneural tube, which consists of Schwann cell basement membrane and endoneurium -The axon sprout grows at the rate of 3 mm/day |
|
|
2 biochemical markers for Astrocytes
|
Glial Fibrillary Acidic Protein (GFAP) and glutamine synthetase
|
|
|
Blood-Brain Barrier
-consists of |
-Tight junctions of nonfenestrated endothelial cells; some authorities include the astrocytic foot processes
-Infarction of brain tissue destroys the tight junctions of endothelial cells and results in vasogenic edema, which is an infiltrate of plasma into the extracellular space |
|
|
Blood-CSF Barrier
-consists of |
-Tight Junctions between the Cuboidal Epithelial clls of the choroid plexus.
-The barrier is permeable to some circulating peptides (insulin) and plasma proteins (prealbumin) |
|
|
Lewy bodies
|
are neuronal inclusions that are characteristic of Parkinson's disease
|
|
|
Negri bodies
-where found |
-In the pyramidal cells of the hippocampus and the Purkinje cells of the cerebellum
|
|
|
Hirano bodies
|
are intraneuronal, eosinophilic, rodlike inclusions that are found in the hippocampus of patients with Alzheimer's disease
|
|
|
Neurofibrillary tangles
|
consist of intracytoplasmic degenerated neurofilaments. They are seen in patients with Alzheimer's disease
|
|
|
Sensory Axons
-Ia (A-alpha) -diameter -function |
-12-20 micrometers
-protprioception, muscle spindles |
|
|
Sensory Axons
-Ib (A-alpha) -diameter -function |
-12-20 micrometers
-proprioception, golgi tendon organs |
|
|
Sensory Axons
-II (A-beta) -diameter -function |
-5-12 micrometers
-touch, pressure, and vibration |
|
|
Sensory Axons
-III (A-delta) -diameter -function |
-2-5 micrometers
-touch, pressure, fast pain, and temperature |
|
|
Sensory Axons
-IV (C) -diameter -function |
-0.5-1 micrometers
-slow pain and temperature, unmyelinated fibers |
|
|
Motor axons
-Alpha (A-alpha) -diameter -where at -innervate |
-12-20 micrometers
-Alpha motor neurons of ventral horn -(innervate extrafusal muscle fibers) |
|
|
Motor axons
-Gamma (A-gamma) -diameter -where at -innervate |
-2-10 micrometers
-Gamma motor neurons of ventral horn -(innerate intrafusal muscle fibers) |
|
|
Preganglionic autonomic fibers (B)
|
myelinated preganglionic autonomic fibers
|
|
|
Postganglionic autonomic fibers (C)
|
unyelinated postganglionic autonomic fibers
|
|
|
Metastatic Brain tumors
-most common locations |
-in metastatic tumors, the primary site of malignancy is the lung in 35% of cases, the breast in 17%, in the GI tract in 6% melanoma in 6%, and the kidney in 5%
|
|
|
Glioblastoma multiforme
-is |
the most common and most fatal type of brain tumor
|
|
|
Meningioma
-is |
a benign noninvasive tumor of the falx and the convexity of the hemisphere
|
|
|
Schwannoma
-is |
a benign peripheral tumor derived from Schwann cells
|
|
|
Ependymoma
-is |
found in the ventricles and accounts for 60% of spinal cord gliomas
|
|
|
Medulloblastoma
-is |
the second most common posterior fossa tumor seen in children and may metastasize through the CSF tracts
|
|
|
Cutaneous Receptors
-Meissner's corpuscles -Pacinican corpuscles |
-Meissner's corpuscles are encapsulated endings that are touch receptors
-Pacinian Corpuscles are pressure and vibration receptors |
|
|
Dorsal Columns
-aka |
Medial Lemniscus Pathway
|
|
|
Dorsal Columns
-function |
mediates
-tactile discrimination -vibration sensation -form recognition -joint and muscle sensation (conscious proprioception) |
|
|
Dorsal Columns
-receptors |
-Pacini's and Meissner's tactile corpuscles
-joint receptors -muscle spindles -golgi tendon organs |
|
|
Dorsal Columns
-first-order neurons located in |
the dorsal root ganglia at all levels. They project axons to he spinal cord through the medial root entry zone
|
|
|
Dorsal Columns
-first-order neurons give rise to |
-the gracile fasciculus from the lower extremity
-the cuneate fasciculus from the upper extremity -the collaterals for spinal reflexes (myotatic reflex) -the axons that ascend in the dorsal columns and terminate in the gracile and cuneate nuclei of the causal medulla |
|
|
Dorsal Columns
-second-order neurons are located |
-in the gracile and cuneate nuclei of the caudal medulla
|
|
|
Dorsal Columns
-second-order neurons -give rise to |
-axons and internal arcuate fibers that decussate and form a compact fiber bundle (medial lemniscus)
|
|
|
Dorsal Columns
-second-order neurons -medial lemniscus-pathway |
-ascends through the contralateral brain stem and terminates in the VPL nucleus of the thalamus
|
|
|
Dorsal Columns
-third-order neurons -located |
in the VPL nucleus of the thalamus
|
|
|
Dorsal Columns
-third-order neurons -project |
through the posterior limb of the internal capsule to the postcentral gyrus, which is the primary somatosensory cortex (Brodmann's areas 3, 1, and 2)
|
|
|
Dorsal Columns
-transection of the dorsal column-medial lemniscus tract -above the sensory decussation |
transection results in contralateral loss of the dorsal column modalities
|
|
|
Dorsal Columns
-transection of the dorsal column-medial lemniscus tract -in the spinal cord |
transection results in ipsilateral loss of the dorsal column modalities
|
|
|
Dorsal Columns
-crosses where -uses what |
-at the causal medulla
-internal arcuate fibers that decussate and form medial lemniscus |
|
|
Lateral Spinothalamic Tract
-function |
-the lateral spinothalamic tract medates pain and temperature sensation
|
|
|
Lateral Spinothalamic Tract
-receptors |
are free nerve endings. The lateral spinothalamic tract receives input from fast- and slow-conducting pain fibers (A-delta and C, rspectively)
|
|
|
Lateral Spinothalamic Tract
-first-order neurons -located -project to |
-in the dorsal root ganglia at all levels
-project axons to the spinal cord through the dorsolateal tract of Lissauer (lateral root entry zone) to second-order neruons |
|
|
Lateral Spinothalamic Tract
-Second-order neurons -located -give rise to -axons terminate in the |
-found in dorsal horn
-they give rise to axons that decussate in the vental white commissure and ascend in the contralateral lateral funiculus -their axons terminate in the VPL of the thalamus |
|
|
Lateral Spinothalamic Tract
-Third-order neurons -located -project |
-are found in the VPL nucleus of the thalamus
-project through the posterior limb of the internal capsule to he primary somatosensory cortex (Brodmann's areas 3,1, and 2) |
|
|
Lateral Spinothalamic Tract
-transection of the lateral spinothalamic tract |
results in contralateral loss of pain and temperature below the lesion
|
|
|
Lateral Corticospinal Tract
-function |
-Mediates voluntary skilled motor activity, primarily of the upper limbs. It is not fully myelinated until the end of the second year (Babinski's sign)
|
|
|
Lateral Corticospinal Tract
-fiber caliber |
approximately 90% of the fibers lie between 1 and 4 micrometers and 4% lie above 20 micrometers (from the giant cells of Betz)
|
|
|
Lateral Corticospinal Tract
-origin |
-arises from layer V of the cerebral cortex from three cortical areas in equal aliquots:
-the premotor cortex (Brodmann's area 6) -The primary motor cortex (Brodmann's area 4) -The primary sensory cortex (Brodmann's areas 3, 1, and 2) -The arm and face areas of the motor homunculus arise from the lateral convexity; the foot region of the motor homunculus is found in the paracentral lobule |
|
|
Lateral Corticospinal Tract
-termination |
The lateral corticospinal tract terminates contralaterally, through interneurons, on ventral horn motor neurons
|
|
|
Lateral Corticospinal Tract
-course -Telencephalon |
-Telencephalon-the lateral coricospinal tract runs in the posterior limb of the internal capsule in the tlencephalon
|
|
|
Lateral Corticospinal Tract
-course -Midbrain |
-Midbrain-the lateral corticospinal tract runs in the middle 3/5 of the crus cerebri in the midbrain
|
|
|
Lateral Corticospinal Tract
-course -Pons |
the lateral corticospinal tract runs in the base of the pons
|
|
|
Lateral Corticospinal Tract
-course -medulla |
-The lateral corticospinal tract runs in the medullary pyramids.
-Between 85% and 90% of the corticospinal fibers decussate in the pyramidal decussation as the lateral corticospinal tract. -The remaining 10% to 15% of the fibers continue as the anterior corticospinal tract |
|
|
Lateral Corticospinal Tract
-course -spinal cord |
The lateral corticospinal tract runs in the dorsal quadrant of the lateral funiculus
|
|
|
Lateral Corticospinal Tract
-transection of the lateral corticospinal tract -above the motor decussation |
transection results in the contralateral spastic paresis and Babinski's sign (upgoing toe)
|
|
|
Lateral Corticospinal Tract
-transection of the lateral corticospinal tract -in the spinal cord |
-trasection results in ipsilateral spastic paresis and Babinski's sign
|
|
|
Hypothalamospinal Tract
-anatomic location |
Projects without interruption from the hypothalamus to the ciliospinal center of the intermediolateral cell column at T1 to T2.
-It is found in the spinal cord at T1 or above in the dorsolateral quadrant of the lateral funiculus. -It is also found in the lateral tegmentum of the medulla, pons, and midbrain. |
|
|
Hypothalamospinal Tract
-clinical features |
-Interruption of this tract at any level results in Horner's syndrome
-(miosis, ptosis, hemianhidrosis, and apparent enopthalmos) -the signs are always ipsilateral |
|
|
Upper Motor Neuron Lesions
-caused by |
transection of the corticospinal tract or destrufction of the cortical cells of origin
|
|
|
Upper Motor Neuron Lesions
-result in |
spastic paresis with pyramidal signs (Babinski's sign)
|
|
|
Lower Motor Neuron Lesions
-caused by |
damage to the motor neurons
|
|
|
Lower Motor Neuron Lesions
-result in |
-flaccid paralysis, areflexia, atrophy, fasciculations, and fibrillations
-Poliomyelitis or Werdnig-Hoffman disease results from damage to the motor neurons |
|
|
Amyotrophic Lateral Sclerosis
-aka -is -caused by -have no |
-ALS, or Lou Gehrig's Disease
-is a combined UMN and LMN disease -ALS is couased by damage to the corticospinal tracts, with pyramidal signs, and by damage to the LMNs, with LMN symptoms -Patinets with ALS have no sensory deficits |
|
|
Patients with neurosyphilis
-get what -characterized by |
-dorsal colum disease (tabes dorsalis)
-characterized by a loss of tactile discrimination and position and vibration sensation. -Patients have a Romberg sign (subject stands with his feet together. when he closes his eyes, he loses his balance. This is a sign of dorsal column ataxia) |
|
|
Ventral Trigeminothalamic Tract
-mediates |
Pain and temperature sensation from the face and oral cavity
|
|
|
Dorsal Trigeminothalamic Tract
-mediates |
Tactile discrimination and pressure sensation from the face and oral cavity. It receives input from Meissner's and Pacini's corpuscles
*This tract is both crossed and uncrossed |
|
|
Corneal Reflex
-Afferent Limb -Efferent Limb |
-Opthalmic Nerve (V-1)
-Facial Nerve (VII) |
|
|
Jaw Jerk
-Afferent Limb -Efferent Limb |
-Mandibular Nerve (V-3)
-Mandibular Nerve (V-3) |
|
|
Tearing (lacrimal) Reflex
-Afferent Limb -Efferent Limb |
-Opthalmic Nerve (V-1)
-Facial Nerve (VII) |
|
|
Oculocardiac Reflex
-Afferent Limb -Efferent Limb |
-Opthalmic Nerve (V-1)
-Vagal Nerve (X) |
|
|
Audiotry system
-derived from |
-The otic vesicle, which is a derivative fo the otic placode, a thickening of the surface ectoderm
|
|
|
In Normal ears,
-Weber Test shows -Rinne Test shows |
-no lateralization
-AC>BC, both ears |
|
|
In Conduction deafness of left ear
-Weber Test shows -Rinne Test shows |
-lateralizes to left ear
-BC>AC on left -AC>BC on right |
|
|
In Conduction deafness of right ear
-Weber Test shows -Rinne Test shows |
-Lateralizes to right ear
-BC>AC on right -AC>BC on left |
|
|
In Nerve deafnessof left ear
-Weber Test shows -Rinne Test shows |
-lateralizes to right ear
-AC>BC, both ears |
|
|
In Nerve deafness of right ear
-Weber Test shows -Rinne Test shows |
-lateralizes to left ear
-AC>BC, both ears |
|
|
Vestibular System
-function |
-Maintains posture and equilibrium and coordinates head and eye movements
|
|
|
Vestibular (horizontal) Nystagmus
-Fast Phase-in direction of -Slow Phase-in direction of |
-Direction of Rotation
-Opposite of Rotation |
|
|
Postrotatory (horizontal) Nystagmus
-Fast Phase-in direction of -Slow Phase-in direction of |
-Oppostie of Rotation
-Direction of rotation -The patient past-points and falls in the direction of previous rotation |
|
|
Caloric Nystagmus (stimulation of horizontal ducts) in Normal Patients
-Cold Water Irrigation-in direction of -Warm Water Irrigation-in direction of |
-To opposite side
-To same side |
|
|
Test Results in Unconscious subjects
|
-No nystagmus is seen
-When the brain stem is intact, there is deviation of the eyes to the side of the cold irrigation -With bilateral MLF transection, there is deviation of the abducting eye to the side of cold irrigation -With lower brain stem damage to the vestibular nuclei, there is no deviation of the eyes |
|
|
Lesions of the parahippocampal uncas
|
may cuase olfactory hallucinations [uncinate fits (seizures) with deja vu]
|
|
|
CN 3
-function |
-moves the eye, constricts the pupil, accomodates, and converges
|
|
|
Eye muscles
-SIN mnemonic |
-Superior muscles are intorters of the globe
|
|
|
Medial rectus muscle
-function |
adducts the eye
|
|
|
Superior rectus muscle
-function |
elevates, intorts, and adducts the eye
|
|
|
Inferior rectus muscle
-function |
depresses, extorts, and adducts the eye
|
|
|
Inferior oblique muscle
-function |
elevates, extorts, and abducts the eye
|
|
|
Levator palpebrae muscle
-function |
elevates the upper eyelid
|
|
|
Edinger-Westphal nucleus
-projects |
preganglionic parasympathetic fibers to the ciliary ganglion of the orbit through CN III
|
|
|
Ciliary Ganglion
-projects |
postganglionic parasympathetic fibers to the sphincter muscle of the iris (miosis) and the ciliary muscle (accomodation)
|
|
|
Oculomotor paralysis (palsy)
-seen with |
transtentorial herneiation (tumor, subdural or epidural hematoma)
|
|
|
Denervation of the levator palpebrae muscle
-causes |
pstosis-drooping of the upper eyelid
|
|
|
Denervation of the extraocular muscles
-causes |
-the affected eye to look "down and out" as a result of the unopposed action of the lateral rectus and superior oblique muscles
|
|
|
Superior Oblique Muscles
-innervated by |
CN IV
|
|
|
Lateral Rectus Muscles
-innervated by |
CN VI
|
|
|
Oculomotor Palsy
-causes |
diplopia (double vision) when the patient looks in the direction of the paretic muscle
|
|
|
Interruption of parasympathetic innervation (internal opthalmoplegia)
-results in |
a dilated, fixed pupil and paralysis of accommodation (cycloplegia)
|
|
|
Transtentorial (uncal) herniation
-what happens |
increased supratentorial pressure (from a tumor) forces the hippocampal uncus through the tentorial notch and compresses or stretches the oculomotor nerve
|
|
|
Transtentorial (uncal) herniation
-results in |
-Pupilloconstricot fibers are affected first, resulting in a dilated, fixed pupil
-Somatic efferent fibers are affected later, resulting in external strabismus (extropia) |
|
|
Trochlear Nerve
-innervates |
Superior Oblique Muscle
|
|
|
Superior Oblique Muscle
-function |
depresses, intorts, and abducts the eye
|
|
|
CN IV paralysis
-results in |
-Extorsion of the eye and weakness of downward gaze
-vertical diplopia, which increases when looking down -head tilting to compensate for extorsion (may be misdaignosed as idiopathic torticollis) |
|
|
Trigeminal nerve
-derived from -divisions |
-Pharyngeal (brachial) arch 1
-Opthalmic, Maxillary, Mandibular |
|
|
CN VI paralysis
-is -seen |
-The most common isolated palsy that results from the long peripheral course of the nerve
-Seen in patients with meningitis, subarachnoid hemorrhage, late-stage syphilis, and trauma |
|
|
Abducent nerve paralysis
-results in |
-Convergent (medial) strabismus (esotropia) with inability to abduct the eye
-Horizontal diplopia with maximum separation of the double images when looking toward the paretic lateral rectus muscle |
|
|
CN VII
-functions |
-mediates facial movements
-taste -salivation -lacrimation -general sensation from the external ear |
|
|
CN VII
-derived from |
Pharyngeal (brachial) arch 2
|
|
|
CN VII
-and taste |
-it innervates the taste buds from the anterior 2/3 of the tongue
|
|
|
Solitary tract
-for -what nerves |
-Tastes
-VII, IX, X |
|
|
Vestibulocochlear Nerve (CN VIII)
-2 divisions and their function |
-vestibular-maintains equilibrium and balance
-cochlear-mediates hearing |
|
|
Vestibular Nerve
-lesions-result in |
-disequilibrium
-vertigo -nystagmus |
|
|
Cochlear Nerve
-lesions-result in |
-destructive lesions cause hearing loss (sensorineural deafness)
-irritative lesions can cuase tinnitus (ear ringing) -an acoustic neuroma is a Schwann cell tumor of the cochliar nerve that cuases deafness |
|
|
CN IX
-function |
-Along with CN X, XI, and XII, it mediates taste, salivation, and swallowing
-it mediates input from the carotid sinus, whcih contains baroreceptors that monitor arterial blood pressure -it also mediates input from he carotid body, which contains chemoreceptors that monitor the CO2 and O2 concentration of the blood |
|
|
CN IX
-derived from |
-pharyngeal (brachial) arch 3
|
|
|
what nerve does taste from posterior 1/3 of tongue
|
CN IX
|
|
|
CN IX
-lesions-result in |
-loss of general sensation in the pharynx, tonsils, fauces, and the back of the tongue
-loss of afferent limb of gag reflex -loss of taste from posterior 1/3 of tongue |
|
|
CN X
-mediates -innervates |
-phonation, swallowing (with IX, XI, XII), elevation of the palate, taset, and cutaneous sensation from the ear
-viscera of the neck, thorax, and abdomen |
|
|
CN X
-derived from |
-the pharyngeal (brachial) arches of 4 and 6
|
|
|
CN XI
-mediates |
-head and shoulder movement and innervates the laryngeal muscles
|
|
|
Medial Medullary Syndrome (anterior spinal artery syndrome
-affected structures and resultant deficits include: |
-corticospinal tract (medullary pyramid)-lesions result in contralateral spastic hemiparesis
-medial lemniscus-lesions result in contralateral loss of tactile and vibration sensation from the trunk and extremities -hypoglossal nucleus or intraaxial root fibers-lesion reults in ipsilateral flccid hemiparalysis of the tongue. |
|
|
Lateral Medullary Syndrome (PICA)
-things affected |
-vestibular nuclei
-inferior cerebellar peduncle -nucleus ambiguus of CN IX, X, XI -glossopharyngeal nerve roots -vagal nerve roots -spinothalamic tracts (spinal lemniscus) -spinal trigeminal nucleus and tract -descending sympathetic tract |
|
|
Lateral Medullary Syndrome (PICA)
-vestibular nuclei-see |
nystagmus, nausea, vomiting, and vertigo
|
|
|
Lateral Medullary Syndrome (PICA)
-inferior cerebellar peduncle-see |
-ipsilateral cerebellar signs-dystaxia, dysmetria (past pointing), dysdiadochokinesia
|
|
|
Lateral Medullary Syndrome (PICA)
-nucleus ambiguus of CN IX, X and XI-see |
ipsilateral laryngeal, pharyngeal, and palatal hemiparalysis (loss of gag reflex-efferent limb), dysarthria, dysphagia, and dysphonia (hoarseness)
|
|
|
Lateral Medullary Syndrome (PICA)
-glossopharyngeal nerve roots-see |
-lesions result in loss of the gag reflex (afferent limb)
|
|
|
Lateral Medullary Syndrome (PICA)
-vagal nerve roots-see |
-same deficits as seen in lesions involving the nuclesu ambiguus:
ipsilateral laryngeal, pharyngeal, and palatal hemiparalysis (loss of gag reflex-efferent limb), dysarthria, dysphagia, and dysphonia (hoarseness) |
|
|
Lateral Medullary Syndrome (PICA)
-spinothalmic tracts (spinal lemniscus)-see |
contralateral loss of pain and temperature sensation from the trunk and extremities
|
|
|
Lateral Medullary Syndrome (PICA)
-spinal trigeminal nucleus and tract-see |
-ipsilateral loss of pain and temperature sensation from the face (facial hemianesthesia)
|
|
|
Lateral Medullary Syndrome (PICA)
-descending sympathetic tract-see |
ipsilateral Horner's syndrome
|
|
|
Medial Inferior Pontine Syndrome
-results from |
occlusion of the paramedian branches of the basilar artery
|
|
|
Medial Inferior Pontine Syndrome
-structures affected and resultant deficits |
-cortiocpinal tract-contralateral spastic hemiparesis
-medial lemniscus-contralateral loss of tactile sensation from the trunk and extremities -abducent nerve roots-ipsilateral lateral rectus palsies |
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-structures affected |
-facial nucleus
-cochlear nuclei -vestibular nuclei -spinal trigeminal nucleus and tract -middle and inferior cerebellar peduncles -spinothalamic tracts -descending sympathetic tract |
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-facial nuclues -deficit |
-ipsilateral facial nerve paralysis
-ipsilateral loss of taste from teh anterior 2/3 of tongue -ipsilateral loss of lacrimation and reduced salivation -loss of corneal and stapedial reflexes (efferent limbs) |
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-cochlear nuclie -deficit |
-unilateral central deafness
|
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-vestibular nuclei -deficit |
nystagmus, nausea, vomiting, and vertigo
|
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-spinal trigeminal nucleus and tract -deficit |
-ipsilateral loss of pain and temperature sensation from the face
|
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-middle and inferior cerebellar peduncles -deficit |
-ipsilateral limb and gait dystaxia
|
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-spinothalamic tracts (spinal lemniscus) -deficit |
contralateral loss of pain and temperature sensatino from the trunk and extremities
|
|
|
Lateral Inferior Pontine Syndrome (AICA syndrome)
-descending sympathetic tract -deficit |
-ipsilateral Horner's syndrome
|
|
|
Medial Longitudinal Fasciculus (MLF) syndrome
-aka |
internuclear ophthalmoplegia
|
|
|
Medial Longitudinal Fasciculus (MLF) syndrome
-see |
interrupts fibers from the contralateral abducent nucleus that project through the MLF to the ipsilateral medial rectus subnucleus of CN III
|
|
|
Medial Longitudinal Fasciculus (MLF) syndrome
-causes |
-medial rectus palsy on attempted lateral conjugate gaze
-nystagmus in the abducting eye -convergence remains intact |
|
|
Medial Longitudinal Fasciculus (MLF) syndrome
-syndrome often seen in patients with |
multiple sclerosis
|
|
|
Parinaud's Syndrome
-often resultant of |
a pinealoma or germinoma of the pineal region
|
|
|
Parinaud's Syndrome
-affected structures and resultant deficits |
-superior colliculus and pretectal area-lesions cause paralysis of upward and downward gaze, pupillary disturbances, and absence of convergence
-cerebral aqueduct-compression causes noncommunicating hydrocephalus |
|
|
Acoustic Neuroma (Schwannoma)
-is |
-a benign tumor of Schwann cells that affects the vestibulocochlear nerve.
-it is a posterior fossa tumor of the internal auditory meatus and cerebellopontine angle |
|
|
Acoustic Neuroma (Schwannoma)
-often compresses |
-the facial nerve (CN VII), which accompanies CN VIII in the cerebellopontine angle and internal auditory meatus
|
|
|
Acoustic Neuroma (Schwannoma)
-affected structures and deficits |
-cochlear of VIII-tinnitus and unilateral nerve deafness
-vestibular of VIII-vertigo, nystagmus, nausea, vomiting, unsteadiness of gain -VII-facial weakness and loss of efferent limb of corneal reflex -spinal trigeminal tract-paresthesia, anesthesia of ipsilateral face, loss of afferent limb of corneal reflex |
|
|
Acoustic Neuroma (Schwannoma)
-often accompanied by |
-Neurofibromatosis type 2 often occurs with bilateral neuromas
|
|
|
Locked-In Syndrome
-is |
a lesion of the base of the pons as the result of infarction, trauma, tumor, or demyelination
|
|
|
Locked-In Syndrome
-affected tracts |
-corticospinal and corticobulbar tracts are affected bilaterally
-oculomotor and trochlear nerves are not injured -patients are conscious and may communicate through vertical eye movements |
|
|
Subclavian Steal Syndrome
-results from |
thrombosis of the left subclavian artery proximal to the vertebral artery
|
|
|
Subclavian Steal Syndrome
-blood shunted |
-retrograde down the left vertebral artery and into the left subclavian artery
|
|
|
Subclavian Steal Syndrome
-clinical signs |
-transient weakness and claudication of the left arm on exercise
-vertebrobasialar insufficiency |
|
|
3 main functions of the cerebellum
|
-maintenance of posture and balance
-maintenance of muscle tone -coordination of voluntary motor activity |
|
|
Cerebellar Cortex has 3 layers
|
-molecular layer-contains stellate and basket cells, and the dendritic arbor of the Purkinje cells
-purkinje cell layer-lies between the molecular and granule layer -granule layer-inner layer overlying the white matter. Contains granule cells, Golgi cells, and cerebellar glomeruli (consists of a mossy fiber roseete, granule cell dendrites, and a Golgi cell axon. |
|
|
Cerebellum
-purkinje cells |
-convey the only output from the cerebellar cortex.
-project inhibitory output to the cerebellar and vestibular nuclei |
|
|
Cerebellum
-excited by -inhibited by |
-are excited by parallel and climbing fibers
-inhibited by GABA-ergic basket and stellate cells |
|
|
Cerebellum
-Granule cells -excite |
-by way of glutamate-purkinje, basket, stellate, and golgi cell through parallel fibers
|
|
|
Cerebellum
-Granule cells -inhibited by -excited by |
-inhibited by golgi cells
-excited by mossy fibers |
|
|
Cerebellum
-Parallel fibers -are -extend |
-the axons of granule cells
-extend into the molecular layer |
|
|
Cerebellum
-Mossy Fibers -are |
-the afferent excitatory fibers of the spinocerebellar, pontocerebellar, and vestibulocerebellar tracts
|
|
|
Cerebellum
-Mossy Fibers -terminate |
-as mossy fiber rosettes on granule cell dendrites
|
|
|
Cerebellum
-Mossy Fibers -excite |
-granule cells to discharge through their parallel fibers
|
|
|
Cerebellum
-Climbing Fibers -are |
-the afferent excitatory (by way of aspartate) fibers of the olivocerebellar tract
|
|
|
Cerebellum
-Climbing Fibers -arise from |
-contralateral inferior olivary nucleus
|
|
|
Cerebellum
-Climbing Fibers -terminate |
-on neurons of the cerebellar nuclei and dendrites of Purkinje cells
|
|
|
The Major Cerebellar Pathway
|
-Purkinje cells of the cerebellar cortex project to the cerebellar nuclei
-Dentate nucleus gives rise to the dentatothalamic tract-projects through the superior cerebellar peduncel to the contralateral ventral lateral nucleus of the thalamus -ventral lateral nucleus of the thalamus projects to the primary motor cortex of the precentral gyrus (area 4) -motor cortex projects as the corticopontine tranct to the pontine nuclei -pontine nuclei projects as the pontocerebellar tract to thte contralateral cerebellar cortex, where they terminate as mossy fibers |
|
|
Cerebellar Nuclei
|
dentate, emboliform, globose and fastigial
|
|
|
The major effector nucleus of he cerebellum
|
dentate nucleus-gives rise to the dentatothalamic tract-projects through the superior cerebellar peduncel to the contralateral ventral lateral nucleus of the thalamus
|
|
|
Anterior vermis syndrome
-results from -causes |
-atrophy of the rostral vermis, most commonly caused by alcohol abuse
-causes gait, trunk, and leg dystaxia |
|
|
Posterior vermis syndrome
-involves -result of -most commonly caused by -causes |
-flocculonodular lobe
-brain tumors in children -medulloblastomas or ependymomas -truncal dystaxia |
|
|
Thalamus
-is -role |
-the largest division of the diencephalon
-important role in the integration of the sensory and motor systems |
|
|
Thalamus
-anterior nucleus |
-part of the Papez circuit of emotion of the limbic system
|
|
|
Thalamus
-mediodorsal nucleus |
-when destroyed, memory loss occurs (Wernicke-Korsakoff syndrome)
-plays a role in the expression of affect, emotion, and behavior (limbic function) |
|
|
Thalamus
-pulvinar |
-largest thalamic nucleus
-it plays a role in the integration of visual, auditory, and somesthetic input -destruction of the dominant pulvinar mya result in sensory dysphasia |
|
|
Thalamus
-Ventral anterior/Ventral Lateral |
-motor
|
|
|
Thalamus
-VPL |
-receives fibers from spinothalamic tracts and the medial lemniscus
-it projects to the sensory cortex (Brodmann's 3, 1, 2) |
|
|
Thalamus
-VPM |
-receives fibers from the trigeminothalamic tracts
-projects to the sensory cortex (Brodmann's 3, 1, 2) -The gustatory (taste pathway originates in the solitary nucleus and projects via the central tegmental tract to VPM, and thence to the gustatory cortex of the postcentral gyrus (Brodmann's 3b) of the frontal operculum and insular cortex -the taste pathway is ipsilateral |
|
|
Thalamus
-Metathalamus -Lateral Geniculate Nucleus -Medial Geniculate Nucleus |
-LGN is a visual relay nucleus. It receives retinal input through the optic tract and projects to the primary visual cortex (Brodmann's 17)
-MGN-an auditory relay nucleus. It receives auditory input through the brachium of the inferior colliculus and projects to the primary auditory cortex (Brodmann's 41 and 42) |
|
|
Anterior limb of Internal Capsule
-located |
between caudate nucleus and the lentiform nucleus
|
|
|
Genu of Internal Capsule
-contains |
corticobulbar fibers
|
|
|
Posterior limb of Internal Capsule
-located |
between the thalamus and the lentiform nucleus.
|
|
|
Posterior limb of Internal Capsule
-contains |
corticospinal (pyramid) fibers as well as sensory (pain, temperature, and touch), visual, and auditory radiations
|
|
|
Anterior limb of Internal Capsule
-blood supply |
medial striate branches of the anterior cerebral artery and the lateral striate branches of the middle cerebral artery
|
|
|
Genu of Internal Capsule
-blood supply |
direct branches from the internal carotid artery or by pallidal branches of the anterior choroidal artery
|
|
|
Posterior limb of Internal Capsule
-blood suppy |
branches of the anterior choroidal artery and lenticulostriate branches of the middle cerebral arteries
|
|
|
transection of left upper division of geniculocalcarine tract (visual radiation)
-gives |
right contralateral lower quadrantanopia
|
|
|
transection of left lower division of geniculocalcarine tract (visual radiation)
-gives |
right contralateral upper quadrantanopia ("pie in the sky")
|
|
|
Pupillary Light Reflex Pathway
-afferent limb -efferent limb |
-afferent limb-CN II
-efferent limb-CN III |
|
|
Pupillary Light Reflex Pathway
-pathway |
-gaglion cells of the retina-project bilaterally to the pretectal nuclei
-the pretctal nucleus of the midbrain projects (through the posterior commisure) crossed and uncrossed fibers to the Edinger-Westphal nucleus -Edinger-Westphal nucleus of CN III-gives rise to preganglionic parasympathetic fibers. These fibers exit the midbrain and synapse with postganglionic parasympathetic neurons of the ciliary ganglion -Ciliary ganglion-gives rise to postganglionic parasympathetic fibers-innervate the sphincter muscle of the iris |
|
|
MLF syndrome/internuclear ophthalmoplegia
-damage to -causes |
-damage (demyelination) to the MLF between the abducent and oculomotor nuclei
-cuases medial rectus palsy on attempted lateral gaze and monocular horizontal nystagmus in the abducting eye -convergence is normal |
|
|
MLF syndrome/internuclear ophthalmoplegia
-most commonly seen in |
multiple sclerosis
|
|
|
One-and-a-half Syndrome
-consists of -whats messed up |
-bilateral lesions of the MLF and a unilateral lesion of the abducent nucleus
-on attempted lateral conjugate gaze, the only muscle that functions is the intact lateral rectus |
|
|
Argyll Robertson Pupil
-is -occurs in |
-the absence of a miotic reaction to light, both direct and consensual, with the preservation of a miotic reaction to near stimulus (accommodation-convergence)
-occurs in syphilis and diabetes |
|
|
Transtentorial (uncal) herniation
-occurs |
-as a result of increased supratentorial pressure, which is commonly caused by a brain tumor or hematoma (subdural or epidural)
|
|
|
Transtentorial (uncal) herniation
-pressure forces |
the parahippocampal uncus through the tentorial incisure
|
|
|
Transtentorial (uncal) herniation
-impacted uncus forces |
-the contralateral crus cerebri against the tentorial edge (Kernohan's notch) and puts pressure on the ipsilateral CN III and posterior cerebral artery
|
|
|
Transtentorial (uncal) herniation
-neurologic defects |
-Ipsilateral hemiparesis-occurs as a result of pressure on the corticospinal tract, which islocated in the contralateral crus cerebri
-a fixed and dilated pupil, ptosis, and a "down-and-out" eye are caused by pressure on the ipsilateral oculomotor nerve -Contralateral homonymous hemianopia is caused by compression of the posterior cerebral artery, which irrigates the visual cortex |
|
|
Megacolon
-absence of -occurs |
-ganglion cells in the myenteric plexus
-occurs when neural crest cells do not migrate into the colon |
|
|
Shy-Drager syndrome
-involves -characterized by |
-preganglionic sympathetic neurons from the intermediolateral cell column
-characterized by orthostatic hypotension, anhidrosis, impotence, bladder atonicity |
|
|
Major Hypothalamic Nuclei and Their Functions
-Paraventricular Nucleus |
-synthesizes ADH, oxytocin, and CRH
-gives rise to the supraopticohypophyseal tract, which projects to the neurohypophysis -regulates water balance (vonservation) -destruction causes diabetes insipidus |
|
|
Major Hypothalamic Nuclei and Their Functions
-Medial Preoptic Nucleus |
-regulates the release of gonadotropic hormones from the adenohypophysis
-contains the sexually dimorphic nucleus, the development of which depends on testosterone levels |
|
|
Major Hypothalamic Nuclei and Their Functions
-Suprachiasmatic Nucleus |
-receives direct input from the retina
-plays a role in the reuglation of circadian rhythms |
|
|
Major Hypothalamic Nuclei and Their Functions
-Anterior Nucleus |
-plays a role in temperature regulation
-stimulates the parasympathetic nervous system -destruction results in hyperthermia |
|
|
Major Hypothalamic Nuclei and Their Functions
-Supraoptic Nucleus |
-sythesizes ADH and oxytocin (similar to the paraventricular nucleus)
|
|
|
Major Hypothalamic Nuclei and Their Functions
-Dorsomedial Nucleus |
-in animals, savage behavior results when this nucleus is stimulated
-obesity when stimulated |
|
|
Major Hypothalamic Nuclei and Their Functions
-Ventromedial Nucleus |
-Satiety Center
-when stimulated, it inhibits the urge to eat -bilateral destrction results in hyperphagia, obesity, and savage behavior |
|
|
Hypothalamus
-is -helps to |
a division of the diencephalon that subserves 3 systems: the autonomic nervous system, endocrine system, and limbic system
-helps to maintain homeostasis |
|
|
Major Hypothalamic Nuclei and Their Functions
-Arcuate (infundibular) nucleus |
-contains neurons that produce factors that stimulate or inhibit the action of the hypothalamus
-this nucleus gives rise to the tuberohypophyseal tract, which terminates in the hypophyseal portal system of the infundibulum. -it contains neurons that produce dopamine (prolactin-inhibiting factor) |
|
|
Major Hypothalamic Nuclei and Their Functions
-Mamillary Nucleus |
-receives input from the hippocampla formation through the postcommissural fornix
-it projects to the anterior nucleus of the thalamus through the mamillothalamic tract -patients with Wernicke's encephalopathy, which is a thiamine (b1) deficiency, have lesions in the mamillary nucleus -lesions are also associated with alcoholism |
|
|
Major Hypothalamic Nuclei and Their Functions
-Posterior Hypothalamic Nucleus |
-Plays a role in thermal regulation (conservation and increased production of heat)
-lesions result in poikilothermia (inability to thermoregulate) |
|
|
Major Hypothalamic Nuclei and Their Functions
-Lateral Hypothalamic Nucleus |
-induces eating when stimulated
-lesions cause anorexia and starvation |
|
|
Major Fiber Systems of the Hypothalamus
-Fornix |
-the largest projection to the hypothalamus
-projects from the hippocampal formation to the mamillary nucleus, anterior nucleus of the thalamus, and septal area -fornix then projects from the septal area to the hipocampal formation |
|
|
Major Fiber Systems of the Hypothalamus
-Medial Forebrain bundle |
-traverses the entire lateral hypothalmic area
-interconnects the orbitofrontal cortex, septal area, hypothalmus, and midbrain |
|
|
Major Fiber Systems of the Hypothalamus
-Mamillothalamic tract |
-projects from the mamillary nuclei to the anterior nucleus of the thalamus (part of the Papez circuit)
|
|
|
Major Fiber Systems of the Hypothalamus
-Stria terminalis |
-the major pathway from the amygdala
-interconnects the septal area, hypothalamus, and amygdala |
|
|
Major Fiber Systems of the Hypothalamus
-Supraopticohypohysial Tract |
-conducts fibers from the supraoptic and paraventricular nuclei to the neurohypophysis, which is the release site for ADH and oxytocin
|
|
|
Major Fiber Systems of the Hypothalamus
-Tuberohypophysial (tuberoinfundibular) tract |
-conducts fibers from the arcuate nucleus to the hypophyseal portal system
|
|
|
Major Fiber Systems of the Hypothalamus
-Hypothalamospinal Tract |
-Contains direct descending autonomic fibers
-These fibers influence the preganglionic sympathetic neurons of the intermediolateral cell column and preganglionic neurons of the sacral parasympathetic nucleus -Interruption above the first throacic segment (T1) causes Horner's syndrome |
|
|
Anterior Hypothalamus
-excitatory efect on |
-the parasympathetic nervous system
|
|
|
Posterior hypothalamus
-excitatory effect on |
-the sympathetic nervous system
|
|
|
Anterior Hypothalamus
|
-regulates and maintains body temperature
-destruction cuases hyperthermia |
|
|
Posterior Hypothalams
|
-Helps to produce and conserve heat
-destruction causes inability to thermoregulate |
|
|
Paraventricular Nucleus
|
-synthesizes ADH, whcih controls water excretion by the kidneys
|
|
|
Hypothalamus and Food Intake
|
-Ventromedial Nucleus-when stimulated inhibits the urge to eat. Bilateral destruction results in hyperphagia, obesity, and savage behavior
-Lateral Hypothalamic Nucleus-when stimulated induces the uge to eat. Destruction causes starvation and emaciation |
|
|
Craniopharyngioma
-originates |
-a congenital tumor that originates from remnants of Rathke's puch
|
|
|
Craniopharyngioma
-is usually -is |
-calcified
-the most common supratentorial tumor in children and the most common cause of hypopituitarism in children |
|
|
Craniopharyngioma
-pressure on the chiasma -pressure on the hypothalamus |
-causes bitemporal hemianopia
-causes hypothalamic syndrome (adiposity, diabetes insipidus, disturbance of temperature regulation, somnolence) |
|
|
Limbic System
-considered |
-the anatomic substrate that underlies behavioral and emotional expression
-it is expressed through the hypothalamus by way of the autonomic nervous system |
|
|
Limbic System
-orbiotfrontal cortex |
-mediates the conscious perception of smell
-has reciprocal connections with the mediodorsal nucleus of the thalamus -it is interconnected through the medial forebrain bundle with the septal area and hypothalamic nuclei |
|
|
Limbic System
-mediodorsal nucleus of the thalamus |
-receives input from the amygdala and plays a role in affective behavior and memory
|
|
|
Limbic System
-limbic lone |
-includes the subcallosal area, paraterminal gyrus, cingulate gyrus and isthmus, and parahippocampal gyrus, which includes the uncus
-it contains, buried in the parahippocampal gyrus, the hippocampal formation and amygdaloid nuclear complex |
|
|
Limbic System
-hipocampal formation |
-functions in leraning, memory, and recognition of novelty
|
|
|
Limbic System
-hipocampal formation -major structures |
-dentate gyrus-contains granule cells that receive hipocampal input and project output to the pyramidal cells of the hippocampus and subiculum
-hippocampus (cornu Ammonis)-has a 3-layered archicortex. It contains pyramidal cells that project through the fornix to the septal area and hypothalamus -subiculum-receives input through the hippocampal pyramidal cells. It projects through the fornix to the mamillary nuclei and the anterior nucleus of the thalamus. |
|
|
Amygdaloid Complex
|
-a basal ganglion that underlies the parahippocampal uncus
|
|
|
Amygdaloid Complex
-stimulation causes -lesions cause |
-fear and signs of sympathetic overactivity
-placidity and hypersexual behavior |
|
|
Limbic Midbrain Nuclei and Associated Neurotransmitters
|
-Ventral Tegmental Area-dopamine
-Raphhe Nuclei-serotonin -Locus Ceruleus-norepinephrine |
|
|
-Ventral Tegmental Area
-neurotransmitter |
-dopamine
|
|
|
-Raphhe Nuclei
-neurotransmitter |
-serotonin
|
|
|
-Locus Ceruleus
-neurotransmitter |
-norepinephrine
|
|
|
Bilateral destruction or removal of the cingulate gyry causes
|
-loss of initiative and inhibition as well as dulling of the emotions.
-memory is unaffected |
|
|
Lesions of the anterior cingulate gyri cause
|
placidity
|
|
|
Cingulectomy is used to treat
|
severe anxiety and depression
|
|
|
Basal Ganglia
-components |
-caudate nucleus
-putamen -globus pallidus |
|
|
Grouping of the Basal Ganglia
-striatum -consists of |
-caudate nucleus
-putamen |
|
|
Grouping of the Basal Ganglia
-lentiform nucleus -consists of |
-globus pallidus
-putamen |
|
|
Grouping of the Basal Ganglia
-Corpus Striatum -consists of |
-Lentiform Nucleus (putamen and globus pallidus)
-Caudate nucleus |
|
|
Grouping of the Basal Ganglia
-Clasustrum -consists of |
-lies between the lentiform nucleus and the insular cortex
-it has recprocal connections between the sensory cortices |
|
|
The Striatal (extrapyramidal) Motor System
-plays a role in -also involved in |
-the initiation and execution of somatic motor activity, especially willed movement
-it is also involved in automatic stereotyped postural and reflex motor activity (ex normal subjects swing their arms when they walk) |
|
|
The Striatal (extrapyramidal) Motor System
-structure |
-neocortex
-striatum (cuadatoputamen, or neostriatum) -globus pallidus -subthalamic nucleus -substantia nigra (pars compacta and pars reticularis) -Thalamus (ventral anterior, ventral lateral, and centromedian nuclei) |
|
|
Parkinson's Disease
-is |
-a degenerative diseas that affects the substantia nigra and its projections to the striatum
|
|
|
Parkinson's Disease
-results |
-Parkinson's disease causes a depletion of dopamine in the substantia nigra nad striatum as well as a loss of melanin-containing dopaminergic neurons in the substantia nigra
|
|
|
Parkinson's Disease
-clinical signs |
-bradykinesia
-stooped posture -shuffling gait -cogwheel rigidity -pill-rolling tremor -masked facies -Lewy bodies are found in the melanin-containing neurons of the substatia nigra -progressive supranuclear palsy is associated with Parkinson disease |
|
|
Parkinson's Disease
-treatment |
-L-dopa
-surgical intervention includes pallidotomy (rigidity) and ventral thalomotomy (tremor) |
|
|
Methylphenyltetrahydropyridine (MPTP)-induced parkonsonism
|
-MPTP is an analog of meperidine (Demerol)
-it destroys dopaminergic neurons in the substantia nigra |
|
|
Huntington's disease
-is |
-an inherited autosomal dominant movement disorder that is traced to a single gene defect on chromosome 4
|
|
|
Huntington's disease
-associated with |
-degeneration of the cholinergic and gama-aminobutyric acid-ergic neurons of the striatum.
-accompanied by gyral atrophy in the frontal and temporal lobes |
|
|
Huntington's disease
-get |
-glutamate excitotoxicity
-GLU is released in the striatum and binds to its receptors on straital neurons resulting in an action potential. |
|
|
Huntington's disease
-how is glutamate removed |
-GLU is removed from the extracellular space by astrocytes.
|
|
|
Huntington's disease
-glutamate is bound -results in -this cascade of events |
-to the N-methyl-D-aspartate (NMDA) receptor
-results in an influx of calcium ions and subsequent cell death -this cascade of events with neuronal death most likely occurs in cerebrovascular accidents (stroke) |
|
|
Hemiballism
-is |
-a movement disorder that usually results from a vascular lesion of the subthalamic nucleus
|
|
|
Hemiballism
-lesion of what |
lesion of the subthalamic nucleus
|
|
|
Hemiballism
-clinical signs |
-violent contralateral flinging (ballistic) movements of one or both extremities
|
|
|
Hepatolenticular Degeneration
-aka |
Wilson's Disease
|
|
|
Wilson's Disease
-is |
-an autosomal recessive disorder that is caused by a defect in the metabolism of copper
-gene locus is on chromosome 13 |
|
|
Wilson's Disease
-clinical signs |
-choreiform or athetotic movements
-rigidity -wing-beating tremor (tremor is the most common neurologic sign) -deposition of copper in the cornea gives rise to the corneal Kayser-Fleischer ring -deposition of copper in the liver leads to multilobar cirrhosis |
|
|
Wilson's Disease
-lesions |
-are found in the lentiform nucleus
|
|
|
Wilson's Disease
-psychiatric symptms |
-psychosis
-personality disorders -dementia |
|
|
Wilson's Disease
-diagnosis based on |
-low serum ceruloplasmin
-elevated urinary excretion of copper -increased copper concentration in a liver biopsy specimen |
|
|
Wilson's Disease
-treatment |
-penicillamine, a chelator
|
|
|
Tardive Dyskinesia
-is |
-a syndrome of repetitive choreic movement that affects the face and trunk
|
|
|
Tardive Dyskinesia
-results from |
-phenothiazines
-butyrophenones -metoclopramide |
|
|
Neurotransmitters
-Acetylcholine -major transmittor of |
-peripheral nervous system
-neuromuscular junction -parasympathetic nervous system -preganglionic sympathetic fibers -postaganglionic sympathetic fibers that innervate sweat glands and some blood vessels in the skeletal muscle |
|
|
Neurotransmitters
-ACh -found in |
-the neurons of the somatic and visceral motor nuclei in the brain stem and spinal cord
-also found in the basal nucleus of Meynert, which degenerates in Alzheimer's disease |
|
|
What degenerates in Alzheimer's disease
|
-basal nucleus of Meynert
-so get decreased ACh |
|
|
What NT is depleted in Alzheimer's disease
|
Acetylcholine
|
|
|
What NT is depleted in Parkinson's disease
|
Dopamine
|
|
|
What NT is increased in schizophrenia
|
Dopamine
|
|
|
Dopamine increased in...
|
schizophrenia
|
|
|
Dopamine decreased in...
|
Parkinson's
|
|
|
Acetylcholine decreased in...
|
Alzheimer's
|
|
|
Dopamine is found where in the CNS
|
-arcuate nucleus of the hypothalamus
|
|
|
Dopamine Receptors
|
-D1-receptors are postsynaptic. They activate adenylate cyclase and are excitatory
-D2-receptors ar both postsynaptic and presynaptic. They inhibit adenylate cyclase and are inhibitory. -Antipsychotic drugs block D2 receptors |
|
|
-Antipsychotic drugs block what receptors
|
D2 receptors
|
|
|
Norepinephrine
-is |
-the transmitter of most postganglionic sympathetic neurons
-Antidepressant drugs enhance its transmission |
|
|
Antidepressant drugs enhance the transmission of what NT
|
norepinephrine
|
|
|
Norepinephrine
-plays a role in |
-anxiety states
-panic attacts are believed to result from paroxysmal discharges from the locus ceruleus. |
|
|
Norepinephrine
-receptors |
-most postsynaptic receptors of the locus ceruleus pathway are beta-1 or beta-2 receptors that activate adenylate cyclase and are excitatory
|
|
|
Norepinephrine
-found |
in locus ceruleus
|
|
|
Reduced Norepinephrine activity
-related to |
depression
|
|
|
Increased Norepinephrine activity
-related to |
mania
|
|
|
Serotonin
-found where |
raphe nuclei of the brain stem
|
|
|
when 5-HT activity is reduced,
|
-decreased levels of catecholamines cause depression and insomnia
|
|
|
when 5-HT activity is increased,
|
elevated levels of catecholamines cause mania
|
|
|
dysfunction of 5-HT may underlie
|
obsessive-compulsive disorder
|
|
|
Certain antidepressants work by
-doing what to 5-HT |
-increase 5-HT availability by reducing its reuptake
-5-HT agonists that bind 5-HT1A and those that block 5-HT2 have antiderpressant properties |
|
|
Fluoxetine
-is |
-a selective serotonin reuptake inhibitor (SSRI)
|
|
|
Endorphins
-found |
exclusively in the hypothalamus
|
|
|
Endorphins
-Beta-endorphin |
-the major endorphin found in the brain
-one of the most powerful analgesics known |
|
|
Enkephalins
-found |
-in the globus pallidus
-coexist with dopamine, GABA, NE, and ACh. -are colocalized in GABA-ergic pallidal neurons |
|
|
Enkephalins
-role |
play a role in pain suppression
|
|
|
Substance P
-role |
-plays a role in pain transmission
|
|
|
Substance P
-concentrated in |
-substantia nigra (highly concentrated)
-also found in the dorsal root ganglion cells and substantia gelatinosa |
|
|
Substance P
-colocalized with |
GABA in the striatonigral tract and plays a role in movemnt disorders
|
|
|
Substance P
-levels are reduced in |
-patients with Huntington's Disease
|
|
|
Somatostatin
-regulates the release of |
-growth hormone and thyroid-stimulating hormone
|
|
|
The concentration of somatostatin in the neocortex and hippocampus is significantly reduce in patients with
|
-Alzheimer's disease
|
|
|
somatostatin levels are increased in patients with
|
-Huntington's disease
|
|
|
Inhibitory amino acid transmitters
|
-GABA
-Glycine |
|
|
GABA
-is |
-the major inhibitory neurotransmitter of the brain
|
|
|
GABA
-receptors |
-GABA-A and GABA-B are intimately associated with bezodiazepine-binding sites
|
|
|
GABA
-benzodiazepines |
-enhance GABA activity
|
|
|
GABA
-GABA-A receptors |
-open chloride channels
|
|
|
GABA
-GABA-B receptors |
-are found on the terminals of neurons that use another transmitter (ie NE, DA, 5HT)
-activation of GABA-B receptors decreases the release of the other transmitter |
|
|
Glycine
-is |
-the major inhibitory neurotransmitter of the spinal cord
|
|
|
Glycine
-used by |
-used by the Renshaw cells of the spinal cord
|
|
|
Excitatory Amino Acid Transmitters
|
Glutamate and Aspartae
|
|
|
Glutamate
-is |
the major excitatory transmitter of the brain
|
|
|
Glutamate and NMDA receptors
|
glutamate, through its NMDA receptors plays a role in long-term potentiation ( a memory process) of hippocampal neurons
|
|
|
Glutamate plays a role in
|
-kindling and subsequent seizure activity
-under certain conditions, glutamate and its analogs are neurotoxic |
|
|
Alzheimer's Disease
-characterized histologically by |
-neurofibrillary tangles
-senile (neuritic) plaques -amyloid substance -granulovacuolar degeneration -Hirano bodies |
|
|
Myasthenia Gravis
-results from |
-autoantibodies against the nicotinic acetylcholine receptor on skeletal muscle
-these antiboides block the postganglionic acetylcholine bindgin site |
|
|
Myasthenia Gravis
-cardinal manifestation |
-fatigable weakness of the skeletal muscle
|
|
|
Myasthenia Gravis
-diagnosis |
-edrophonium or neostigmine injection
|
|
|
Lambert-Eaton Myasthenic Syndrome
-caused by |
-a presynaptic defect of acetylcholine release
|
|
|
Lambert-Eaton Myasthenic Syndrome
-causes |
-weakness in the limb muscles, but not the bulbar muscles
|
|
|
Lambert-Eaton Myasthenic Syndrome
-50% of cases are |
-associated with neoplams
|
|
|
Lambert-Eaton Myasthenic Syndrome
-in these patients, muscle strength |
-improves with use (vs those in Myasthenia Gravis in which muscle use results in fatigue)
|
|
|
Cerebral Cortex
-layers |
6 layers
-Layer 1-molecular -Layer 2-external granular -Layer 3-external pyramidal -Layer 4-internal granular -Layer 5-internal pyramidal -Layer 6-multiform layer |
|
|
Broca's Speeach Area
-Brodmann's numbers -located -destruction results in |
-44 and 45
-the posterior part of the inferior frontal gyrus in the dominant hemisphere -expressive, nonfluent aphasia (Broca's Aphasia) |
|
|
Sensory Cortex
-Brodmann's -destruction |
-3, 1, 2
-destruction results in contralateral hemihypesthesia and astereognosis |
|
|
Hippocampal cortex
-bilateral lesions result in |
-the inability to consolidate short-term memory into long-term memory
-earlier memories are retrievable |
|
|
Construction apraxia
|
the inability to draw or construct a geometric figure
|
|
|
hemineglect
|
-if the patient draws only the right half of the clock
-lesion is located in the right inferior parietal lobule |
|
|
Broca's Aphasia
|
-lesion in the frontal lobe, in the inferior frontal gyrus (Brodmann 44, 45)
-good comprehension -effortful speech -dysarthric speech -telegraphic speech -nonfluent speech -poor repetition -contralateral lower facial and upper limb weakness |
|
|
Wernicke's Aphasia
|
-lesion in the posterior temporal lobe, in the superior temporal gyrus (Brodmann 22)
-poor comprehension -fluent speech -poor repetition -Quadrantanopia -paraphasic errors-non sequiturs (L. does not follow) are statements irrelevant to the question askeed, neologism are words with no meaning, driveling speech |
|
|
Conduction Aphasia
|
transection of the arcuate fasciculus; the arcuate fasciculus interconnects Brodmann's speech area with Wernicke's speech area
-poor repetion -good comprehension -fluent speech |
|
|
Transcortical Motor Aphasia
|
-poor comprehension
-good repetition -nonfluent speech |
|
|
Transcortical Mixed Aphasia
|
-poor comprehension
-good repetition -nonfluent speech |
|
|
Transcortical Sensory Aphasia
|
-poor comprehension
-good repetition -fluent speech |
|
|
Global aphasia
|
-results from a lesion of the perisylvian area, which contains Broca's and Wernicke's areas.
-Global aphasia combines all of the symptoms of Broca's and Wernicke's aphasias |
|
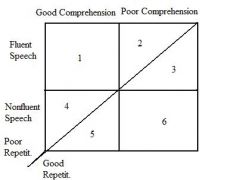
|
1-Conduction Aphasia
2-Wernicke's Aphasia 3-Transcortical Sensory Aphasia 4-Broca's Aphasia 5-Transcortical Motor Aphasia 6-Mixed Transcortical Aphasia |