![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
114 Cards in this Set
- Front
- Back
|
Bowel elimination |
passage and dispelling of stool through the intestinal tract by means of intestinal smooth muscle contraction |
|
|
Urinary elimination |
passage of urine out of the urinary tract through the urinary sphincter and urethra |
|
|
Variations of Elimination Problems |

|
|
|
What are the consequences of loss of control? |
Leads to: -Skin breakdown -Changes in daily activities -Changes in social relationships |
|
|
Who is at RISK FOR ELIMINATION PROBLEMS? |
All individuals, regardless of age, gender, or race, are potentially at risk Populations at greatest risk: -Children -Pregnant women -Older adults |
|
|
Individual Risk Factors |
-Age(children, older adults) -Pregnancy -Neurological impairment: traumatic brain injury, stroke -Altered mobility: fracture, obesity -Cognitive impairment: dementia, Alzheimer’s --Congenital defects: spina bifida, cerebral palsy -Medical conditions: renal stones, crohn’s disease |
|
|
How to assess a Problem With Voiding ? |
-Explore its duration, severity, and precipitating factors -Note the patient’s perception of the problem -Check the adequacy of the patient’s self-care behaviors |
|
|
Effects of Diuretics on Urine Production and Elimination |
prevent reabsorption of water and certain electrolytes in tubules |
|
|
Effects of Cholinergic on Urine Production and Elimination |
stimulate contraction of detrusor muscle, producing urination |
|
|
Effects of Analgesics and tranquilizers on Urine Production and Elimination |
suppress CNS, diminish effectiveness of neural reflex |
|
|
Medications Affecting Color of Urine |
Anticoagulants:red urine Diuretics:pale yellow urine Pyridium:orange to orange-red urine Elavil:green or blue-green urine Levodopa:brown or black urine |
|
|
Physical Assessment of Urinary Functioning |
-Kidneys:Palpation of the kidneys is usually performed by an advanced health care practitioner as part of a more detailed assessment. -Urinary bladder: Palpate and percuss the bladder or use a bedside scanner. -Urethral orifice: Inspect for signs of infection, discharge, or odor. -Skin:Assess for color, texture, turgor, and excretion of wastes. -Urine:Assess for color, odor, clarity, and sediment. |
|
|
Constipating Foods Affecting Bowel Elimination |
cheese, lean meat, eggs, pasta |
|
|
Elimination Developmental Considerations (Infants) |
Characteristics of stool and frequency depend on formula or breast feedings |
|
|
Elimination Developmental Considerations (Toddler) |
Physiologic maturity is the first priority for bowel training. |
|
|
Elimination Developmental Considerations (Child, adolescent, adult) |
Defecation patterns vary in quantity, frequency, and rhythmicity |
|
|
Elimination Developmental Considerations (Older Adult) |
Constipation is often a chronic problem; diarrhea and fecal incontinence may result from physiologic or lifestyle changes. |
|
|
Foods with Laxative effect Affecting Bowel Elimination |
fruits and vegetables, bran, chocolate, alcohol, coffee |
|
|
Gas producing Foods Affecting Bowel Elimination |
onions, cabbage, beans, cauliflower |
|
|
Effect of Medications on Stool |
Aspirin,anticoagulants: pink to red to black stool Iron salts: black stool Antacids:white discoloration or speckling in stool Antibiotics:green-gray |
|
|
Physical Assessment of the Abdomen |
-Inspection:observe contour, any masses, scars, or distention -Auscultation:listen for bowel sounds in all quadrants Note frequency and character, audible clicks, and flatus. Describe bowel sounds as hypoactive, hyperactive, absent or infrequent. -Percussion and palpations: performed by advanced practice professionals |
|
|
Physical Assessment of the Anus and Rectum |
-Inspection and palpation ---Lesions,ulcers, fissures (linear break on the margin of the anus), inflammation, and external hemorrhoids ----Ask the patient to bear down as though having a bowel movement. Assess for the appearance of internal hemorrhoids or fissures and fecal masses. ---Inspect perineal area for skin irritation secondary to diarrhea or fecal incontinence. |
|
|
Common Diagnostic Tests (laboratory test) |
Urinalysis, blood urea nitrogen (BUN), creatinine, culture, occult blood |
|
|
Common Diagnostic Tests (Radiographic tests and scans) |
X-rays, computed tomography (CT) scans, magnetic resonance imaging (MRI), ultrasound |
|
|
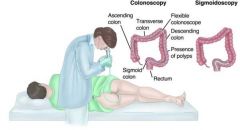
Common Diagnostic Tests (Direct observation tests) |
Colonoscopy, cystoscopy, uroscopy *Other tests: Bladder stress testing, urine flow studies |
|
|
How do you care for a patient undergoing Testing related to Elimination? |
-Patient knowledge -Psychosocial and emotional factors; fear, anxiety -Urologic/bowel function, include voiding/bowel habits/pattern -Fluid intake -Hygiene -Presence of pain or discomfort -Allergies |
|
|
What are the types of Urine Specimens? |
-Routine urinalysis -Clean-catch or midstream specimens -Sterile specimens from indwelling catheter -Urine specimen from a urinary diversion -24-hoururine specimen -Specimens from infants and children |
|
|
What to do for a Stool Collection? |
-Medical aseptic technique is imperative -Hand hygiene, before and after glove use, is essential -Wear disposable gloves -Do not contaminate outside of container with stool -Obtain stool and package, label, and transport according to agency policy |
|
|
Patient Guidelines for StoolCollection |
•Void first so that urine is not in stool sample •Defecate into the container rather than toilet bowl •Do not place toilet tissue in the bedpan or specimen container •Notify nurse when specimen is available |
|
|
What are some Primary Prevention of Elimination? |
•Hydration •Adequate dietary fiber •Regular toileting practices •Regular exercise •Avoidance of environmental contamination |
|
|
Screening for Elimination |
• Colonoscopy screening • Occult blood screening • Prostate cancer screening |
|
|
Colonoscopy |
|
|
|
Most common treatment strategies |
•The most common strategies include •Pharmacotherapy •Incontinence management •Invasive procedures and surgery * Treatment strategies depend on the underlying condition |
|
|
Pharmacotherapy for Bowel Elimination |
•Laxatives •Bulk-forming agents •Bowel stimulants •Lubricants •Saline laxatives •Stoolsofteners •Antibiotics •Antispasmodics •Analgesics |
|
|
Pharmacotherapy for Urinary Elimination |
• Antibiotics •Antispasmodics •Analgesics |
|
|
Surgical Interventions for Bowel Elimination |
• Colectomy • Colostomy or ileostomy • Rectal prolapse repair • Hemorrhoidectomy |
|
|
Surgical Interventions for Urinary Elimination |
• Prostate surgery • Bladder surgery • Urinary diversion • Surgery for renal calculi • Stents to relieve obstruction |
|
|
How to Maintain Normal Voiding Habits |
• Schedule • Urge to void • Privacy • Position • Hygiene |
|
|
Promoting Regular Bowel Habits |
• Timing • Positioning • Privacy • Nutrition • Exercise • Abdominal settings • Thigh strengthening |
|
|
Patient Outcomes for NormalBowel Elimination |
• Patient has a soft, formed bowel movement every 1 to 3 days without discomfort. •The relationship between bowel elimination and diet, fluid, and exercise is explained. •Patient should seek medical evaluation if changes in stool color or consistency persist. |
|
|
Whatare the three things that regulate and maintain bodily homeostasis? |
1. Fluid 2. Electrolyte 3. Acid-base Balance |
|
|
Wateris the __________ that accounts for ____% of total body weight and transportsand dissolves salts, nutrients, and wastes |
Water is the solvent that accounts for 60% of total body weight and transports and dissolves salts, nutrients, and wastes |
|
|
Whatare the 2 major fluid compartments? |
1. Intracellular Space 2. Extracellular Space |
|
|
Whatare the 3 types of extracellular fluid? |
1. Transcellular (1L at any given time) 2. Plasma (1/3 of ECF) 3. Interstitial (2/3 of ECF) & lymph |
|
|
How much does 1 liter of H2O weigh? |
2.2 lbs |
|
|
Whatare the normal values for Sodium? |
Sodium(Na+) 135 - 145 mEq/L
|
|
|
What are the normal values for Potassium? |
Potassium (K+) 3.5 - 5.0 mEq/L |
|
|
What are the normal values for Chloride? |
Chloride (Cl+) 98 -106 mEq/L |
|
|
What are the normal values for Calcium? |
Calcium (Ca2+) 4.4 - 5.2 mEq/L (9 - 10.5 mg/dl) |
|
|
What four mechanisms control fluid and electrolyte movement (tell if theyrequire energy)? |
1. Active transport (Energy req.) 2. Diffusion (no energy req.) 3. Facilitated transport (no energy req.) 4. Osmosis (no energy) |
|
|
What are fluids with the same osmolality as the cell interior? |
Isotonic |
|
|
Whatare solutions in which the solutes are less concentrated that thecells? |
Hypotonic |
|
|
Whatare solutions in which the solutes are more concentrated than thecells? |
Hypertonic |
|
|
What is the accumulation of fluid in the interstitium? |
Edema |
|
|
What are causes of increased venous hydrostatic pressure? |
1. Fluid Overload 2. Heart Failure 3. Liver Failure 4. Obstruction of venous return to the heart 5.Venous insufficiency |
|
|
How do you measure pitting edema? |
Measure finger depression in mm |
|
|
How should you document the severity of pitting edema? |
1. No pitting 2. Mild edema (2mm depression, disappears rapidly) 3. Moderate pitting (4mm depression, disappears in 10-15s) 4. Moderately severe pitting (6mm depression, may last more than 1 min.) 5. Severe pitting (8mm depression, can last more than 2 min.) |
|
|
What is first spacing? |
Normal distribution of fluid in the ICF and ECF |
|
|
What is second spacing? |
Abnormal accumulation of interstitial fluid (edema) |
|
|
What is third spacing? |
Accumulation of fluid in a part of the body where it is not easily exchanged. |
|
|
What are preventative measures to reduce the risk for developing fluid volume overload? |
-Strictly monitor I/Os -Monitor vital signs -Weigh daily -Assess for breath sounds -High fowlers position -Restrict sodium intake -Auscultate heart (muffled sound if overload) -Administer Diuretics -Fluid restriction -Auscultate lung sounds |
|
|
What are nursing interventions for treating fluid volume deficit? |
-Monitor changes in vital signs -Strict I/Os -Daily weights -Force fluids -Isotonic IV fluid administration (0.9 % NaCl) |
|
|
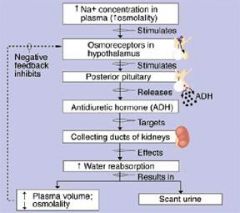
List the body mechanisms that regulate water balance |
1. Hypothalamic (stimulates thirst or ADH release) 2. Pituitary (ADH release by posterior pituitary which reabsorbs water into blood and decrease urine output. 3. Adrenal Cortical (releases glucocorticoids and mineralcorticoids) 4. Renal 5. Cardiac (hormones help excrete sodium and water) 6. Gastrointestinal (secretes 8000ml of digestive fluids that are reabsorbed; vomiting and diarrhea cause significant fluid loss) 7. Insensible water loss (invisible vaporization from lungs and skin) |
|
|
What are the differences in the pediatric population for fluid and electrolyte balance? |
1. Mouth (site for introducing infection b/c kids put everything in their mouths) 2. Esophagus (lower esophageal sphincter is not developed so children vomit after eating) 3. Stomach (stomach capacity is small) 4. Intestines (small intestine not fully mature) 5. Biliary System (liver large at birth) 6.Fluid balance and losses (body balance, insensible losses, more body fluid than adults) *GI tract doesn't mature until 2yrs old |
|
|
What are normal physiologic changes that increase susceptibility for fluid and electrolyte imbalances? |
-loss of ability to concentrate urine -Decreased renal blood flow -Hormonal changes -Loss of subcutaneous tissue -Thinning of the dermis (loss of moisture through the skin) -decreased thirst mechanism -Increased risk of free-water loss -Functional and musculoskeletal changes -Mental status changes -incontinence |
|
|
What are some causes of fluid volume deficit? |
-Major illnesses or injury -Disease -Therapeutic measures (IV fluids, diuretics NG tubes (loss of NA, K, H, Cl) -Perioperative patients (restriction of PO fluids, blood loss, gastro prep) |
|
|
What are the S&S of fluid volume deficit? |
-Thirst -Tachycardia -decreased skin turgor -hypotension -dry mucous membranes -decreased urine output -increased serum osmolaity, H/H & Na+ |
|
|
What are some causes of fluid volume overload? |
-Excessive fluid intake -Abnormal retention of fluids -shift of fluids from interstitial into plasma fluid |
|
|
Whatare S&S of fluid volume overload? |
-Bounding pulse -Crackes -Edema -Hypertension -Muffled heart sounds -Jugular vein distension -Decreased serum osmolality, H/H & Na+ |
|
|
What are abnormalities of the following lab values you would see with dehydration? |
1.H&H (more than 3x Hgb) 2.BUN > 20 3.Specific Gravity > 1.030 4.Serum Osmolality > 295 5.Serum Sodium >145 mEq/L 6.Serum Potassium > 5.0 mEq/L |
|
|
Priority Nursing Interventions for Dehydration |
1. Correct underlying cause 2. PO Fluids 3. IV Fluid (0.9% Saline) 4. I and O 5. Weights 6. Vital Signs 7. Skin color 8. Urine output (monitor) |
|
|
Prevention of Dehydration |
1. Identify pts at risk 2. Implement measures to minimize fluid loss 3. Oral re-hydration solution 4. Antidiarrheal medications 5. Anti-emetic Medications 6. Antipyretic Medications |
|
|
Nursing Management of Fluid Volume Overload |
•Strict Intake and Output •Monitor vital signs •Daily weights •Administer diuretics •Sodium restriction •Assess breath sounds (crackles) •High fowlers position if + SOB |
|
|
Normal BUN levels |
8 to 20 mg/dL |
|
|
Erythrocyte count (RBC count) Values |
M. 4.2–5.4 × 10m^6/μL F. 3.6–5.0 × 10^6/μL |
|
|
Hematocrit (Hct) Values |
M. 40 -50% F. 37-47% |
|
|
Platelet count Values |
150–400 × 103/μL |
|
|
Leukocyte count (WBC count) |
4.8–10.8 × 103/μL |
|
|
Hemoglobin (Hb) Values |
M. 14.0–16.5 g/dL F. 12.0–15.0 g/dL |
|
|
Creatinine (serum) Values |
0.6–1.2 mg/dL |
|
|
What is the first line of defense in the regulation of water? |
Thirst |
|
|
Negative Feedback Loops (make it more stable) for the regulation of water |
1. Hypothalamic/Pituitary Gland:Antidiuretic Hormone (ADH) 2.Adrenal Cortex: Aldosterone |
|
|
Process of Maintaining homestasis (picture) |
|
|
|
What is the major plasma protein in the vascular space? |
Albumin |
|
|
What is colloidal oncotic pressure? |
The pressure exerted by a colloid (plasma protein) in a solution. It is affected by the solute load. *Force that pulls fluid IN to a compartment |
|
|
Hypokalemia Assessment Findings |
- N/V/D - Paresthesias & Muscle weakness - EKGChanges & - Dysrhythmias |
|
|
Hypokalemia Causes |
-GI losses -Diuretics - Steroids |
|
|
Hyperkalemia Assessment Findings |
- N/V/D - Paresthesias & Muscle weakness - EKG Changes & - Dysrhythmias |
|
|
Hyperkalemia Causes |
-Renal Failure - Burns/Crush injuries - Over-ingestion |
|
|
Prevention and Treatment of Hypokalemia |
•Can be treated with 3 potassium salts: –Potassium Chloride*** preferred –Potassium Phosphate –Potassium Bicarbonate •PO-for prevention and treatment –16-24 mEq/day- prevention –40-100 mEq/day- treatment *PO preferred, IV reserved for ppl who cannot take PO or severe deficiency |
|
|
Uses,Dosage, and Preparations |
•Solution or solid formulas –Sustained release best tolerated by patients•Adverse effects: GI tract irritation- N/V/D, abdominal discomfort, severe intestinal injury •Take with meals or full glass of water |
|
|
IV Potassium Preparations |
•MUST BE DILUTED IN SODIUM CHLORIDE-40 MEQ/L OR LESS –EXTREMELY IRRITATING TO THE VEINS •MUST BE INFUSED SLOWLY (NO FASTER THAN 10 MEQ/HR IN ADULTS) *****NEVER GIVE IV PUSH******(Only pump) •RAPID INFUSION RESULTS IN CARDIAC ARREST |
|
|
Complications of Potassium Replacement |
•Hyperkalemia- which can prove fatal –Monitor potassium levels before and during treatment •Renal failure–Monitor renal function (BUN/Creatinine) before and during treatment–Stop infusion immediately if renal failure develops •EKG changes can be an early sign that potassium toxicity is developing |
|
|
Who should not receive potassium replacement? |
Do not give to patients with renal failure, those on potassium-sparing diuretics, or hypoaldosteronism |
|
|
Treatment of Hyperkalemia |
•Withhold potassium-containing foods•Withhold medicines that promote potassium accumulation •Combination treatment includes: –Infusion of a calcium salt –Infusion of glucose and insulin –Infusion of sodium bicarbonate •Oral or rectal administration of sodiumpolystyrene sulfonate (Kayexalate, Kionex) •Peritoneal or extracorporeal dialysis |
|
|
Hyponatremia Clinical Manisfestations |
- Nausea - Muscle cramping & twitching - Increased ICP SEIZURE |
|
|
Hyponatremia Causes |
- Vomiting - Diuretics - Excessive water intake |
|
|
Hypernatremia Clinical Manisfestations |
- S/S fluid overload - CNS disturbances |
|
|
Hypernatremia Causes |
- Salt ingestion - Inadequate water ingestion - Hypertonic tube feeds |
|
|
Treatmentof Hyponatremia |
Sodium chloride: •injection ( 0.45% or 0.9%) - over 18 to 24 hours, according to deficiencies •Oral administration: -For prevention of heat exhaustion (prostration) give 1 g with each glass of water •For treatment of heat cramps, give dose with each glass of water |
|
|
Hypocalcemia Clinical Assessment Findings |
- Tetany: Trousseau and Chvostek’s Sign -Bradycardia - Hypotension - Paresthesias (abnormal sensation, “pins and needles") - Increased gastric motility - Seizures - Confusion - Irritability |
|
|
Hypocalcemia Causes |
-Hypoparathyroidism - decrease GI absorption - Diuretics Renal Failure |
|
|
Hypercalcemia Clinical Assessment Findings |
- Sedative effect - Tachycardia - hypertension - Muscle weakness - Constipation - Absent DTR (deep tendon reflex) - Dysrhythmias |
|
|
Chvostek’s Sign (Hypocalcemia) |
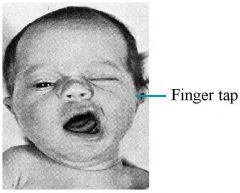
Tapping the face over the facial nerve causes spasm of the lip, nose, or face when the test result is positive. |
|
|
Hypercalcemia Causes |
- Hyperparathyroidism - Immobility - Excessive Intake |
|
|
Trousseau’s Sign (Hypocalcemia) |
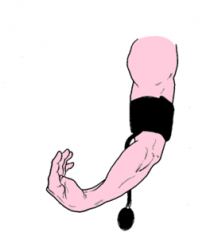
Contraction of the fingers and hands (i.e., carpopedal spasm) indicates the presence of tetany (muscle spasm) |
|
|
Treatment of Hypocalcemia |
•Calcium acetate- Oral •Calcium chloride- Injection only (IV) •Calcium gluconate- Oral or injection •Calcium phosphate- Oral –For emergency and treatment of hypocalcemic tetany use IV calcium |
|
|
Hypomagnesium Clinical Assessment Findings |
- Hyperactive deep tendon reflexes - CNS depression |
|
|
Hypomagnesium Causes |
- Alcoholism - GI losses |
|
|
Hypermagnesium Clinical Assessment Findings |
- Depressed Cardiac Impulse - Hypotension - Facial Flushing Paralysis |
|
|
Hypermagnesium Causes |
-Excessive ingestion - Renal Failure |
|
|
Prevention and Treatment of Hypomagnesemia |
•Magnesium Oxide PO (magnesium supplements, excessive doses can cause diarrhea) •Magnesium Sulfate IV or IM (treatment for severe hypomagnesemia) |
|
|
Adverse Effects of Magnesium Sulfate |
•Neuromuscular blockade •Paralysis of respiratory muscles •Can intensify effects of neuromuscular blockades (succinylcholine, atracurium) –Can be counteracted with calcium-should be at bedside •Contraindicated in patients with AV heartblock •Monitor serum mag levels |
|
|
Osmolality Normal Values |
275 - 295 mOsm/kg *describes the fluid in the body |