![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
Definition of heart failure |
State in which either/or:
(1)heart is incapable of pumping a sufficient supply of blood to meet the metabolic requirements of the body
(2) requires elevated ventricular filling pressures to accomplish this goal |
|
|
Systolic Dysfunction |
EF <40% |
|
|
Cardiac Index |
CO/BSA (L/min/m2)
Normal is 2.5 - 4.0 |
|
|
Determinants of SV |
Rhthym (sinus vs afib) Preload Afterload Contractility |
|
|
Cardiac Output |
CO = HR X SV
Normal is ~ 5L/min |
|
|
Myocardial Wall Stress/Tension |
Tension directly proporotional to:
(1) Intraventricular Pressure (2) Radius |
|
|
Determinants of MAP |
MAP ~= to SVR X CO |
|
|
Poiseuille equation for blood flow |
Flow is directly related to:
(1) Change in pressure (2) radius to power of 4
Inversely related to:
(1) Vessel length (2) Blood viscosity |
|
|
Primary disease processes leading to heart failure |
CAD Cardiomyopathies Myocarditis Valvular heart disease Pericardial disease Pulmonary disease (e.g. COPD) |
|
|
High Output Heart Failure |
Supranormal cardiac output with that lead to neurhormonal activation and eventual heart failure |
|
|
Mechanism and causes of high output heart failure |
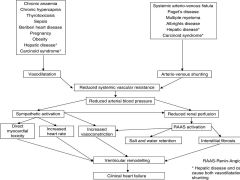
|
|
|
NYHA Classification of Heart Failure Severity |
I. Asymptomatic on ordinary physical activity |
|
|
Causes of acute exacerbations of CHF |
• Sodium and volume excess |
|
|
Overview of management for acute CHF exacerbations |
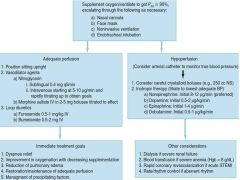
|
|
|
How does NIV help with cardiogenic pulmonary edema |
(1) Increased FRC leads to improved oxygenation and decreased WOB
(2) Reduced O2 demand and decreased adrenergic stimuli
(3) Improves V/Q matching
(4) Reduced afterload improved cardiac output
(5) Reduced preload |
|
|
AHA Stages of Heart Failure |
A: At risk of heart failure without symptoms nor structural heart disease B: Structural heart disease without symptoms of CHF D: Refractory CHF |
|
|
Summary of Canadian Cardiovascular Society Recommended Treatments for CHF |

|
|
|
Indications for cardiac resynchronization therapy
|
LVEF < 35%
LBBB NYHA class II, III, or IV Sinus rhythm QRS > 150ms |
|
|
Indications for ICD as primary prevention in heart failure
|
EF < 35% and NYHA class Ii or III
EF < 30% and NYHA class I |