Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
137 Cards in this Set
- Front
- Back

|
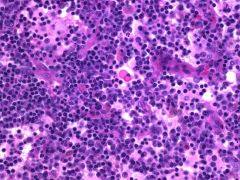
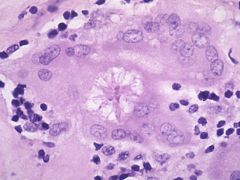
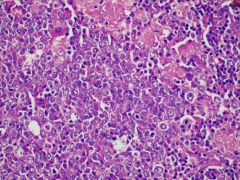
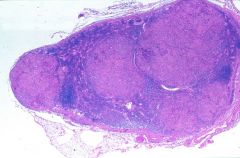
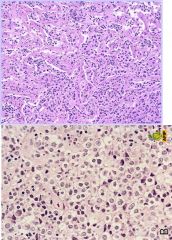
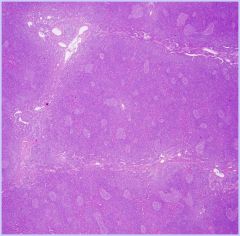
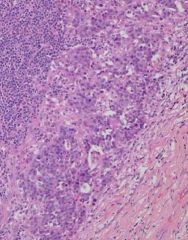
Rosai-Dorfman (Sinus histiocytosis with massive lymphadenopathy)
Unknown etiology Massive painless enlargement cervical LNs Distension of sinuses by histiocytes, lymphocytes, and plasma cells – diagnostic hallmark of the disease (pic - intersinusal tissue abundant plasma cells) |
|
|
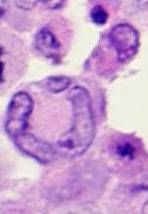
Rosai Dorfman
Many of the histiocytes have intact lymphocytes within their cytoplasm – an important diagnostic feature known as emperipolesis. Self-limiting |
|
Asian female painless cervical node
|
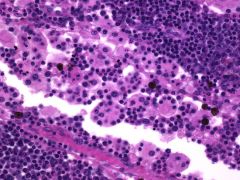
Kikuchi lymphadenopathy
Unknown etiology, self-limiting, painless young Asian females Paracortical well-circumscribed necrotizing lesions PLASMA CELLS & NEUTROPHILS ARE RARE DDx: lymphoma w necrosis |
|
|
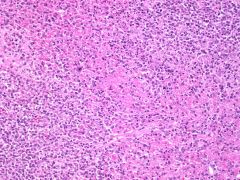
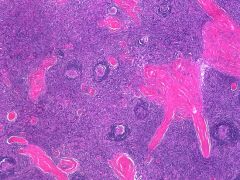
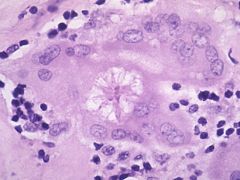
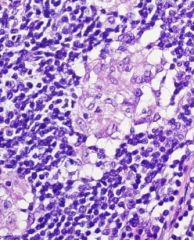
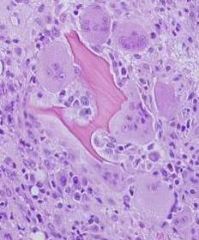
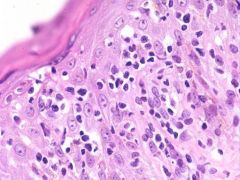
Sarcoidosis
Non-necrotizing granulomas with epithelioid histiocytes, Langhans giant cells Asteroid bodies (pic) can be seen within giant cells and are composed of aluminum, silicon, Ca, P, lipoproteins |
|
|
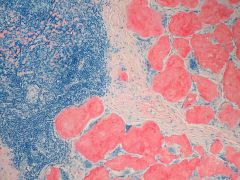
Amyloid
Congo Red |
|
|
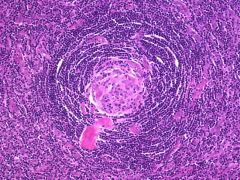
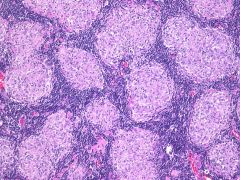
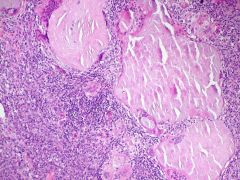
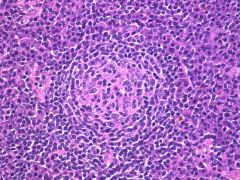
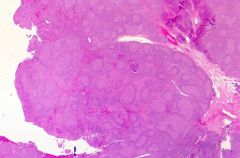
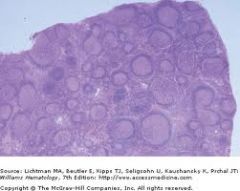
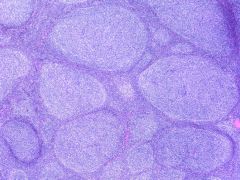
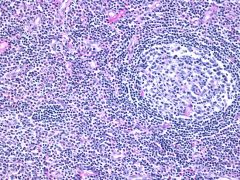
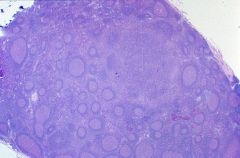
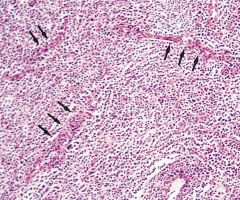
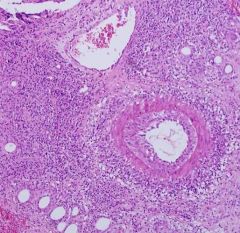
Castleman's Disease
90% of solitary lesions are hyaline-vascular type Large lymphoid follicles and sclerotic bands Abnormal germinal centers with hyalinization and vasc prolif *** Concentric layering of lymphocytes resulting in an onion-skin appearance Asymptomatic |
|
|
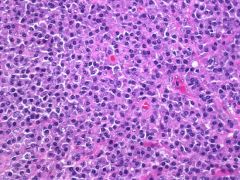
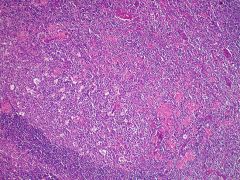
Castleman's Disease, plasma cell type
Systemic / multicentric Diffuse plasma cell proliferation interfollicular ** symptomatic & poor px: F, anemia, elevated ESR, hypergammaglobulinemia, and hypoalbuminemia |
|
19M painless axillary lymphadenopathy
|
Toxoplasmosis
Hyperplastic follicles with rx germinal centers with numerous TBMs and clusters of epithelioid histiocytes. ALSO MONOCYTOID B CELL HYPERPLASIA |
|
|
DDx for double+ CD4 & CD8
|
T cell lymphoma
PTGC (Progressively transformed germinal ctrs) Thymoma NLP-HD |
|
|
Necrotizing neutrophilic granulomas seen in?
|
- Cat scratch
- LGV - Yersinia - tularemia - fungal |
|
Marked follicular hyperplasia with giant irregular shaped follicles. Can involute and show depleted follicles with fibrosis.
|
HIV related lymphadenopathy
|
|
|
Multiple germinal centers in 1 follicle
Lollipop germinal centers with blood vessels Onion skin mantle zone |
Castleman's disease
(associated with HHV8) |
|
|
Follicular dendritic cell markers
|
CD21
CD23 CD35 D240 |
|
|
Follicular hyperplasia
Epithelioid hyperplasia Monocytoid B cells in sinuses |
marginal zone,Toxoplasma gondii
|
|
|
Paracortical proliferation immunoblasts
Sinus distension monocytoid B cells Focal necrosis and apoptosis |
Mono
Large atypical cells are CD30+! |
|
|
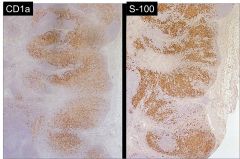
Pale paracortical expansion
Increased Langerhans and IDR cells Melanin pigment |
Dermatopathic lymphadenitis.
... LN draining a rash. Can mimic MF |
|

Large zones of necrosis
Crescentic histiocytes Karyorrhexis (No neutrophils or eos or plasma cells) Dx? DDx? |
Kikuchis
-young Asian females SLE (plasma cells) Cat scratch |
|

Suppurative granulomas
Stellate abscess NEUTROPHILS |
Bartonella henselae
(Warthin-Starry or Brown Hopps stain) |
|
Distended sinuses with foamy histiocytes
Bilateral cervical LN Teenager with fever |
Rosai-Dorfman disease
(emperipoiesis) |
|
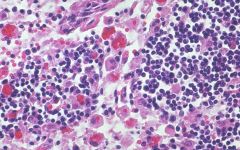
Erythrophagocytosis DDx:
|
"Hemophagocytic syndrome"
- Virus - TCL - X-linked syndrome |
|
Immunodeficient patients
Vascular nodular proliferation Plump endothelium |
Bacillary angiomatosis
(Also caused by Bartonella henselae!) (Looks nodular; looks like soft tissue tumor: DDx is Kaposi! Do warthin-starry stain) |
|
|
Dim CD20
CD5 CD23 |
CLL/SLL
|
|
|
Poor prognostic markers in CLL
|
CD38
ZAP70 trisomy 12 del(11q) del(17p) |
|
|
Bright
CD11c CD25 CD103 Annexin A1 TRAP DBA.44 |
Hairy cell leukemia
|
|
|
HCL in spleen?
Bone marrow? Peripheral blood? |
RED PULP LAKES
Fried egg & reticulin fibrosis Pancytopenia & MONOCYTOPENIA |
|
|
What is unique about treatment for HCL?
|
NO CHOP
good response to purine analog |
|
|
What do we call HCL with a an atypical feature (eg. leukocytosis
|
monos, lacking a classic marker),HCL variant.
POOR PROGNOSIS & resistant to therapy |
|
|
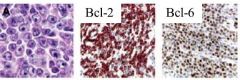
CD10
bcl2 bcl6 genetics? when is bcl2 negative? |
FISH t(14; 18)
MBC, mcr bcl2 is negative in cutaneous FL Also, as FL grade increases, bcl2 expression decreases |
|
|
CD20
CD5 CD43 bcl2 bcl1 genetics? |
Mantle cell lymphoma
(bcl1 = cyclin D1) t(11;14) |
|
|
Mantle cell lymphoma involving GI tract?
|
lymphomatous polyposis
|
|
|
Follicular colonization by marginal zone
Monocytoid cells Plasmacytoid cells DUTCHER BODIES gene? In what %? px implication? when is the classic translocation not seen? |
Marginal zone lymphoma
t(11;18) in 25-50% MALT & resistant to abx therapy! MLT and AP12 genes Not seen in DLBCL from MZL Not seen in nodal MZL |
|
|
MZL precursors
|
Hashimoto
Sjogrens HCV Lyme Disease (skin) Chlamydia (eye) Campylobacter (sm int) H pylori (gastric) |
|
|
IgM gammopathy + LPL + bone marrow involvement
|
Waldenstrom macroglobulinemia
|
|
|
Cryoglobulinemia
Hyperviscosity Dutcher bodies Dx? IHC? |
LPL
CD5- / CD10- / CD23- |
|
|
Starry sky
Bubbly cytoplasm Tingible body macrophages genetics? |
Burkitt lymphoma
t(8;14) myc/IgH t(2;8) kappa/myc t(8;22) myc/lambda |
|
|
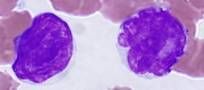
Butt cell
|
Follicular lymphoma
|
|
|
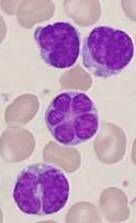
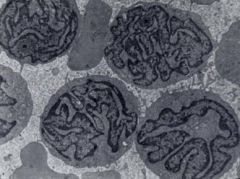
Flower cell
|
Adult T cell Leuk/Lymphoma
|
|
|
Hallmark cell
|
Anaplastic large cell lymphoma
|
|
|
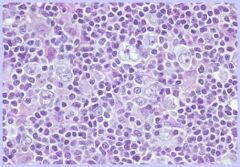
Popcorn cell
|
NLP-HL
|
|
|
CD20
CD10 bcl6 MIB1 100% bcl2 in 20% |
Burkitt
|
|
|
3 forms of Burkitt
|
1. Endemic - Africa, kids, jaw, EBV
2. Sporadic - 50% childhood lymphoma. ave 30y, GI, breast. 3. Immunosuppressed |
|
|
2 main types of DLBCL and prognosis?
|
Germinal center type (better px)
Activated B cell type |
|
|
Leg lesion old lady
Strong bcl2 bcl6 MUM1 |
Primary cutaneous DLBCL of leg
Aggressive and poor px |
|
|
<10% large B cells
CD20 +- CD30 bcl6+ |
T cell rich DLBCL
|
|
|
30F with SVC syndrome and mediastinal mass
histology? |
Mediastinal / thymic DLBCL
Lots of fibrosis lots of cytoplasm = fried egg appearance *lack surface Ig by flow. Can do PCR IgH rearr |
|
|
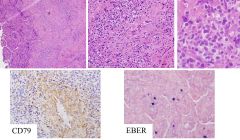
Angiocentric and angiodestructive lesion in the lung or brain
|
Lymphomatoid granulomatosis
EBV+ B cells Lots of reactive T cells CD79a around blood vessels |
|
|
CD20
CD45 EMA OCT2 BOB1 classic cell? |
NLP-HL
POPCORN CELL or L&H cell Progressive transformation of germinal centers NO EOS or NEUTROPHILS |
|
|
CD15
CD30 50% LPM1 / EBER PAX5 |
Classic HL
|
|
|
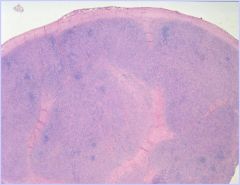
Thick capsule
Fibrous bands EOS NEUTROPHILS RS CELLS |
NS-HL
|
|
|
HL with highest level of EBV
and Least involvement of mediastinum |
Mixed cellularity HL
(interfollicular pattern, less fibrosis) |
|
|
Regressed germinal centers
No eos |
PMNs
RS in mantle zones,Lymphocyte rich HL |
|
|
LN with cells with increased cytoplasm
|
background eos and histiocytes
ITK/ SYK translocation,Peripheral Tcell lymphoma, NOS |
|
|
Lymphoepithelioid variant of TCL
|
Lennert lymphoma
(looks like large histiocytes but they are T cells) |
|
|
Rash
Hepatosplenomegaly Hypergammaglobulinemia CD23+ around vessels |
Angioimmunoblastic T cell lymphoma
Arborizing vessels Effaced architecture Polymorphous infiltrate |
|
|
CXCL1
PD1 |
AITCL
also 2/3/4/5/10 |
|
|
CD45-
EMA+ CD30+ ALK1+ cell? |
Anaplastic large cell lymphoma
Hallmark cell (kidney shape, wreath nucleus) |
|
|
t(2;5)
|
ALCL
|
|
|
Is ALK1 nuclear or cytoplasmic?
|
both!
Nuclear in ALK-NPM1 translocation t(2;5) Cytoplasmic in others |
|
|
Lytic bone lesions
Hepatosplenomegaly Skin lesions Hypercalcemia cell? |
Adult TCell Leuk/Lymphoma
Flower cell |
|
|
HTLV1+ in Japan
|
Caribbean, Africa,Adult Tcell Leuk/Lymphoma
|
|
|
TCLIA translocation
|
T prolymphocytic lymphoma
|
|
|
T cell lymphoma with main ddx of MCL & Burkitt?
|
T-lymphoblastic lymphoma
TdT+ CD5- CyclinD1- MIB<80% |
|
|
HTLV1
FOXP3 CD25 |
Adult T cell leuk/lymphoma
(also associated with lots of osteoclasts) |
|
|
Jejunal perforation
Celiac sprue px? |
Enteropathy-type TCL
|
|
|
9q34
CD5- CD8+ CD103+ 2/3/7/56+ |
Enteropathy-type TCL
|
|
|
Young men
Aggressive Hepatosplenomegaly No lymphadenopathy |
Hepatosplenic TCL
Subtle - sinusoids have T cells |
|
|
gamma-delta cells
CD4- CD8- iso7q trisomy 8 |
Hepatosplenic TCL
|
|
|
Young Asian
Large midline facial tumor Angiocentric Necrosis |
Extranodal NK-T lymphoma nasal type
|
|
|
EBV+
sCD3- cCD3e+ CD56/67+ |
Extranodal NK-T lymphoma nasal type
|
|
|
Lymphocytes surrounding fat lobules in sub q
fat necrosis karyorrhexis |
Subcutaneous panniculitis-like TCL
|
|
|
alpha-beta cells or gamma-delta in SPLTCL?
|
alpha-beta
gamma-delta in gamma-delta cutaneous TCL |
|
|
Scaly red rash becomes tumor
Epidermotropism Pautrier microabscesses CD4+ |
Mycosis fungoides
|
|
|
Cerebriform nuclei in peripheral blood & LAD
|
Sezary syndrome
|
|
|
Reactive follicular hyperplasia
|
|
Dx?
IHC? Genetics? |
Follicular lymphoma
+ CD19/20/22/79a + CD10, bcl2, bcl6 - CD5, CD43 |
|
|
What is CD43?
|
Expressed in normal and neoplastic T cells
Anomalous expression in MCL, CLL, some MZL NEGATIVE in FL (More sensitive than CD5 but less specific: 95% CLL stains CD5+ but 100% with CD43; 90% MCL CD5+, 100% CD43; MZL 10% CD5+, 50% CD43+) |
|
|
Asteroid body of sarcoid
The radiating filamentous arms contain complex lipoproteins, calcium, phosphorus, silicon, and aluminum. |
|
|
Which form of Castelmans has poor px?
What syndrome is it associated with? What virus? |
Multicentric (usually plasmacytic)
POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin abnormalities) HHV8 |
|
|
Castlemans buzzwords / clues
|
Onion skinning of mantle zone
Lollipop (germinal center w blood vessel) Multiple germinal centers in one follicle SMALL follicles (vs HIV - LARGE!) HHV8 |
|
|
Stages of HIV-related lymphadenopathy
|
Follicular hyperplasia (giant irregularly shaped) --> involution --> depletion / fibrotic
|
|
subcutaneous nodules revealed hyperplasia of germinal centers and a prominent perinodal eosinophilic infiltrate.
|
Kimura's disease
an inflammatory disorder of unknown origin endemic in the far east. |
|
|
Pattern of toxoplasmosis: follicular, paracortical, or sinus?
Mono? |
Follicular (follicular hyperplasia, epithelioid histiocytes, monocytoid B cells in sinuses)
Mono is paracortical pattern: Paracortical proliferation of immunoblasts, sinus distension of monocytoid B cells, focal necrosis / apoptosis, Large atypical cells (CD30+, EBER) |
|
|
Major DDx of infectious mono?
|
T-cell rich DLBCL
|
|
|
Markers of acute EBV?
chronic? |
IgM & IgG VCA (viral capsid antigen)
Positive heterophil ab Chronic markers: IgG EBNA, IgG VCA (EBV nuclear antigen) |
|
|
EBV associations...
|
Nasopharyngeal carcinoma
Oral hairy leukoplakia Aplastic anemia ... |
|
|
What are the atypical lymphocytes circulating in mono?
|
Reactive CD8+ T cells, responding to B-cell infection with the virus
|
|
|
Dermatopathic lymphadenopathy
Stains Langerhans cells and IDRCs |
|
|
Conditions associated with follicular pattern?
|
RLH
FL Castleman HIV Toxo RA Syphilis |
|
|
Conditions associated with a paracortical pattern?
|
EBV
Dermatopathic Kikuchi Cat Scratch Drug Lupus |
|
|
Conditions associated with a sinusoidal pattern?
|
Rosai-Dorfman
Hemophagocytic syndrome Bacillary angiomatosis LCH Whipple |
|
|
Major DDx of Kikuchi?
|
SLE (plasma cells!)
|
|

|
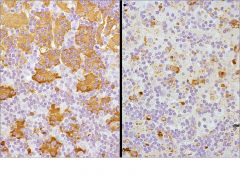
CLL
DIM CD20, 23, 11c |
|

|
HCL
BRIGHT CD20, 23, 11c |
|
|
What is bcl-1?
|
cyclin D1
|
|
Leg of an old lady
|
Primary cutaneous DLBCL
AGRESSIVE Immunoblasts - prominent nucleolus Unique IHC: bcl2+ / bcl6+ / MUM1+ / CD10- |
|
30y female with SVC syndrome
|
Mediastinal / thymic large B cell lymphoma
Lots of fibrosis Increased cytoplasm (~fried egg of HCL) **Lack surface Ig by flow - must do IgH rearr by PCR |
|
|
Large mediastinal mass think of 2 heme things?
|
Mediastinal / thymic large B cell lymphoma
Hodgkin |
|
Lung lesion
|
Lymphomatoid granulomatosis
Lung & brain Angiocentric & Angiodestructive! EBV+ Lots of rx T cells |
|
Progressive transformation of germinal centers
|
Reactive process
- Large follicles (3-4 times normal) - inward migration of perifollicular small B cells and activated T cells into the germinal centers - Absent L and H cells - May proceed, follow or accompany NLPHL Associated with NLPHL also pediatric nodal marginal zone lymphomas (boys, localized, etc) |
|
IHC of popcorn cell / LH cell?
|
(NLPHL)
CD20 CD45 EMA J chain OCT2 AND BOB1 (cHL will be neg for one of these) T cells ring around LH cell and are CD3 & 57+ -CD15, CD30 |
|
Dx?
IHC? |
Nodular sclerosis HL
Thick capsule Classic reed sternberg cells CD15/30+ CD20/45- 50% LMP1, EBER PAX5+ fascin+ |
|
|
HL with less fibrosis, no thickening of capsule, and interfollicular pattern?
|
Mixed cellularity HL
|
|
|
HL with highest frequency of EBV+?
|
MCHL, 75%
|
|
|
Hl with least involvement of mediastinum?
|
MCHL
|
|
Regressed germinal centers
Nodular growth pattern RS cells in mantle zone No eos or PMNs in background (what other disease has regressed germinal centers?) |
Lymphocyte-rich HL
(Castleman's!) |
|
|
What 3 T-cell lymphomas classically present in the lymph nodes?
|
Peripheral T-cell lymphoma, NOS
Angioimmunoblastic T-cell lymphoma Anaplastic large cell lymphoma |
|
|
What T-cell lymphomas present in the blood / bone marrow?
|
Adult T-cell leukemia/lymphoma
T pLL (prolymphocytic leuk) T LGL T LbL (lymphoblastic lymphoma) Aggressive NK-cell leukemia |
|
|
What T-cell lymphomas present in extranodal sites?
|
Enteropathy-type T cell lymphoma
Hepatosplenic T-cell lymphoma Extranodal NK/T-cell lymphoma, Nasal type Subcutaneous panniculitis-like T cell lymphoma Γδ cutaneous T cell lymphoma Mycosis fungoides Primary cutaneous CD30+ T cell LPD |
|

|
Peripheral T cell lymphoma NOS
T cells have increased clear cytoplasm Background of EOS & HISTIOCYTES |
|
|
Lennert lymphoma
(lymphoepithelial variant pTCL NOS) Looks like histiocytes but they are T cells |
|
Rash
Hepatosplenomegaly Hypergammaglobulinemia |
Angioimmunoblastic TCL
|
|
|
IHC of AITCL?
|
CD3
*****CD10***** (From TReg cells = germinal center!) EBER+ CXCL13+ PD1+ |
|
|
Hallmark cell of ALCL
|
|
Dx?
IHC? |
Sinusoidal growth pattern of ALCL
**CD45- EMA+ CD30+ |
|
|
Does ALK+ ALCL have better or worse px than ALK-?
|
Better
Usually younger patients (<30) |
|
|
Molecular of ALCL & how does IHC assist in identifying the cytogenetics?
|
t(2;5)
also t(1;2), t(2;3), inv(2)... all involve ALK gene IHC for ALK can help as the classic translocation t(2;5) is ALK-NPM, which shuttles to & from the nucleus, so there is ALK nuclear positivity in t(2;5); cytoplasmic in others |
|
|
What type of ALK+ ALCL does NOT have a good prognosis?
|
small cell variant
|
|
|
Which lymphoma is caused by HTLV1, and what patient population is classic?
|
Adult T cell leuk/lymphoma
Japan, Caribbean, African |
|
|
Lytic bone lesions
Hypercalcemia Skin lesions |
Adult TCL/L
|
|
|
Flower cell of Adult TCL/L
|
|
Which lymphoma?
|
Adult TCL/L
LYTIC BONE LESIONS LOTS OF OSTEOCLASTS! |
|
|
Classic stains for adult TCL/L
|
HTLV1
FoxP3 (usu nl in paracortical) CD25 CD4+/5+ EBV- |
|
|
Which lymphoma occurs in celiac, presents with perforated jejunum, and has a very bad px?
|
Enteropathy-associated TCL
|
|
|
What T cell marker is classically NOT expressed in enteropathy associated TCL?
|
CD5-
|
|
|
young male with hepatosplenomegaly, without lymphadenopathy. What is the aberrant T cell marker?
|
Hepatosplenic TCL
GAMMA DELTA T CELLS! Usually CD4/-8- + CD2, 3, 7, 8, 56, 103 |
|
|
Iso(7q) or tri(8)
|
Hepatosplenic TCL
|
|
|
Hepatosplenic TCL
INVOLVES SINUSOIDS of liver and spleen; SPARES WHITE PULP CLASSICALLY INVOLVES BONE MARROW TOO! |
|
Young Asian patient with large midline facial mass
|
Extranodal NK/T lymphoma nasal type
ANGIOCENTRIC NECROSIS hemophagocytosis T(CD3+) or NK (CD56); EBER+ |
|

|
Subcutaneous panniculitis-like TCL
Αβ are included in SPLTCL Γδ are called cutaneous γδ T cell lymphoma Lesions are confined to subcutis Lymphocytes encircle fat lobules Septum involvement is mild Karyorrhexis and fat necrosis almost always present |
|
CD4+
|
Mycosis fungoides
Long natural history Epidermotropism Cerebriform nuclei PAUTRIER MICROABSCESSES |
|
|
Cerebriform nuclei of MF
|
|
|
Sezary syndrome
|
Exfoliative erythroderma, generalized lymphadeopathy and malignant (Sezary) T cells in the peripheral blood
Spares bm |
|
|
ITK/SYK translocations
|
PTCL
|
|
|
TCL1A translocations
|
T-PLL
|
|
|
9q34 amplifications
|
Enteropathy associated TCL
|
|
|
Isochromosome 7q
|
Hepatosplenic TCL
|
|
|
Trisomies
|
Angioimmunoblastic TCL
|