![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
172 Cards in this Set
- Front
- Back
|
Basics of neonatal examination <6 weeks. |
Vitals incl temp Top to toe - well/unwell; pale; jaundiced, dysmorphia, muscle bulk/fat stores Eyes - pupil shape, sz, reaction, Posture - floppy/stiff; spontaneous movement Respiratory - auscultate, WOB, RR @ rest Cardiac - HR, HS, Cap refil, colour Physical development - Head circumference, weight, length Check mouth + Palate Abdomen Hip examination Moro reflex - dropping backwards and arms flare out and up Primitive reflexes |
|
|
Describe the position of a "Floppy"infant in the supine position. |
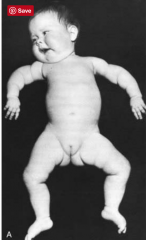
Arms externally rotated and abducted Frogs legs - externally rotated hips, flexion at knees |
|
|
Temperature of a neonate that requires referral to hospital for investigation? |
38C Requires full septic screen - urine, bld, csf |
|
|
Outline the red flags for neonates which require referral to hospital. |
Fever 38C or higher RR > 60, increased WOB, central cyanosis or apnoeas (>20 seconds) Prolonged cap refill >2 sec Tachycardia >160 - persistent New pallor or mottled skin Lethargy or poor response to stimulation - reduced activity or movement Abnormal movements or seizures Severe jaundice - onset within 48 of life, onset after 48 with serum bilirubin above treatment threshold, ANY conjugated hyperbilirubinaemia |
|
|
Describe the signs of increased WOB in Neonates/infants/children. |
Nasal flaring Intercostal/subcostal/sternal recession Expiratory grunting Abdominal breathing Accessory muscle use Forward posture |
|
|
Examination of the eye in the neonate |
Pupil - shape, size, reaction to light Red Reflex - 45cm away - both eyes simutaneously Upward Gaze (usually limited) Lateral gaze - if limited needs to be monitored and referred if not improved by 3 months ? Strabismus Corneal light reflex - for esotropia (lateral alignment of eye - use cover and uncover tests to elicit exotropia/esotropia - types of strabismus |
|
|
Describe strabismus. Types? |
Crossed eyes, is a condition in which the eyes do not properly align with each other when looking at an object. TYPES esotropia where the eyes are crossed (inward) exotropia where the eyes diverge hypertropia where they are vertically misaligned |
|
|
Indications for referral to opthalmologist for neonate/infant? |
Abnormal red reflex (abnormal colour, diminished reflex, dark spots or any asymmetric) - cataracts, retinoblastomas etc Squint --> may lead to amblyopia (loss of visual cortex) |
|
|
Describe the cardio-respiratory examination in a neonate. |
Apex beat Murmurs HS Femoral pulses RR WOB Stridor Include liver palpation with hepatomegaly being a sign of RHF |
|
|
NEONATE How to triage referral of neonate cardiac murmurs |
Isolated murmurs --> General paediatrician within a few weeks Any murmur associated with poor feeding, breathlessness or sweatiness with feeds, cyanosis, absent or diminished femoral pulses, signs of cardiac failure, failure to thrive require URGENT ASSESSMENT --> call paediatrician |
|
|
NEONATE Most commonly missed cardiac anomaly in neonates? |
Large VSD |
|
|
NEONATE Presentation of VSD in neonate ? |
Poor growth Sweating while feeding Tachycardia Overactive praecordium Pansystolic murmur Enlarge liver |
|
|
NEONATES Describe conditions that can cause stridor with or without increased WOB |
Laryngotracheomalacia Laryngeal web Haemangiomas or the larynx and trachea |
|
|
NEONATE Describe the reg flags of stridor in neonates. |
Persistent including sleeping Severe or progressive Associated with hoarse cry Apnoea Cyanotic episodes Feeding difficulty Failure to thrive Aspiration Recurrent chest infections Further evaluation --> overnight study + oximetry + nasoendoscopy |
|
|
NEONATES Name causes of tachypnoea or increased WOB. |
Acute infection ie bronchiolitis Congenital heart disease Cardiac arrhythmias ie SVT |
|
|
NEONATE Diagnosis and management of laryngotracheomalacia? |
Clinical diagnosis of intermittent stridor (worse with feeding, supine position or URTIs) Management - Reassurance but assess for red flags requiring referral to rule out other cause |
|
|
NEONATE Presentation, diagnosis and management of Laryngeal web? |
Presentation - Persistent stridor, may have respiratory distress Diagnosis - Nasoendoscopy Management - Sleep study ENT referral |
|
|
NEONATE Presentation, diagnosis and management of Haemangiomas of the larynx / trachea ? |
Presentation - Haemangiomas of the skin + worsening stridor Diagnosis - Nasoendoscopy Management - Referral to paediatrician and ENT |
|
|
NEONATE Presentation, diagnosis and management of Acute infection/bronchiolitis? |
Presentation - Coryzal symptoms, wheeze, crackles, fever, apnoea (may be the only presenting symptom) Diagnosis - Clinical, Nasal PCR swab, CXR if focal signs Management - Consider referral to hospital |
|
|
NEONATE Presentation, diagnosis and management of Congenital heart disease? |
Presentation - Poor feeding, TTF, Cyanosis, murmur, Signs of cardiac failure (including wheeze and crackles) Diagnosis - Clinical Management - Discussion with paediatrician + referral (+/- to hospital) |
|
|
NEONATE Presentation, diagnosis and management of Cardiac Arrhythmias? |
Presentation - Poor feeding, TTF, Cyanosis, Signs of cardiac failure (including wheeze and crackles) Diagnosis - Clinical Management - Discussion with paediatrician + referral (+/- to hospital) |
|
|
NEONATE Describe the examination of the abdomen, groin and genitalia in neonates. |
Abdo - organomegaly (--> abdo USS), normal for liver to be 1-2 below the costal margin Any swelling is abnormal (including hernias)--> referral to surgeon and educate about signs to present to ED - strangulated/incarcerated hernia (red/purple/painful) --> urgent hospital referral Groin - hernias Genitals - confirm urethral meatus (hypospadius - assess urine stream and refer paed surgeon/urologist) Testes |
|
|
Investigation for hepatomegaly/splenomegaly in NEONATE? |
Abdomen USS Paediatrician referral |
|
|
Which paediatric hernia usually has conservative management? |
Umbilical - They usually resolve by school age - Rarely require OT prior to age 4/5 years |
|
|
Timing for referral for undescended testes? |
Review at 6 months - if still un descended - refer to surgeon May be abdominal, inguinal canal, supra scrotal Intervention should be between 6-12 months of age OTHER - if associated with bilateral unpalpable testes or associated with hypospadius, small phallus, cleft palate ---> URGENT referral to paediatrician ? endocrine/metabolic/genetic conditions |
|
|
Indications for hip USS in neonates? Timing? |
Risk factors or Abnormal examination 4-6 weeks |
|
|
Risk factors for developmental dysplasia of the hips in NEONATES? What are the risk factors also associated with? |
Risk factors Breech Family history 1st degree or 2x second degree relative Oligohydramnios These are also risk factors for positional plagiocephaly, torticollis, foot deformities such as talipes equinovarus |
|
|
Clinical tests for development dysplasia of the hips? |
Ortaolani Barlow Reduced ROM (hip abduction) Also investigate in cases of uncertain examination such as a click rather than a clunk |
|
|
Red Flags for occult spinal bifida . |
Deep sacral dimple - >5mm, unable to visualise base Dimple >5mm diameter Dimple >2.5cm distance from anal verge Associated cutaneous findings - hair tufts, vascular lesion (haemangioma, telangectasia), subcutaneous mass or lipoma, skin appendage (skin tag), discolouration or pigmentation |
|
|
Basics of paediatric history? |
Presenting problem Past history - medial, surgical Perinatal history - pregnancy, birth, neonatal history Vaccination history Meds, allergies Family history Growth (percentiles), feeding and diet Development --> Gross/Fine motor, speech/communication, social skills Family and social function - relationships, behaviour, sleep |
|
|
What are the 4 domains of development ? |
Gross motor Fine Motor Communication and speech Social development |
|
|
What is anthropometric data? |
Centile measurements Weight Height/Length Head circumference |
|
|
When is a good time to assess development? |
Every visit but in particular immunisation visits |
|
|
Screening tool for development? |
Denver II Development Screening Test |
|
|
What is the appropriate action to take when there is a significant concern regarding development? |
Specialist referral and/or further work up |
|
|
Which of the following are True/False? 1. Neurological development if equinal-caudal and inside out. 2. Roughly a baby sits at 7-8 months. 3. Roughly a baby crawls at 1 year. |
1. False - caudo-equinal development (top down) 2. True 3. False - crawling at 9 months, standing at 1 year |
|
|
Development at 6 weeks? |
MOTOR Some head control Symmetrical movement of limbs and eyes SOCIAL/SPEECH Smiling Brief eye contact Cooing |
|
|
Development at 4 months? |
MOTOR Tracks objects through 180 degrees Lifts head, knees Hands to midline/mouth Grasp SOCIAL/SPEECH Social smiling (in response to a smile), laughing ++ Eye contact ++ Cooing |
|
|
Development at 6 months? |
MOTOR Propped up sitting (independent 7-8months) Hands to feet, hands to prop self up in front Head control when pulled up Bangs objects on surface SOCIAL/SPEECH Babbling Listens (quiets when spoken to) Enjoys interactive games Smiles when sees parents Vocal play - new sounds, raspberries |
|
|
Development at 12 months? |
MOTOR Feet take position when placed on ground Standing with support (holding on) Crawling Points Grasps with index + thumb Claps Waves goodbye SOCIAL /SPEECH +++ Conversational babble Few words - Mum/dad Separation anxiety Perseveration Looks at books / follows a point Waves |
|
|
Development at 18 months? |
MOTOR Walks well, holding hands Climbs on/off Attempts to jump Tip-tip pincer Bilateral play - hands doing different things Posting objects into containers SOCIAL/ SPEECH Follows 1 step commands Pretend play Interested in everything Pointing and following well established Understands words, increasing vocabulary at least 2 Points to body parts |
|
|
Development at 3.5-4 years? |
MOTOR Learns to ride bike Catches a ball to onto chest/hands for larger ball Throws overarm Hops Washes and dries hands Does puzzles independently SOCIAL/SPEECH Clear intelligible speech Long conversations Plays with peers Does not want to stand out amongst peers |
|
|
Age to sit without support? |
7-8 months |
|
|
Gross motor at 2yrs old? |
Walking upstairs holding on to an adult, possibly attempting alternate feet |
|
|
Motor at 6 yrs ? |
Skipping |
|
|
Motor at 3 years? |
Starting to use a tricycle |
|
|
Fine motor skills of the hand with individual digit movement develops at what age? |
9-18 months |
|
|
Age of first words? |
By 1 year usually but they will have at least developed a large receptive language base and understand many words. |
|
|
Describe the major fine motor hand milestones for different age groups. |
Whole hand 0-9 months 3-6 months - grasping, look at objects they are holding, banging objects on surface 6-9 months - banging objects together, by 9 months hand to hand transfers and purposeful release of objects Individual fingers 9-18 months Pinching (pulp-pulp), pincing (tip-tip), pointing all progressively develop. Pointing should by there by 18 months |
|
|
Asthma in children - Important steps in management? |
1. Confirm diagnosis 2. Assessing symptoms/severity 3. ? Triggers 4. Management plan 5. Discuss goals and management with parent/child 6. Written action plan, ongoing management and management of flare-ups 7. Periodic review 8. General paediatric advice - avoid smoke, eat healthy, physical activity, wt, immunisation |
|
|
Step wise treatment of asthma in children? |
First line - SABA PRN Second line - Regular preventer - ICS (low dose) or montelukast or cromone Third line - Step up regular preventer - high dose ICS or low dose ICS plus montelukast or ICS/LABA combination Following this referral should be made |
|
|
Which of the following are correct? A. 2-5 yr olds with moderate to severe persistent asthma should be trialled on a low dose ICS with review in 4 weeks. B. 2-5 Yr olds with infrequent intermittent asthma should be trialled on montelukast 4mg daily with review in 1-2 weeks C. Regular preventer use is not recommended in children 0-2 years with intermittent asthma |
A/C correct B this preventer is recommended for frequent intermittent asthma in 2-5yr olds |
|
|
TRUE/FALSE In children montelukast is generally trialled prior to ICS except in cases of severe persistent asthma. |
True |
|
|
Children with wheeze only during URTI's are considered to have which type of asthma profile? |
Infrequent intermittent asthma Thus need no preventer therapy |
|
|
What is low dose fluticasone? |
100-200mcg/day |
|
|
Age at which a child can do spirometry > |
usually > 6 yrs old |
|
|
Define asthma |
Airflow limitation - reversible with bronchodilator response - FEV1 increases by >12% (and 200ml in adults) |
|
|
Name some conditions other than asthma which may present with wheezing. |
Tracheomalacia Upper airway dysfunction Inhaled foreign body causing partial airway obstruction |
|
|
Name some conditions that are characteristed by a cough and can often be mistaken for asthma? |
Pertussis (whooping cough) CF Airway abnormalities - tracheomalacia, bronchomalacia Protracted bacterial bronchitis in young chldren Habit-cough syndrome |
|
|
Define infrequent intermittent asthma? |
Symptom free for at least 6 weeks at a time Flareups every 6 weeks of so, but no symptoms in between No preventer required |
|
|
Infrequent vs frequent intermittent asthma? |
- Intermittent - No symptoms between flare ups - Infrequent - > 6 weeks between flare ups - Frequent - < 6 weeks between flare ups (preventer recommended) |
|
|
Describe the subcategories of persistent asthma |
1. Mild - Day time 1 x /week or night time 2x /month - 2. Moderate - daytime symptoms daily, night time >1x/week, sometimes restricts activity 3. Severe - Daytime - continual, night time frequent, flare ups frequent, frequently symptoms restrict activity |
|
|
How much ventolin is delivered to the nose with a mask/spacer? |
50% Hence using a mouth piece when a child is able will give better delivery of the medication Usually 3-4 yrs old |
|
|
At what age can a child usually use a spacer with a mouth piece instead of a mask? Why do this? |
3-4 To reduce the amount of ventolin deposited in the nose |
|
|
T/F A spacer is recommended for children under 8 yrs old for pressurised metered-dose inhalers. |
False Recommended for all children |
|
|
Large volume spacers should only be used from what age? |
5 yrs |
|
|
How do you clean a spacer? |
Warm water with detergent + Do not rinse as this prevents the drug binding to the spacer |
|
|
ICS of choice for younger children? |
Fluticasone - low dose 100-200mcg Pressurised metered dose inhaler - similar to ventolin Beclomethaone and ciclesonide are not recommended < 6 yrs Budesonide comes as a dry power but <5 yr will not be able to generate enough force for the inhaler, and nebs are a more expensive option |
|
|
Benefits of ciclesonide ? Type of drug? Condition? Restrictions? |
ICS for asthma Daily dosing only for >6 yrs old |
|
|
When is the best time of year to wean asthma medications? Example |
End of winter Wean ICS dose ie. half it, if stable on this can trial step down to montelukast. |
|
|
Advise when starting an ICS preventer in a patient with asthma. |
1. Why - preventer - reduces inflammation and prevents flareups 2. Aim is to reduce symptoms and reduce need for reliever - ventolin 3. It should be used every day regardless of whether symptoms are present or not 4. Reliever - should still be used when required 5. Rinse mouth following ICS 6. Return for review in 4 weeks |
|
|
How often should you review spacer technique and the asthma action plan? |
Spacer technique - every visit Asthma action plan - 6 months |
|
|
Which is better to manage an asthma action plan? Peak flow or symptoms |
Symptoms This reduces acute care visits |
|
|
From what age can fluticasone be used? |
1 yr old |
|
|
Good way to open questing for D+A in adolscents? |
Ask about friends usage This is not enough for in depth but good opener Otherwise open ended questions |
|
|
What is CRAFFT? |
Screening questionnaire for adolescents Car, relax, alone, forget, friends, trouble Often teenagers are more open on paper than verbal questions |
|
|
Daily use and blackouts from etoh are indications for what? |
Referral to specialist Same with CRAFFT score > 2 |
|
|
Principles of treating substance abuse in adolescents ? |
Engagement Assessment of severity Psycho-education - essenetial Engagement of parents consider referral |
|
|
Aspects of motivational interviewing? |
Open ended questions Affirmation statements Reflective listening + Summarising statements |
|
|
SCARED tool? |
Screening for Child Anxiety Related Disorders |
|
|
Length of time for gender dysphoria Dx? |
6 months at least |
|
|
Features of gender dysphoria/ gender identity disorder? |
Difference between experienced/expressed and assigned gender. - Must be > 6 months - 2 or more of - a clear difference between one’s perceived gender + physical sex characteristics - an intense need to do away with their physical sex features (avert the maturity of the likelysecondary features) - an intense desire to have the physical sex features of the other gender - a deep desire to transform into the other gender - a profound need for others to identify them as the other gender - a powerful assurance of having the characteristic feelings andresponses of the other gender |
|
|
CI to testosterone therapy? |
pregnancy uncontrolled polycythaemia with a haematocrit >55% unstablecoronary artery disease possibly oestrogen responsive breastcancer |
|
|
Baseline bloods for Female to male transition? |
FBE for polycythaemia LFT for baseline prior to testosterone Fasting lipids - testosterone may increase Fasting BSL - if hx of DM Hba1c if diabetic ECG as testosterone may increase CVD risk |
|
|
Monitoring on Testosterone therapy for transitioning? |
Hormones 3 monthly 1 yr then 1-2 yrly (Testosterone aim - physiological 12-24, ostradiol <200) FBC, LFT, - 3 monthly first yr then 6 monthly (if stable) Lipids and BSL - yearly |
|
|
Perianal features of crohns |
skin tags fissures fistulae Abscess |
|
|
T/F 1. C diff is less common in patients with crohns 2. CDAI is an indicator of inflammation in crohns 3. Severe disease is indicated by a score >400 4. Remission is indicated by a score < 150 for 1 yr |
1. false - more common 2. False - indicator of disease severity 3. False > 450 4. true |
|
|
Complications of crohns? |
Stricture Obstruction Perforation Abscess bleeding |
|
|
Vaccinations to offer when starting biologic DMARDs? |
HPV HBV Influenza Strep pneumo VZV |
|
|
screening for bDMARDs? |
CI - demyelination, cardiac failure, malignancy Assess risk factors - HIV, TB, HBV, VZV, HPV CXR TB screening - IGRA, TST Hep B Pap smear / Cervical screening test |
|
|
Morning after pill? |
levonogestrel 1.5g or 2 x 750ug 12 hours apart Apparently only if < 70 kg |
|
|
Chlamydia treatment in pregnancy? |
Same Azithromycin 1g stat but need TOC ! |
|
|
T/f 1. Trichnomonas mainly occurs in men 2. Adenovirus can cause urethritis 3. PEP is available via trained GPs and PBS 4. PEP is within 72 hrs and continues for 2 weeks |
1. false - mainly females or males who have female partners 2. true - usually meatal erythema and oedema 3. False - No PBS subsidy - Public hospitals only 4. false - 4 weeks |
|
|
In MSM who present with urethral discharge treatment? |
Swabs as appropriate but treat for both chalmydia an gonorrhoea whilst awaiting results |
|
|
Which gonococcal infections require TOC? |
Pharynx Rectal Pregnant Cervical 2 weeks after treatment with NAAT |
|
|
DDX for childhood asthma? |
inhaled foreign body GORD cystic fibrosis persistent infection- pertussis or bacterial bronchitis tracheomalacia habit cough – classically absent when sleeping and treated with suggestion therapy sleep apnoea hyperventilation Travel related |
|
|
Classifications of asthma? |
no in between symptoms Intermittent frequent (>6 weekly) Intermittent infrequent (< 6 weekly) Persistent Mild - day symptoms not everyday, night symptoms not every week Moderate - daytime SS daily, night-time - weekly, restrict activity or sleep somtimes Severe - Continual daily ss, Night time - frequent, frequent flare ups, restricts activity and sleep |
|
|
T/F - asthma 1. inhaled steroids can lead to a 1cm reduction i height in the first yr 2. Avoidance of common allergens like dust improves symptom control |
1. True - no long term difference 2. false - no evidence for this |
|
|
fish oil • vitamin E supplementation • selenium supplementation • dietary sodium restriction • magnesium supplementation • vitamin C supplementation • probiotics • acupuncture • homeopathy • hypnosis • chiropractic therapy • pyridoxine (vitamin B6)1 avoidance of common allergens like dust mite• modified infant formula What do all of these things have in common with childhood asthma |
No evidence to support improvement in symptoms |
|
|
Non pharmacological methods of improving asthma? |
avoidance of cigarette smoke breast feeding is protective Weight loss if overweight or obese ?Cinelole |
|
|
crypt hyperplasia, patchy villous atrophy and intraepitheliallymphocytosis on small bowel biopsy indicates? |
Coeliac disease |
|
|
Most common nutritional deficiency in coeliac disease? Others? |
Iron deficiency Vit D B12 Folate deficiency |
|
|
investigations for coeliac disease? |
IgA-tTg tissue transglutaminase IgG-DGP - deaminated gliadin peptide Total IgA Colonoscopy if + |
|
|
Management of coeliac disease? |
Life long gluten free diet to manage symptoms and prevent complications Dietetic advice Referral to coeliac australia Treat micronutrient deficiencies Monitor growth and development Screen 1st degree relatives |
|
|
Monitoring of coeliac disease? |
review in 6 months - with bloods and height/weight - serology, FBC, Iron studies Yrly height, weight, BMI, Bloods including serology, FBC and iron studies |
|
|
complications for coeliac disease? |
MALT - lymphoma Osteoporosis Iron deficiency Poor growth Dental enamel problems infertility |
|
|
HLA associations with coeliac disease? |
HLA DQ2 + DQ8 Negative --> rules out the condition but the test has a 50% prevalence rate in the general population |
|
|
T/F Coeliac serology may be falsely negative in children under 2-4 yrs of age |
True - can take yrs for the antibodies to develop |
|
|
In the child of an affected mother with coeliac disease what is the suggested screening? |
1. bloods routine without symptoms at 4,7,12 yrs or 2. Buccal/saliva HLA status --> if negative - no further screening |
|
|
DDx for episodic abdominal pain in a child? |
constipation hirschsprungs disease Intussesception volvulus |
|
|
DDx for constipation in a child |
Usually idiopathic but rare can be caused by hypothyroidism, coeliac disease, neurological dysfunction, anteriorly placed anus |
|
|
Investigations for suspected constipation? |
None as long as normal growth velocities and otherwise well |
|
|
Vomiting in infants - DDx |
GOR (physiological)/ GORD (FTT) Pyloric stenosis (projectile) Malrotation (bilious with distension) Cows mild protein allergy (V+D, eczema, urticaria - breast or formula) Hepatitis - jaundice, pain Viral gastroenteritis - V+D+fever UTI Meningitis, hydrocephalus Metabolic - RTA, electrolytes |
|
|
What is GOR? in infants |
Physiological gastro-oesophageal reflux < 3 minutes post prandial few or no other symptoms Peak at 4 months Resolved by 12 months 70-85% of infants had regurgitation within the first 2 months |
|
|
GORD vs GOR in infants? |
GORD --> troublesome symptoms + complications (uncommon) - FTT, haematemesis, refusal to eat, aspiration pneumonia, sleeping problems, chronic resp disorders, oesophagitis, stricture, anaemia, apnoea REFER |
|
|
Methods to improve GOR in infants |
Prone positioning after feeding Thickening feeds - rice cereal, corn starch, commercial thickeners Avoid tobacco smoke Avoid over feeding Avoid aerophagia Ensure good attachment or using a bottle |
|
|
Dietary change for suspected cows mild protien allergy? |
Trial soy infant formula for 2 weeks - no dairy products Mum to have elimination diet of dairy - if symptoms recur when restarting dairy--> referral to paeds dietician |
|
|
Criteria for a specific learning disorder? |
1. > 6 months 2. significantly below expected for chronological order + impairment in everyday living 3. School age manifestation 4. Intellectual disability, visual and hearing impairment, mental and neurological disorders and psychosocial factors ruled OUT Reading, writing, perform mathematics |
|
|
Management of specific learning disabilities |
Audiometry assessment Vision assessment by opthal Special education program at school Psychoeducation assessment by an educational or developmental psyhcologist Speech therapist Occupational therapist - hand writing Paediatrician tutors |
|
|
Abdo pain in Neonates Infants/preschool |
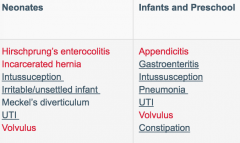
Red = acute |
|
|
Abdominal pain in School aged children Adolescents? |
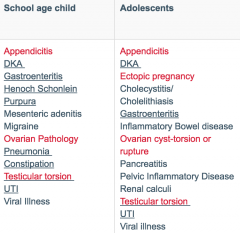
red = acute |
|
|
infant with severe bouts of episodic abdominal pain Followed by episodes of pallor and lethargy.PR bleeding or “redcurrent jelly stool” is a late sign. Dx? |
Inussusception |
|
|
investigations for heavy menstrual bleeding in adolescent? |
FBC Ferritin Coags bHCG TSH+/- T4 Pelvic US if pain or palpable mass |
|
|
History for heavy menstrual bleeding in adolescent? |
Menstrual history - menarche, LMP, frequency, duration, flow, pain Sexual history bruising or other bleeding Galactorrhoea Lethargy/HA |
|
|
Exam for heavy menstrual bleeding in adolescent> |
Pallor Androgen excess - hirsutism, acne Acanthosis nigricans Abnormal bleeding Abdomen - uterine or ovarian mass |
|
|
Management of heavy menstrual bleeding in adolescent>? |
NSAIDS - naproxen, mefenamin acid, ibuprofen Tranexamic acid 1 g 6 hrly Progresterone COCP |
|
|
History - acute eye injury? 5 |
high velocity projectiles - lawn mowers, power tools, hammering, MVA Chemical exposure Pain Foreign body, tearing or photphobia Prolonged contact lens use Visual disturbance - flashes (detachment) or floaters (intraoccular) Discharge ? First aid |
|
|
Signs of penetrating eye injuries? |
severe loss of vision or red reflex Loss of ocular mobility Asymmetrical pupil Hyphaema Distorted appearance of globe Localised conjunctival haemorrhage or chemosis |
|
|
Exam for ocular trauma - paed? |
Globe - VA, Red reflex, EOM, pupils, hyphaema VA - snellen, E chart, Picture book, Fields Lids, conjunctiva + sclera - trauma, foreign bodies, cornea, anterior chamber, iris, pupil, fundus |
|
|
Normal eye ph? |
6-8 important for chemical burns - continue irrigation until normal pH -- ie measure with urine dipstick |
|
|
Symptoms of meningococcal? |
Rapid onset Fever Leg pain Sepsis Altered LOC Neck stiffness, headache, photophobia, bulging fontanelle Petechiae / purpura - non blanching |
|
|
Causes of AOM? |
viral (25%) Streptococcus pneumoniae (35%) non-typable strains of Haemophilus (25%) Moraxella catarrhalis (15%). |
|
|
signs of AOM? |
Loss of midd ear landmarks - handle of malleus, incus and light reflex Dull, opaque, bulging TM - yellow grey Reduced TM mobility on pneumatic otoscopy urti - coryza, red pharynx, Fever, irritability, |
|
|
complications of AOM>? |
Serous otitis media / glue ear - hearing loss and developmental delay Perforation Febrile convulsions Suppurative - mastoiditis, suppurative labyrinthitis, or intracranial infection - meningitis, extra/sub-dural abscess, brain abscess Facial nerve palsy Lateral sinus thrombosis Benign intracranial HTN |
|
|
Most important avoidable factor for AOM? |
SMOKE exposure dummies also not god |
|
|
Paracetamol dose in children? |
15mg/kg x 4 /day |
|
|
Management of AOM? |
Paracetamol 15mg/kg/dose QID Topical lignocaine drops 2% AB - if <12 months, unwell, immunosuppressed or not improving within 24-48 hrs. - Amoxycillin 15mg/kg/dose TDS 5 days If no response in 48 hrs - review Dx or augmentin 22.5mg/kg/dose BD Parent information sheet No effect of decongestants, anti-histamines, corticosteroids |
|
|
Paed with acute red eye. History? 5 |
Ocular trauma contact lens wearer Time course of the redness Eye pain Itch Discharge |
|
|
5 yo with itchiness, eyelid swelling and redness, watery discharge red eye dx? |
Allergic conjunctivitis Topical antihistamines or PO + lubricants |
|
|
8 yo with Dull aching eye pain and red eye dx? |
Iritis scleritits episcleritis |
|
|
Subconjunctival haemorrhage in a child causes ? |
NAI Trauma Vigorous coughing or vomiting |
|
|
Management of corneal abrasion |
Topical chloramphenicol Review daily until healed |
|
|
Presents with an enlarged, hazy cornea, photophobia and lacrimation and red eye and pain and reduced VA |
acute glaucoma |
|
|
Mid cycle recurrent abdominal pain in 16 yo female? |
Mittelsmertz --> NSAIDS +/- gyn referral |
|
|
Acute management of seizures in a child? |
Airway + breathing + oxygen + monitor IV access BSL Benzodiazepine if > 5-10 minutes or unknown length of duration Look for cause - fever, trauma, Neuro signs Benzo - midaz IV/IO/IM/Buccal/Intranasal 0.15mg/kg (depends on site) if afebrile --> should be referred to PAEDS for follow up |
|
|
Benefits of breast feeding? |
Prevents - NEC in premies, + other GI infections resp infections Cognitive and neuro development benefits Reduced obesity Mother - weight loss, reduced OP risk, Breast ca risk and ovarian risk |
|
|
Management of low breast milk supply |
Encourage ! Assess attachment Express after feeding (more stimulation=more production) Skin to skin contact Lactation review consider galactogogues - metoclopramide 10mg TDS 5 days then taper over 5 days , domperidone 1-20mg QID - better! http://ww2.rch.org.au/emplibrary/rchcpg/Breastfeeding_Appendix4.pdf |
|
|
Advise to mothers breastfeeding and etoh intake? |
Maternal levels = breast mild levels 1 drink only and allow 2 hours before breastfeeding |
|
|
Non pharm management of mastitis/ blocked ducts? |
Warmth to breasts prior to feeding Express every few hours - when settled go back to normal feeds Massage with expressing Cold packs between sessions - fashwasher, ice pack, cold cabbage leaf NSAIDS |
|
|
Investigations for bronchiolitis? |
none routinely clinical diagnosis Can do respiratory swab |
|
|
Regarding the penis which is t/f 1. Partial foreskin attachments require intervention 2. Balanitis can be severe enough to require PO AB 3. The foreskin is non retractile in most newborns |
1. False - normal variant - usually resolves 2. true 3. true --> it separates overtime - 40% retractile at 1yr, 90% 4 yrs, 99% 15 yrs |
|
|
At what age does the Foreskin retract? |
40% at 1 year, 90% at 4 years and 99% at 15 years |
|
|
Common causes for red penis tip? |
Irritation from wet/soiled nappies inappropriate attempts at retracting the foreskin Bubble bath/Soap residue Rx - Avoid above, reassurance, barrier cream, Topical 1% hydrocortisone |
|
|
Frequency of balanitis in boys Rx? |
6% uncircumcised + 3% of circumcised males RX - Warm bath with foreskin retracted (if retractile and not too painful) - Topical hydrocortisone 1% - mild - Topical Ab sometimes used - Candida treatment if evidence of satellite lesions - Nystatin, clotrimazole, miconazole - If cellulitis - PO antibiotics |
|
|
Antibiotics for perineal infection in young boys? |
Co-trimoxazole 4/20mg/kg BD or amoxycillin 15mg/kg 8 hrly |
|
|
Management of Zipper injury in boys ? |

topical / local anaesthetic infiltration/sedation 1. Cut median bar of zipper with wire cutters (zipper falls off) 2. Cut through zipper below -Zipper can be separated from below If trapped within slider - liberal anaesthetic cream and ease slider down CHECK FOR URETHRAL INJURY |
|
|
Indicators of a true phimosis? |
Foreskin not retractile bu puberty Previously retractile becomes non retractile Obvious ring of scar tissue at opening Inability to visualise urethral meatus Ballooning of the foreskin with micturition |
|
|
Management of true phimosis |
Application of topical steroids - 0.05% betamethasone BD for 2-4 weeks Gentle retraction of foreskin without causing discomfort Apply a thick layer to the tightest part of the foreskin Higher potency can be used If not responding --> Circumcision |
|
|
Management of paraphimosis? |
Adequate analgesia / sedation Liberally cover entire foreskin and glans in topical anaesthetic cream and gladwrap for 1 hr Firmly + gently compress within 1 hand for a few minutes to try and squeeze the oedema out The glans may then be pushed back and foreskin returned to normal position If manual reduction fails--> surgical review |
|
|
Royal australian college for physicians (Paeds section) + Paeds surgeons association stance on circumcision |
Recommend against circumcision and certainly not < 6 months |
|
|
Main clinical indication for circumcision? |
Severe phimosis not responding to steroids |
|
|
Features /assessment of severe respiratory disease / conditions in paeds? |
Behaviour - irritable, lethargic Tachypnoea - increased or markedly reduced as tiring WOB signs - Marked Accessory (nasal flaring, sternomastoid contraction, forward posture) Marked Retraction - intercostal, suprasternal, costal margin, paradoxical breathing Oxygenation - spO2 < 85 % - Cyanosis HR - Significant increase or decrease BP - Increase or decrease RCH |
|
|
cause of whooping cough |
Bordetella pertussis |
|
|
Age group most at risk from pertussis? |
< 6 months Apnoea, severe pneumonia, encephalopathy |
|
|
Infective period of bordetella pertussis? |
Just prior to the cough and 21 days after unless treated |
|
|
Features of bordetella pertussis infection? |
Cough and coryza for 1 week followed by paroxysms of cough Post tussive vomiting Apnoea + cyanosis with coughing - infants >70% of household contacts infected |
|
|
How long can the PCR pertussis swab be + for? |
Usually negative after 21 days or 5-7 days of effective AB |
|
|
Management of confirmed pertussis? |
Ab if early < 14 days or complications Azithromycin if can swallow tablets Clarythromycin is unable to Allergy - bactrim |
|
|
Exclusion period for Whooping cough? |
5 days of treatment or 21 days from cough Daycare contacts - same room or household contacts < 6 months old and received < 3 pertussis immunisations --> Excluded or 14 days from first exposure or following 5 days AB |
|
|
Who gets antibiotic prophylaxis for pertussis following exposure? |
Close contact (household) during infective period < 21 days or < 5 days Ab - > 1 hour exposure <1 m AND CHILD - Age < 6 months, <3 doses immunisation, Household member < 6 months, attended day care in the same room as infant and < 6month ADULT - Expectant parents in the last month of pregnancy, Health care worker in maternity hospital or newborn nursery, child care worker caring for infants < 6 months or household member aged < 6 months ( ie adult exposed and 3 month old at home) |
|
|
Antibiotic choice for pertussis prophylaxis ? |
Same as full treatment - azithromycin Or bactrim (trimethoprim + sulfamethoxazole) |
|
|
a 3 month old goes to day care where another child in his class was confirmed positive for pertussis and was at school with him last week. How do you manage this case? |
Exclude for 14 days from exposure or 5 days of treatment + treatment with PO antibiotics - Suspension clarythromycin (Azithro no suspension) Or bactrim |