![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
282 Cards in this Set
- Front
- Back
|
In which patient should you use ambulatory BP monitoring or self assessment? |
- Unusual variation between readings - Suspected white coat HTN - HTN resistant to drug therapy - Suspected hypotensive episodes - ie. the elderly |
|
|
Lifestyle recommendations as per the red book for Cardiovascular disease? |
Encourage any physical activity and aim for at least 30 minutes of moderate-intensity physical activity on most, if not all, days Recommend smoking cessation Suggest a target waist measurement <94 cm for men and <80 cm for women, and a body mass index (BMI) <25 kg/m2 Recommend dietary salt restriction ≤4 g/day (65 mmol/day sodium) Encourage limiting alcohol intake to ≤2 standard drinks per day for males and ≤1 standard drink per day for females |
|
|
Aims for HTN therapy? |
≤140/90 mmHg for adults without CVD (low risk)(including those with CKD) ≤130/80 mmHg for adults with diabetes or with microalbuminuria or macroalbuminuria (urine ACR >2.5 mg/mmol for males, >3.5 mg/mmol for females) In patients at high absolute risk - some evidence - SBP <120 mmHg - when tolerated |
|
|
Diagnosis of HTN? |
BP high on 2 separate occasions - first assessment - both arms Check for orthostatic hypotension in elderly |
|
|
HTN management plan if low CVD risk? |
< 10% absolute CVD risk 1. Lifestyle advice 2. Ofter pharmacotherapy if persistently > 160/100 3. Review BP 140-159 after 2 months of lifestyle advice |
|
|
HTN management plan if moderate CVD risk? |
10-15% absolute CVD risk 1. Intensive lifestyle advise 2. Pharmacotherapy if SBP 140-159/ DBP 90-99; review if 130-139 / 85-89 in 6 months 3. Pharmacotherapy and lifestyle for BP > 160/100 or family history of premature CVD or high risk B/G |
|
|
HTN management plan if high CVD risk? |
> 15% absolute CVD risk or clinically high risk 1. Intensive lifestyle advise 2. Pharmacotherapy - simultaneous with lipid therapy - Target BP< 140/90 - without CVD - SBP< 120 in those who can tolerate and CKD - BP< 130/80 - diabetes + micro/macroalbuminaemia |
|
|
High risk backgrounds for CVS? |
South Asian, Middle Eastern, Maori, Aboriginal, Torres Strait Islander or Pacific Islander descent |
|
|
Factors that make a patient clinically high CVD risk? |
diabetes and >60 years of age diabetes with microalbuminuria moderate or severe CKD - persistent proteinuria or eGFR < 45 previous diagnosis of familial hypercholesterolemia (FH) SBP ≥180 mmHg or DBP ≥110 mmHg serum total cholesterol >7.5 mmol/L Aboriginal and Torres Strait Islander peoples aged >74 years |
|
|
All ATSI are considered to be high risk with respect to CVD. t/f |
False All over the age of 74 yrs are high risk for CVD |
|
|
First line lipid lowering drug? |
Statins - class effect |
|
|
First line antihypertensive for CVD risk ? |
ACEI, ARB, CCB, Thiazides single therapy only Not BB - less compliance and risk reduction for stroke risk |
|
|
T/f Aspirin is used as primary prevention for CVD |
False - only secondary prevention |
|
|
Frequency of BP review for low, moderate and high risk CVD - stable on therapy ? |
Low/moderate - 6 monthly High - 3 monthly |
|
|
Triple whammy? |
ACEI/ARB + diuretic + NSAID (other than low dose aspirin) ----> acute renal failure |
|
|
Medications that frequently raise BP? |
Clozapine Corticosteroids Haemopoietics - darbepoetin HRT Immunomodifiers - cyclosporin, tacrolimus MAOIs - phenelzine, leflunomide NSAIDs OCP Oral decongestants - pseudoephedrine Venlafaxine |
|
|
Up titrating antihypertensives - recommended prescribing? |
Add a second agent rather than up titrate the first agent. Ie try a combination medicine |
|
|
For the CVD risk factor calculator - after quitting smoking, how soon can they be re-categorised as "non-smoker"? |
12 months smoke free |
|
|
Features of PVD? |
Intermittent claudication - brought on with exercise + relieved by rest. Severe pain - foot to buttock Worse on leg elevation Gangrene Lower limb ulceration >4 weeks Reduced cap refill, cold, absent pulses, poor perfusion PMHx - IHD, CVA, lipids, smoking, htn, DM |
|
|
What important screening is required for PVD? |
AAA -- very common Consider the patient to have CAD!! |
|
|
Dx PVD? |
< 0.9 Hand held doppler and blood pressure cuff Arterial duplex US is only required for specialist care |
|
|
Main cause of death in PVD? |
Coronary artery disease is the cause of death in 75% of patients with peripheral arterial disease. The 5-year rate of nonfatal myocardial infarction and stroke is 20%, and of vascular death, 15%. |
|
|
Management of PVD? |
1. Graduated walking program 2. Smoking cessation 3. Statin 4. ACEI 5. Anti-platelet - aspirin 1st line Consider - Cilostazol 100mg PO BD - improves walking distance Angioplasty for severe disease - disabling or ischemia |
|
|
What is Thromboangiitis obliterans? |
Buergers disease Severe occlusive arteriopathy - atherosclerosis Heavy smoking young men ! Bipass rarely feasible Amputations are common STOP SMOKING! |
|
|
Tool to assess for risk of familial hypercholesterolaemia ? |
Dutch Lipoid Clinic Network Score 1st' relative w/ LDL>95th centile or premature vascular disease < 55M, <60 F (1) 1st' - w/ tendinous xanthomata or arcus cornealis (2) Child with LDL> 95th centile (2) Personal hx premature CAD, PVD, CVA - M <55, F<60 (2/1) Tendinous xanthomata (6) Arcus cornealis (4) LDL > 8.5 (8) LDL 6.5-8.4 (5) LDL 5-6.4 (3) LDL 4-4.9 (1) > 8 - definite 6-8 probable 3-5 Possible < 3 unlikely |
|
|
What is metabolic syndrome ? |
3 of 5 items 1. Waist circumference (f>88, m>102) - asian 80/90cm 2. Trigs > 1.7 ( or treated) 3. HDL < 1 men < 1.3 females 4. BP >130 systolic or >85 diastolic 5. Fasting BSL > 5.5 |
|
|
Key factors to address with metabolic syndrome? |
avoid smoking – normal weight (BMI 18.5–24.9 kg/m2) and normalgirth (waist circumference: <80 cm (women), <94 cm (men)) consume a Mediterranean type diet ensure low salt intake (<4 g/day) reduce alcohol consumption: ≤2 standard drinks/day (for men),≤1 standard drink/day (for women) physical activity >30 minutes every day Treat BP Treat lipids consider Aspirin |
|
|
Chest pain Dx - most likely, most serious, pitfalls, masquerades? 3 each |
Most likely - MSK, anxiety, IHD Serious - AMI, PE, Pericarditis Pitfalls - Cholelithiasis, pneumonia, shingles, GORD, oesophageal spasm Masquerades - depression, thoracic spine disease, ? |
|
|
Initial approach to STEMI in GP land? |
Call for help - nursing staff, other GP Aspirin 300mg soluble or chewable Clopidogrel 300mg IV access 14/16 G 1-2 GN - 400mcg SL 5 minutely (BP>100) Metoclopramide 10mg IV Morphine 2mg IV 5min Oxygen if sats <94% Cardiac monitoring Defib - set up and ready to go with adrenaline + Saline |
|
|
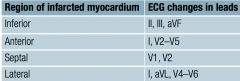
ECG leads by location in the heart? Inferior Anterior Septal Lateral? |
|
|
|
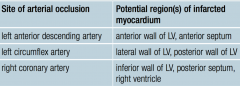
Which coronary artery to which region or myocardium? LAD L. circumflex R. coronary |
|
|
|
Features of posterior infarction? |
less common ST depression + Tall R waves in V1-V3 Can use posterior leads to Dx also |
|
|
Complications of MI? |
Cardiogenic shock, hypotension Arrhythmia - bradycardia, VT Cardiac rupture - septal, wall Acute valvular disease - ruptured chordae tendinae Death CCF Pericarditis |
|
|
indication for fibrinolysis for AMI? |
No timely access to PCI 1. duration of symptoms of AMI > 20 minutes 2. <12 hours have elapsed since onset of symptoms 3. ECG changes of either ST elevation >1 mm in two contiguouslimb leads or ST elevation >2 mm in two contiguous chest leads(or new left bundle branch block). |
|
|
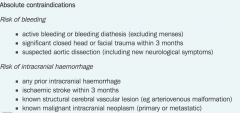
absolute CI to fibrinolysis for AMI? |
1. Bleeding risk - active bleeding or bleeding disorder, closed head or facial trauma in 3 months, suspected aortic dissection 2. ICH risk - any prior ICH, ischemic stroke within 3 months, Structural vascular lesion (AVM, aneurysm) |
|
|
Relative CI to fibrinolysis for AMI? |
1. Bleeding risk - anticoagulants, non-compressible puncture, major surgery within 3 weeks, internal bleeding (GIT, urinary) 4/52, active peptic ulcer, CPR if traumatic or > 10 minutes 2. ICH risk - severe or poorly controlled HTN, BP>180/110, Ischaemic stroke >3 months, intracranial abnormalities that are not absolute, dementia 3. Pregnancy |
|
|
Basic post ami meds? |
Aspirin + clopidogrel (even if no PCI) ACEI - ramipril Statin - atorvastatin (maximal) BB - metoprolol PRN nitrates Cardiac rehab! |
|
|
Consideration of PPIs in CAD? |
PPI impair conversion of clopidogrel into active form Hence H1 blockers might be a better option |
|
|
Main DDx for patient with erectile dysfunction 6 months post ami? |
Anti hypertensive effect Depression Progression of vascular disease/atherosclerosis |
|
|
DXx for 78 yo with CAD, COPD who presents with ongoing SOB? |
AMI, progression of CAD CCF Exacerbation or general worsening of COPD Paroxysmal arrhythmia Anaemia Renal failure Carcinoma of the lung (ex smoker) Recurrent PE Medication ADR |
|
|
78 yo with CAD, COPD who presents with ongoing SOB. Investigations As per check 2012 |
FBE - anaemia EUC - renal failure or electrolytes D dimer - PE exclusion ECG - ami, arrhythmia, LVH Spirometry - lung function ECHO - valvular or CCF |
|
|
What is the effect of omega 3 fatty acids on lipid levels? |
reduces trigs increased HDL |
|
|
Benefit of garlic in CAD? |
About 1 clove of garlic daily may have benefits in lowering bloodpressure (by up to 5%) and lowering cholesterol (by up to 9%).However, there is no evidence for efficacy in improving cardiovascularoutcomes |
|
|
important findings for assessment of hereditary hypercholesterolaemia? 2 |
Tendon xanthomata = hereditary condition Arcus cornealis also high risk Xanthalasma palpebrarum is much more common! |
|
|
Inheritance of familial hypercholesterolaemia? |
AD - ie 50% inheritance 25 x increased risk of atherosclerosis |
|
|
LDL level suspicious for familial hypercholesterolaemia? |
> 5 Use the Dutch tool - using family history, PMHx, LDL, clinical findings |
|
|
Important things to r/o when diagnosing familial hypercholesterolaemia? |
Nephrotic syndrome Diabetes Hypothyroidism Corticosteroid use These all contribute to hypercholesterolaemia |
|
|
Management priorities for familial hypercholesterolaemia? |
1. treatment for patient 2. Referral to specialist (cardiologist or endocrine) for care and genetic testing 3. Cascade genetic testing for first degree relatives |
|
|
Target LDL for familial hypercholesterolaemia? |
< 2.5 with no CVD < 1.8 with CVD |
|
|
Exam for new HTN? |
UA Carotid bruit Fundi for hypertensive changes Peripheral vascular exam ECG - LVH Abdomen - AAA, renal bruit, ballot kidneys for PCKD |
|
|
Bloods for new HTN ? |
fasting cholesterol and lipids BSL EUC UACR 24 hr BP monitoring or home monitoring |
|
|
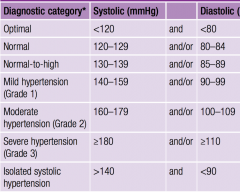
BP categories for classifying HTN? Normal Mild Moderate Severe |
|
|
|
Patients with automatic high risk CVD ? 6 |
diabetes and aged >60 years diabetes with microalbuminuria UACR >2.5 males, >3.5 females) moderate or severe CKD (persistent proteinuria or eGFR <45) patients with familial hypercholesterolaemia SBP ≥180 mmHg or DBP ≥110mmHg serum total cholesterol >7.5 mmol/L. |
|
|
Diet advice for htn? |
Salt - low Reduced saturated fat intake Reduced liquorice Increased oily fish and dietary fibre |
|
|
CVD risk 8% HTN persistent;y 155/94 ? Rx? |
None indicated Low risk < 10% then Intervention only indicated at > 160/100 But patient centered care! Once on BP meds - consider statin if cholesterol > 5.5 or HDL <0.9 |
|
|
Not meeting target with 1 antihypertensive - how best to improve control? |
Add a second agent - synergistic and reduced ADRs |
|
|
A patient with no family history, no personal history of lipids or CAD. Normal HDL 1.2, no diabetes. normal Trigs. No HTN. Not ATSI How high does cholesterol need to be to qualify for PBS lipid lowering therapy ? |
> 7.5 if Male 35-75 or female post menopause -75 otherwise > 9 ! |
|
|
Features of an innocent murmur in a child? |
Soft, < 2/6 intensity, systole, ejection BAD - harsh, pan systolic, diastolic, continuous, increase with valsalva, clicks, 4th HS Assess peripheral pulses for coarctation and hepatomegaly |
|
|
Most common congenital heart defect? |
VSD 1/3 then ASD, Patent ductus arteriosus, pulmonary stenosis Check 2016 |
|
|
Fetal alcohol syndrome cardiac defects? |
VSD ADS |
|
|
Trisomy 21 cardiac defects? |
Atrioventicular septal defects (endocardial cushion) - AVSD ASD VSD |
|
|
Turner syndrome cardiac defects? |
Coarctation of the aorta, bicuspid aortic valve |
|
|
Marfan syndrome cardiac defects?? |
Mitral valve prolapse |
|
|
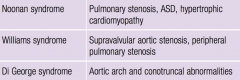
Noonan, Williams, Di George syndrome cardiac defects? |
|
|
|
Cyanotic cardiac defects?? |
Tetralogy of fallot Truncus arteriorsis Transposition of the great arteries Total anomalous pulmonary venous drainage Hypoplastic left heart syndrome |
|
|
Management of CCF? |
diuretics - frusemide 40mg / titrate Fluid restriction 1.5L /day Salt avoidance Avoid alcohol + smoking ACEI - titrate to tolerated dose BB Spironolactone if ongoing fluid overload Daily weights - review if 2kg increase over 48 hrs Education about symptoms of fluid overload and the importance of medication compliance Cardiologist management - Cardiac rehab - short low to moderate aerobic exercise ICD - EF< 35% or cardiac arrest CRT - cardiac resynchronisation therapy - QRS>150 Avoid - NSAIDS, CCB, TCAs, Steroids |
|
|
NY heart association grades of symptoms of CCF? |
|
|
|
Which of the following ABI results supports a diagnosis of PAD?A. 0.98B. 0.96C. 0.94 D. 0.88 |
D |
|
|
139/98 mmHg - persistent How would you grade this HTN? |
Mild (normal systolic but high diastolic) |
|
|
Modifiable cardiovascular risk factors? |
Smoking BP dyspilidaemia DM central obesity Poor nutrition Sedentary lifestyle Excess EtOH |
|
|
Non modifiable CVD risk factors? |
Age Sex Family history of premature CVD Ethnicity - ATSI, south asian, maori, pacific islander, middle eastern Lower socio-economic status |
|
|
Who to calculate absolute CVD risk on ? |
ASTI > 35 everyone > 45 Except if already high risk due to other factors (DM+>65, DM+microalbuminuria, moderate CKD, familial lipid, BP>180/110, Cholesterol >7.5, ASTI>75, established CVD) |
|
|
Risk factors used in the absolute CVD risk calculator? |
lipids SBP Age sex LVH on ECG DM Smoking status |
|
|
in diabetics with high CVD risk, patients should be given both a Statin and ACEI even if the BP is normal . t/f |
True Approach to total cardiovascular risk |
|
|
therapy for patients with high > 15% absolute risk should be started on therapy immediately without having to wait for a 3-6 month behaviour modification period T./f |
TRUE Where as moderate risk 10-15% should be given 3-6 months to trial some changes |
|
|
When to start antihypertensives? |
Persistently > 160/100 following lifestyle changes 3-6 months High absolute CVD risk Existing CVD |
|
|
Management of those with high absolute CVD risk ? |
Frequent + sustained advice -> diet and physical activity Smoking cessation Simultaneous BP lowering and lipid modifying therapy Aspirin is NOT routine for primary prevention |
|
|
Overall lifestyle changes for CVD? |
Stop smoking tobacco Balanced diet with low saturated fat and refined carbohydrates Minimising EtOH Regular physical activity 30min/day Maintaining appropriate body weight |
|
|
What are the 5 A's |
Ask - identify those at risk Assess - assess RF and readiness to change Advise - Provide information - behaviour prescription, brief advice, Motivational interviewing Assist - drug therapy, support self monitoring Arrange - Specialist services, support groups, counselling, follow up review |
|
|
Benefits of reducing etoh intake? |
reduction in central adiposity Reduced BP Improve trigs Improved OSA Guidelines now do NOT advise patients to have any EtOH due to risk of misuse |
|
|
Recommended CVD - exercise ? |
The Heart Foundation recommends at least 30 minutes of moderate-intensity physical activity (eg brisk walking) on most, if not all, days of the week (ie 150 minutes per week minimum) Even in bursts of 10 minutes |
|
|
T/F > 50% of deaths in people with DM are due to CVD. |
TRUE! eTG |
|
|
Risk factor for hypoglyaemia? |
Insulin or sulphonylurea use Older Longer duration of DM Renal impairment Lower BMI Cognitive impairment Hepatic impairment |
|
|
Conditions linked to obesity? |
STRONG - RR>3 T2DM, gall bladder, HTN, Lipids, OSA RR 2-3 - CAD, Stroke, OA, Gout RR 1-2 Cancer - endometrial, colon, prostate, breast Sexual dysfunction, infertility, PCOS, urinary incontinence, low back pain, GORD, depression + anxiety |
|
|
Normal waist circumference? Factors to take into consideration? |
Male <94 Women < 80 ATSI should be lower Pacific islander higher cut offs Asian < 90 men |
|
|
Classes of obesity? |
Overweight 25-29.9 Obese - 30 or more Class 1 - 30-34.9 Class 2 - 35-39.9 Class 3 - 40 or more Lower cut offs for asian and ATSI Higher for Islander |
|
|
Effect of weight loss on health outcomes. - Mortality - hospitalisations - depression - incidence of CVD |
NO demonstrated benefit eTG |
|
|
Average weight gain over 5 yrs post quitting smoking> |
3kg |
|
|
Benefits of orlistat? |
reduced hba1c Reduced LDL, trips Reduced waist circumference Reduced BP Weight loss 3 kg at 12 months more than placebo |
|
|
SE of Orlistat? |
steatorrhoea, faecal incontinence, frequent or urgent bowel movements Minimised by avoiding high fat foods Taken with each meal Prevents fat absorption Consider supplementing fat soluble vitamins in long term use |
|
|
Reason for short term use of phentermine (duromine) |
< 12 weeks Due to development of tolerance, drug becomes ineffective and risk of dependence and abuse increases Major CVD effects |
|
|
BP level where mortality starts increasing? |
> 115 systolic |
|
|
Best method to assess BP? |
BP- automated device - patient - seated and resting alone in a quiet room for at least 5 minutes. 1st reading is disregarded + an average of the 2nd and 3rd readings is calculated Otherwise - 24 hour monitor or home readings |
|
|
When calculating absolute CVD risk do you use clinic or home BP readings? |
Clinic! Home readings underestimate risk |
|
|
When to start antihypertensives? |
Low CVD risk + SBP>160/DBP>110 persistent Moderate risk + SBP>140/DBP>90 persistent High risk - immediate even if normal BP |
|
|
BP targets? |
Uncomplicated HTN < 140/90 High risk populations < 120 systolic (balancing harms) |
|
|
First line antihypertensives in uncomplicated HTN? |
ACEI, ARB, CCB, Thiazides |
|
|
First line HTN med with CKD+ proteinuria? |
ACEI or ARB first line Treat if >140/90 persistent Target < 140/90 - but < 120 may have benefit |
|
|
First line HTN med in those with prior AMI? |
ACEI or BB Same with CCF |
|
|
T/f Sympathetic denervation of the renal artery is not currently recommended for clinical management of resistant HTN |
true |
|
|
What is a hypertensive emergency? |
BP > 220/140 AND acute target organ damage or dysfunction - heart failures, APO, AMI, Aneurysm, ACK, Neuro, hypertensive encephalopathy, papilloedema, cerebral infarction, haemorrhagic stroke |
|
|
What is hypertensive urgencies? |
BP > 180/110 Not immediately life threatening but associated Headache or moderate target organ damage R x- PO drugs and review 24-72 hrs |
|
|
Diagnosis of HTN is the same for all methods of dx (home, 24 hr, clinic etc). T.f |
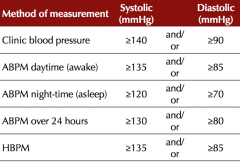
False Heart foundation - HTN management guideline 2016 |
|
|
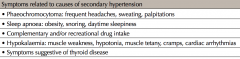
Questions to ask screening for secondary causes for hypertension? |
|
|
|
OTC meds that increase BP? |
Herbal - bitter orange, ginseng, guarana Caffiene pills + caffiene containing tea Natural liquorice St johns wort - reduced efficacy of meds Energy drinks |
|
|
Meds/drugs that worsen HTN? 10 |
NSAIDS Sympathomimetics (decongestants, diet pills, cocaine) Stimulants - amphetamines, modafinil, EtOH excess Oestrogen, HRT Corticosteroids SNRI, MAOI EPO - darbepoetin Rebound - withdrawal of clonidine, or bromocriptine Bupropion |
|
|
Physical exam for HTN |
Pulse - rate, rhythm, character JVP Cardiac - enlargement, Failure - basal creps, peripheral oedema, pulsatile liver Polycystic kidneys Fundi - rentinal haemorrhages Endocrine - cushing or thyroid Waist circ/ BMI UA |
|
|
Investigations for new HTN? |
Urine ACR BSL - fasting Fasting lipid profile EUD Hb ECG - LVH, AF, previous ischemia 2016 heart foundation guideline |
|
|
Investigations to consider for secondary causes |
Renal US or duplex ABI Plasma aldosterone/renin ratio - primary aldosteronism (Hypo-K) Urinary metanephrines and normetanephrine 24 hr - phaemo |
|
|
Salt restriction in HTN? |
Primary < 6 g / day Secondary < 4 g / day |
|
|
EtOH guidelines? |
no more than 2 / day No more than 4 on any one occasion |
|
|
% of patients achieving BP targets with 1 drug? |
30-50% |
|
|
Which is superior ACEI + CCB or ACI or thiazide? |
ACEI + CCB |
|
|
When to start BP meds >? |

|
|
|
Step wise approach to meds in HTN> |
1 at low to moderate dose - review 3 months - if not at target - add second agent - Review in 3 months - if not to target up titrate dose |
|
|
Problem with diltiazen + metoprolol? |
Increased risk of heart block but less than verapamil |
|
|
Contraindications to ACEI or ARB? |
Pregnanct Angioedema Hyperkalaemia Bilateral renal artery stenosis |
|
|
Dihydropyridine CCB? |
D for DISTAL Amlodipine, lercardipine, nifedipine, felodipine etc |
|
|
Common SE of ACEI Example with dose? |
Cough Hyperkalaemia Renal impairment Angioedema Ramipril 2.5-10mg daily |
|
|
Common SE of ARB> Example with dose? |
Hyperkalaemia Renal impairment Angioedema and cough are rare Candesartan 8-32mg daily PO |
|
|
Common SE of Peripheral CCB (distal/dihydropyridine) Example with dose? |
Peripheral vasodilation - peripheral oedema, flushing, headache, dizziness Postural hypotension Tachycardia Palpitations chest pain Gingival hyperplasia Amlodipine 2.5mg-10mg PO daily |
|
|
Common SE of Non-dihydropyridine CCB? Example with dose? |
Bradycardia Constipation - esp verpamil AV block heart failure Diltiazem CR - 180-360 PO OD Verapamil 80-160mg BD or TDS PO |
|
|
Preferred Thiazide like diuretic? |
Chlorthalidone - has better evidence for CVD benefit Dose 12.5 - 25mg OD PO (can start alternate days 12.5mg) |
|
|
Common SE of thiazides? |
Hyperuricaemia Hyperglycaemia Hypercalcaemia Hypokalaemia Hyponatraemia Postural hypotension, dizziness |
|
|
SE of BBs Example with dose? |
Bradycardia Postural hypotension Worsening heart failure Bronchospasm Cold extremities Metoprolol 25mg 25-100mg PO OD or BD Nebivolol 5mg PO daily |
|
|
Monitoring of patients with HTN when starting treatment? |
Review at 4-6 week intervals to assess adherence, ADRs, tolerability, efficacy. (if very high BP - review sooner) EUC --> measure at baseline + 2 weeks after commencing therapy in patients high risk for changes in kidney function Once stable review 3-6 monthly - with annual assessment of CVD risk factors |
|
|
T/F ACEI and ARBs can be safely prescribed at any stage of CKD. |
TRUE (eTG) Bear in mind - risk of hyper-K, Pt with RAS, CKD may need close monitoring of EUCs, NSAIDS/Diuretic combo, ACEI usually renally excreted, ARB hepatically excreted, ACEI interfer with EPO |
|
|
At what eGFR are thiazides not longer effective? |
eGFR < 50 |
|
|
first line agent for hypertensive emergencies? |
sodium nitroprusside - SNP -- ICU reduced by no more than 25% in first 2 hrs LESS urgent - amlodipine 5-10mg or felodipine 2.5-10mg or GTN topical or nifedipine |
|
|
Which anithypertensives have withdrawal syndromes? |
Clonidine - Reflex hypertension - due to catecholamine release BB - Worsens angina AIM gradual reduction Ie metoprolol can stop from 25mg BD |
|
|
Most Important question to ask in a patient with ? resistant HTN already on 2 agents with poor control? |
Medication compliance - rule this out first ! |
|
|
Conditions to consider for ? secondary htn? |
Conns - primary hyperaldosteronism Renal artery stenosis Renal disease - GN, PCKD Non compliance of medications Phaeochromocytoma Medications - etoh, excessive salt, liquorice, PO decongestants, NSAIDS, Corticosteroids, COCP, Cyclospirin, SSRI, SNRI, some CAMs, cocaine, amphetamines |
|
|
Indicators of renal artery stenosis? |
HTN that responds very well to ACEI or ARB - very renin dependent Worsening Renal function with ACEI/ARB Renal bruit Young females, older atherosclerotic patients (PVD, DM) |
|
|
Trig levels > 10 = risk for? |
Pancreatitis |
|
|
Time for Lipid lowering meds to take effect? |
2-3 weeks Stable by 1-3 months |
|
|
Lifestyle recommendations for lipids? |
physical activity and aim for at least 30 minutes of moderate-intensity physical activity on most, if not all, days smoking cessation target waist measurement <94 cm for men and <80 cm for women, and a body mass index (BMI) <25 kg/m2 salt restriction ≤4 g/day (65 mmol/day sodium) limiting alcohol intake to ≤2 standard drinks per day for males and ≤1 standard drink per day for females RACGP Redbook eTG - reduce saturated and trans fats, increase soluble fibre, introduce plant sterols |
|
|
Lipid targets for primary prevention? |
Total cholesterol < 4.0 HDL>1.0 LDL <2.0 non-HL <2.5 TG < 2.0 RACGP Redbook |
|
|
Frequency of lipid screening in low absolute cardiovascular risk? Moderate High |
Low - 5 yrly -- Lifestyle advice Moderate (10-15%) - 2 yrly - intensive lifestyle advice, consider pharmacotherapy if not reaching target after 6 months or family hx or ATSI/maori High - 12 monthly - intensive lifestyle, commence therapy at the same time as lifestyle and anti-hypertensives |
|
|
When to start screening lipids in adults? |
5 yrly from 45 yrs Mainly to calculate absolute CVD risk ATSI 2nd yrly from 35 |
|
|
First line med for high LDL? |
Statins |
|
|
When to titrate statins? |
4-8 weeks to achieve lipid levels If not meeting target with maximum tolerated dose --> add additional therapy - ezetimibe, bile acid binding resins, nicotinine acid and fibrates |
|
|
t/f Ezetimibe in addition to a statin produces very limited benefit in lowering cholesterol. |
FALSE Synergistic 20-25% reduction 10mg daily PO |
|
|
3 problems with bile acid binding resins? IE cholestyramine |
Can increase triglycerides GIT side effects Interfere with absorption of other drugs - anticoagulants, thyroxine, cyclosporin, digoxin |
|
|
2 main SE of nicotinic acid? |
Flushing Gastric irritation |
|
|
Problem with gemfibrozil? |
Significant increase in myositis when given with a statin |
|
|
Dose of a commonly used fibrate? indication? |
Fenofibrate - 145mg daily PO - renally adjusted can be added for LDL but lower down the line 1st line for hypertriglyceridaemia (Also gemfibrozil 600mg PO BD or Fish oil 1.2-3.6g of omega 3 PO daily) |
|
|
Management of hypertriglyceridaemia? |
1. Fenofibrate 145mg PO daily 1. Gemfibrozil 600mg PO BD 1. Fishoil 1.2-3.6g omega 3 PO Daily If not effective add the other + nicotinic acid |
|
|
First line for mixed hyperlipidaemia - trigs and LDL ? |
Statins If high risk both statin + fishoil or fibrate + ezetimibe CAUTION with statin + fibrate |
|
|
Dose of statin |
Atorvastatin 10-80mg PO daily Rosuvastatin 5-40mg PO daily |
|
|
Testing following starting Statin? |
Check lipids at 1-2 months + LFT + CK at this time also BSL too! For fibrates - check EUC for Cr |
|
|
What to do if CK high and asymptomatic in a patient on statin? |
Repeat following 7 days with no exercise If < 5 x ULN - continue |
|
|
When to stop a statin? |
previously normal ALT --> persistently > 3x ULN CK > 10x ULN CK > 5 x ULN and muscle symptoms Unexplained muscle pain Unexplained muscle weakness Monitor - if normalisation and symptoms mild - can restart - if recurs trial different statin or alternative lipid lowering therapy |
|
|
Score to use for patients with features of familial hypercholesterolaemia? Features? |
Dutch Lipid Clinic Network Score Very high LDL, personal or F. Hx or tendon xanthomata or strong family history of premature CVD |
|
|
Cause of secondary high LDL, Trigs |
LDL - hypothyroid, nephrotic syndrome, Cholestasis, Anorexia nervosa Trig - T2DM, Obesity, Renal, Smoking, Drugs, etoh, oestrogen |
|
|
initial therapy in acute chest pain with suspected myocardial ischaemia? |
1. Aspirin 300mg PO chewed or dissolved before swallowing 2. GTN 400mcg SL spray or 600mg mcg tablet - repeat five minutely 3 doses (SBP>100, and not inferior) 3. Persistent pain - morphine 2.5-5mg IV and titrate 5-10minutely - monitor sedation score - IV line - ECG - if certain STEMI - clopidogrel 300-600mg PO or prasugrel or ticagrelor eTG |
|
|
Time to balloon for PCI Time to fibrinolysis if unable to access PCI? |
Balloon - depends on presenting time 1st hr (of chest pain) - 60min 1-3 hrs - 90min 3-12 hrs - 90-120min Fibrinolysis - 30minutes |
|
|
Absolute CI to fibrinolysis for AMI |
|
|
|
Subsequent pharmacological management of STEMI following reperfusion? |
Aspirin 75-150mg PO daily - indefinite Clopidogrel 75mg PO daily - dual for 12 months BB - Metoprolol 25-100mg PO BD (max tolerated dose - SBP>95, HR>55) - indefinite ACEI - Ramipril (start 1.25mg - target 5-10mg daily)to target (prior ami, DM, HTN, anterior, HR>80, LV failure) - monitor Cr, electrolytes Statin - Indefinite - max tolerated consider Aldosterone anatagonist - severe heart failure - eplerenone Anticoagulation - LV thrombus |
|
|
Secondary prevention of cardiovascular events? |
Lifestyle - Smoking cessation, exercise therapy, mediterranean diet, cardiac rehab Pharm -SAAB - Statin (max), Aspirin 100-150mg PO daily, ACEI, BB |
|
|
Treatment of angina episodes? |
GTN - spray (400mcg) or Tablet 600mcg sublingual - repeat 5 min - max 3 |
|
|
Prevention of angina symptoms |
BB - atenolol or metoprolol Non-dihydropyridine CCB - diltiazem or verapamil Nitrates - GTN patch or isosorbide mononitrate SR PRN GTN prior to exertion Additional dihydropyridine CCB to BB or ivabradine |
|
|
Most common time for late coronary stent thrombosis |
Non cardiac surgery when antiplatelets have been stopped! Usually within 12 months of stent placement |
|
|
antiplatelet recommendations as per eTG for cardiac stents? |
Dual antiplatelet therapy (aspirin and clopidogrel, prasugrel or ticagrelor) is recommended for 6 weeks after deployment of a bare metal stent and at least 6 months, but probably no longer than 12 months, after a drug-eluting stent Cardiology review is always recommended prior to non-cardiac surgery in patients with stents! |
|
|
signs and symptoms of pericarditis? |
Symptoms - Fever, malaise, chest pain, Pain - sharp, retrosternal, left sided, eased by leaning forward, worse supine Signs - friction rub, tachycardia, Paradoxical pulse (SBP< 10mmHg with inspiration) Evidence of underlying cause - AMI, autoimmune, neoplasia, infection, uraemia |
|
|
First investigation following Dx of pericarditits? |
ECHO - to assess for pericardial effusion and signs of tamponade Refer to ED for urgent access |
|
|
Management of likely viral pericarditis? |
1. NSAIDS 2. Colchicine 0.5mg BD or OD for 3 months in acute or 6 months in recurrent |
|
|
main stay of heart failure treatment with impaired LV? Pharm |
ACEI BB Spironolactone +/- frusemide for exacerbations CRT - cardiac resynchronisation therapy AICD Transplant Non pharm - salt <2g, < 2L, (1.5 if overloaded), morning weights, Cardiac rehab and exercise program, stop smoking, limit EtOH/caffeine, dietitian - salt, K etc Vaccination - influenza, pneumococcal |
|
|
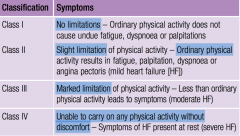
Classes of heart failure ? |
New york heart association 1. no limitation - ordinary activity - no symptoms 2. Slight limitation - ordinary activity - fatigue, dysnoea, angina or palpiations 3. Marked limitation - symptoms at less than ordinary activity 4. Severe limitation - symptoms at rest |
|
|
Initial investigations for heart failure? 4 only Most useful test? |
ECG Bloods - EUC, FBC CXR Useful - ECHO |
|
|
Role of digoxin in heart failure? |
Symptomatic management - patients already on max therapy + ongoing symptoms - Or AF not responding to maximal BB or BB not tolerated No mortality benefit but reduces hospitalisations and symptoms |
|
|
Role of ivabradine in heart failure? |
Ongoing elevated resting heart rate > 70 either due to maxed BB or not tolerant of BB Improves outcomes |
|
|
Indication for Cardiac defibrillator or CRT? |
Post sudden cardiac arrest due to VT/VF LVEF < 35% or AMI+<30% CRT - symptomatic EF< 35% + Broad QRS Greatest > 150 ms |
|
|
Common causes for AF? |
Hyperthyroidism Anaemia OSA Valvular disease - mitral valve IHD CCF HTN ETOH, caffeine |
|
|
Tests to assess new AF? |
FBC - anaemia, infection EUC , CMP - electrolyte ECHO ECG CXR - pulmonary disease - TSH, LFT |
|
|
3 types of AF |
Paroxysmal - self resolves usually within 48 hrs Persistent - continues until reverted with meds Permanent - chronic due to acceptance by cardio or no responding to therapy |
|
|
Trial comparing rate vs rhythm control in AF? |
AFFIRM TRIAL Rate = rhythm |
|
|
CHADSVAS? |
Congestive heart failure HTN Age >74 - 2 Diabetes Stroke / TIA Vascular disease - PVD, CAD Age 65-74 - 1 Sex - female |
|
|
Moa of dabigatran? |
direct thrombin inhibitor - factor II All the others are factor Xa inhibitors Warfarin - II, VII, IX, X |
|
|
Management of thrombosis of superficial femoral vein |
anticoagulation/ !! It is actually a DEEP vein ! and proximal so high risk 3 months if provoked 6 months unprovoked Indefinite if ongoing major risk factor or recurrent episode |
|
|
Rate of occult DVT with superfical thrombophlebitis? |
25% |
|
|
Management options for thrombophlebitits ? |
PO or topical NSAIDS - esp if due to a cannula Or LMWH - clexane 40mg daily 4 weeks |
|
|
Tests required prior to starting heparin? |
FBC - hb and platelets Coags - APTT, INR EUC - Cr |
|
|
Rate of post thrombotic syndrome? |
60% of DVTs complicated with post thrombotic syndrome Pain, swelling, varicose eczema, skin thickening, staining |
|
|
Treatment of DVT |
Graduated compression stocking 30-40mmhg 18 months Anticoagulation - Clexane, warfarin or NOAC Monitor for PE, extension etc --> if occurs on therapy or CI to anticoagulation --> inferior vena cava filter |
|
|
T/f 1. Physical activity reduces LDL and TG and increased HDL 2. physical activity increases insulin sensitivity and lowers BP 3. Mediterranean diet is not associated with reduced total mortality 4. 2.5hrs of moderate exercise /week results in 10% reduction in mortality risk |
1. true 2. True 3. false - it is and reduced CVD risk 4. FALSE - 19% reduction CHECK 2014 |
|
|
Resource for Sudden cardiac death in younger people ? |
Australian genetic heart disease registry |
|
|
History for Sudden cardiac death? |
family history of SCD Drownings Epilepsy Recurrent syncope Premature vascular disease History of CP, SOB, syncope, exercise intolerance |
|
|
Causes of SCD in younger individuals? |
1. Structural - Cardiomyopathy (dilated, hypertrophic, arrhythmogenic RV), myocarditis, CAD, Congenital heart disease 2. Non-structural - Long QT, Brugada, catecholaminergic pVT |
|
|
Usual inheritance pattern of causes of SCD? |
usually AD if 50% risk in children and first degree relatives |
|
|
Chest pain red flags? |
Dizziness/syncope Radiation to arms/jaw thoracic back pain Sweating Palpitations Dysnoea Pain on inspiration - pleuritic pallor PMHx - DM, CAD, HTN |
|
|
Tumours causing chest pain ? |
Lung cancer Mets to ribs Tumours of spinal cord or meninges with referred pain |
|
|
Causes of chest pain |
Common - anxiety, angina, MSK - chest wall Serious - AMI, unstable angina, dissection, PE, pulmonary infarction, Tension pneumothorax, pneumonia, mediastinitis, ruptured oesophagus, tumours (lung, rib mets) Other - GORD, biliary, oesophageal spasm, psychogenic, rib fracture, trauma, pancreatitis, ZOSTER, spinal dysfunction, peptic ulcer |
|
|
20% of ami that are silent? |
20% |
|
|
Chest pain - important history questions? |
Pain - site, onset, duration, offset, precipitants, relieving factors, quality (pleuritic), radiation, positional SOB Syncope Fever, weight loss, night sweats cough, haemoptysis Cardiac RF - age, smoking, lipids, HTN, CAD, F.Hx PE Risk factors - immobility, cancer, oestrogen Trauma, reflux, rash, |
|
|
chest pain with syncope - DDx? |
AMI PE Dissecting aneurysm Aortic stenosis |
|
|
chest pain - pleuritic ddx? |
Pneumonia PE Pneumothorax pericarditis pleurisy MSK |
|
|
Chest pain with thoracic component or radiation DdX? |
Dissecting aortic aneurysm AMi Pericarditis Peptic ulcer Biliary colic cholecystitis Oesophageal spasm thoracic spinal dysfunction |
|
|
Important exam for Chest pain ? |
General - mentation, ABC, Cyanosis, sweating, hemiparesis, tendon xanthomata Pulses - bilateral radial + femoral BP Temp Spo2 Chest wall palpation + spine - tenderness/zoster rash DVT signs Chest - pneumothorax, midline trachea, friction rub, basal creps/crackles, murmurs Abdomen - murphys, tenderness |
|
|
65 yo with chest pain and no femoral pulses dx? |
Aortic dissection May have associated hemiparesis |
|
|
Pleural friction rub? |
Pleurisy Pulmonary infarction |
|
|
sudden, severe andmidline, has a tearing sensation and is usuallysituated retrosternally and between the scapulae dx? Main clinical finding? |
Aortic Dissection Radio-femoral delay or absent femoral pulses Haemodynamic collapse |
|
|
Chest pain - Often sudden onset• Pain usually localised without radiation• Sharp knife-like pain• Continuous pain with sharp exacerbations• Aggravated by inspiration, sneezing and coughing Dx? |
Pleuritis Secondary to pneumonia, pulmonary infarction, tumour infiltration, connective tissue disease - SLE |
|
|
Epidemic pleurodynia (Bornholmdisease) What is this? |
unilateral sharp chest pain following an URTI Commonly Coxsackie B Normal CXR, settles in 1 week with simple analgesia. Dx of exclusion |
|
|
Cardinal sign of pericarditis ? |
pericardial friction rub |
|
|
Chest pain - pleuritic (the commonest), aggravated by coughand deep inspiration, sometimes brought on byswallowing; worse with lying flat, relieved bysitting up Dx? |
Pericarditis |
|
|
Types of pneumothorax? |
Primary or secondary (to underlying pathology) Acute or chronic Spontaneous or traumatic (positive pressure ventilation or rib fractures) |
|
|
Chest pain 35 yo central into the back which recurs following hot drinks and is relieved by GTN DDx |
Oesophageal spasm Ddx angina , peptic ulcer |
|
|
Important causes of chest pain in children? |
Trauma Pneumonia Ischemia - exercise induced, long standing diabetes, sickle cell Sickle cell crisis Asthma |
|
|
Causes of angina? |
CAD valvular lesions - AS Rapid arrhythmias anaemia Prinzmetal angina / coronary vasospasm vasculitis Trauma Collagen disease |
|
|
Important considerations prior to giving GTN for angina? |
Patient sitting or lying down No sildenafil or other PDE5 inhibitors in the last 24 hrs Advise of headache BP > 100 Systolic If pain rapidly relieved spit out the rest of the tablet |
|
|
Management of coronary vasospasm? |
CCB and nitrates Avoid BB |
|
|
3 features of AMI on ECG? |
ST elevation with reciprocal ST depression T wave - hyperacute, then flattening then inversion Deep broad Q wave |
|
|
Peak of trop rise time? |
10 hrs Rising at 3-6 hrs Persists for 5-14 days |
|
|
which test is better for acute re-infarction - cardiac Ck or trop |
CK - drops faster - by 48 hrs Vs trop 5-14 days |
|
|
First line management of STEMI/ cardiac chest pain |
ECG - STEMI or NSTEAC Immediate ambulance transfer to center for PCI or thrombolysis Oxygen if sats < 93 IV line +/- fluids Aspirin 300mg GTN 300mg SL tab or spray - 5 minutely max 3 ensuring BP>100 systolic Morphine 2-5mg Murtaghs |
|
|
Long term management of CAD following STEMI? |
Cardiac rehabilitation Meds - antiplatelets (Aspirin+/-clopidogrel), statin, ACEI, BB - titrate to max tolerated doses Weight maintenance BMI 20-25, or normal waist circumference no smoking Education and counselling regarding lifestyle changes and adherence to meds Regular exercise Diet - low salt, low saturated fat, high fibre, high omega 3 fatty acids |
|
|
Complications of AMI ? |
Arrhythmia, cardiac arrest, death Ventricular failure Pericarditis - acute - first few days Dresslers - weeks -months - pericarditis, effusion, fever LV aneurysm - leading to arrhythmia or thromboembolism Ventricular septal rupture Chordae tendinae rupture of MV Depression/ anxiety |
|
|
Pneumothorax requiring drain? |
> 25 % or symptomatic 3cm from top 2cm from side on CXR |
|
|
Recurrence rate for spontaneous primary pneumothorax? |
30-50% |
|
|
Management of GORD? |
Weight loss if overweight Avoid coffee, etoh, spicy foods Avoid large meals or overeating Antacids - gaviscon or mylanta plus If persistent - H2 blocker (cimetidine or ranitidine) or PPI - omeprazole Murtagh |
|
|
Important arrhythmias causing palpitations not to be missed? |
Sick sinus syndrome VT / torsades Atrial fibrillation complete heart block Second degree heart block type 2 SVT WPW Electrolyte disturbance - hypok/mg/bsl Long QT Symptomatic bradycardia |
|
|
Common causes of palipations? |
Anxiety PVCs or PAC Sinus tachy - fever, sport, emotion, stress drugs - stimulants, cocaine SVT |
|
|
Common causes of tachyarrhymias ? |
Ischaemic heart disease thyrotoxicosis HTN heart failure Mitral disease ASD |
|
|
Tumour causing palpitations? |
Phaeochromocytoma |
|
|
Drugs causing palpitations? |
Etoh cocaine/amphetamines Caffeine Theophilline Alendronate Antipsychotics Anti-arrhythmics Antidepressants - TCA, MOAi Atropine, hyoscine Digitalis Diuretics - low K/Mg GTN Sympathomimetics - pseudoephedrine, salbutamol Thyroxine |
|
|
Palpitations + Syncope DDX |
Sick sinus syndrome Complete heart block Aortic stenosis CVA / TIA |
|
|
Triad of AS? |
Chest pain Syncope Heart failure with SOB, PND, orthopnoea |
|
|
HR of sinus tachy |
100-150 usually > 150 = SVT, rAF, flutter, VT |
|
|
Exam for palpitations? |
Pulse, rate rhythm, character, regularity HS - ? murmur, 4th BP - HTN Temp - fever Thyroid - eyes, neck, Heart failure - JVP, lung base creps, pulsatile liver, peripheral oedema Anaemia, sweaty Liver disease/etoh abuse |
|
|
Waterhammer pulse? |
= collapsing = corrigans sign Aortic regurgitation |
|
|
Small volume pulse? |
Shock Mitral stenosis Constrictive pericardittis Pericardial effusion Aortic stenosis |
|
|
investigations for palpitations? |
ECG --> Holter monitor --> Loop /event recorder CXR FBC - anaemia EUC - electrolyte + Mg TSH - thyroid ECHO, EP study consider dig level, virus serology (myocarditis) |
|
|
Management of PAC? |
None - reassurance Avoid caffeine, etoh, stress, smoking BB - atenolol or metoprolol |
|
|
Example of each type of anti-arrhythmic? |
1 = sodium channel blockers membrane depression 1a - Procainamide 1b - Lignocaine 2 - BB - all 3 - Prolong action potential = Amiodarone, sotalol 4 - CCB - Nondihydropyridine - diltazem, verapamil |
|
|
common SE of BBs |
Fatigue insomnia Nightmares hypotension Bronchospasm Also erectile dysfunction, worsening BSL control, depression |
|
|
ECG features of WPW? |
Short PR Slurred upstroke of QRS - delta wave sudden episodes of SVT ALL --> Radiofrequency ablation |
|
|
Causes for AF? |
Ischaemia Thyroid Etoh abuse, binge Anaemia OSA Mitral valvular disease Cardiomyopathy |
|
|
Agents for chemical cardioversion of AF? |
Sotalol Amiodarone Flecainide - only with structurally normal heart |
|
|
Modifiable RF for CAD? |
HTN Lipids Smoking Obesity Sedentary lifestyle EtOH excess Poor nutrition Mental stress |
|
|
Non modifiable CAD risk factors |
Family history Age Male Cultural background/genetic DM, CKD |
|
|
Complications of HTN? |
IHD Heart failure / LVH Dissection AAA PVD CVA + Vascular Dementia CKD - hypertensive nephrosclerosis Hypertensive retinopathy SAH / ICH |
|
|
Most common cause of death from HTN> |
Stroke 45% heart failure 35% |
|
|
Causes of HTN? |
Essential 90-95% Kidney - GN, Reflux nephropathy, RAS, diabetes, analgesic, chronic pyelonephritis Endocrine - Conns, ushing syndrome, phaechromocytoma, OCP, acromegaly Coarctation PAN Drugs - NSAIDS, corticosteroids Pregnancy |
|
|
Age to consider secondary causes of hypertension? Other factors? |
< 40 yrs Poor response/resistance to pharmacotherapy with good compliance Malignant hypertension Physical findings, or lab findings |
|
|
Clinical exam features indicating secondary cause of HTN? |
Abdominal systolic bruit - Kidney artery stenosis Proteinuria, haematuria, casts - GN Bilateral kidney masses +/- haematuria - PCKD Claudication + delayed femoral pulse - coarctation Progressive nocturia, weakness - Conn's Paroxysmal HTN, headache, pallor, sweating, palpitations - phaeochromocytoma Signs of acromegaly Truncal obesity + striae - cushing |
|
|
Meds that increase BP |
NSAIDS Corticosteroids COCP/HRT/DEPOT Decongestants, amphetamine MOAi , venlafaxine Appetite suppressants EtOH Liquorice Tacrolimus, cyclosporin Bupropion |
|
|
Routine tests for LFTs? |
Fasting BSL Total cholesterol, HDL, LDL, Trigs EUC - Cr, eGFR, ACR, K, Na Uric Acid Hb, Hct UA ECG |
|
|
Non pharm management of HTN? |
reduce EtOh Exercise Weight loss Smoking cessation Sodium < 100mmol Reduce stress Dietary - Lacto-veg diet, Mg supplementation, High Ca, low fat, low caffeine, low liquorice Manage OSA |
|
|
SE of thiazide diuretics? |
Rashes Sexual dysfunction Weakness Blood dyscrasias Muscular cramps Hypo - K, Na Hyper - urate, BSL, Lipids |
|
|
SE of CCB |
Headache Flushing Ankle oedema Palpitations Dizzy Nausea Constipation - verapamil Nocturia, urinary frequency Gum hyperplasia |
|
|
2 major risk factor profiles of cholesterol levels for CAD? |
high LDL + Low HDL Ratio of LDL:HDL > 4 cholesterol > 7.8 |
|
|
Risk reduction following a 10% reduction in total cholesterol? |
20% reduction in CAD after 3 yrs murtagh |
|
|
Common causes of secondary dyslipidaemia? |
Hypothyroidism Nephrotic syndrome T2DM Cholestasis Anorexia Nervosa Obesity Kidney impairment Alcohol excess Obstructive liver disease Meds - thiazides |
|
|
Symptoms of heart failure? |
Exertional dysnoea, dysnoea at rest, orthopnoea, PND Irritating cough at night Lethargy, fatigue Weight change - gain or loss Dizzy spells / syncope Abdominal discomfort? Palpitations Ankle oedema |
|
|
Signs of heart failure |
Left - 3rd HS, Basal crep, low volume pulse, tachycardia, tachypnoea, lateral apex beat, pleural effusion, poor perfusion Right - Raised JVP, Pulsatile liver, peripheral oedema, Ascites, hepatomegaly, RV heave |
|
|
Causes of systolic heart failure? |
1. CAD/IHD - 75% HTN Valvular - aortic or mitral incompetence High output - anaemia, thyrotoxicosis, berriberri, pagets Idiopathic dilated cardiomyopathy Cardiomyopathy - viral, alcoholic, diabetic, familial, sarcoid, SLE, Arrhythmias - AF Scleroderma etc Pulmonary disease - PHTN - right heart failure |
|
|
Common causes of diastolic heart failure? |
IHD HTN Aortic Stenosis AF (inadequate filling) Hypertrophic cardiomyopathy Pericardial disease Infiltrative disease |
|
|
Investigations for heart failure? |
ECHO ECG - IHD CXR - effusions, APO Spirometry - r/o pulmonary disease BNP / pro-BNP FBC - anaemia Electrolytes - important to monitor Cr - drug therapy LFT - congestive hepatomegaly UA TFT Viral serology if unsure of cause |
|
|
CXR findings of heart failure? |
Cardiomegaly Interstial oedema Upper lobe diversion Fluid in fissures Oedema in perihilar area (bat winging) Small basal pleural effusions Kerley B lines Frank pulmonary oedema |
|
|
drugs that worsen heart failure? |
NSAIDS Corticosteroids TCA CCB - non-dihydro Anti-arrhythmics - quinidine Macrolide AB Type 1 antihistamines H2 antagonsit Glitazones TNF alpha inhibitors Etoh illicit drugs - cocaine |
|
|
DDx localised wheeze? |
Foreign body Mucus plug bronchial Carcinoma Extrinsic pressure - mediastinal LN |
|
|
DDx for generalised wheeze? |
Asthma Obstructive bronchitis Bronchiolitis PND - with CCF |
|
|
Questions to differentiate asthma and COPD |
Age < 35 Smoking history Chronic cough Dyspnoea - variable / constant + progressive Response to bronchodilators Reversibility of air flow obstruction on spirometry |
|
|
Dyspnoea DDx Common Serious Others? |
Common - Bronchial asthma, Bronchiolitis (kids), COPD, ageing/lack of fitness, Left heart failure, obesity Serious - CVD (AMI, arrhythmia, PE, Fat embolism, PHTN, Dissection, Cardiomyopathy, tamponade, anaphylaxis), Resp ( Pneumothorax, foreign body, Asthma, COPD, ILD, effusion, TB, ADRS), Cancer (lung, any), Infection (Pneumonia, SARS, avian influenza, epiglottitis, Neuro (polio, neuromuscular disease) Other - idiopathic pulmonary fibrosis, extrinsic allergic alveolitis, sarcoidosis, metabolic acidosis, radiotherapy, renal failure, diabetes, anaemia, anxiety, obesity hypoventilation |
|
|
Drugs causing interstitial fibrosis |
Methotrexate Bleomycin Cyclophosphamide Amiodarone Sulphasalazine Nitrofurantoin gold salts adrenergic nasal sprays |
|
|
Poisons causing hyperventilation? |
Salicylates Alcohol theophylline Ethylene glycol |
|
|
Red flags for Dyspnoea? |
History - sudden onset, IHD, Migrant (africa/asia), recent travel, asthma/allergy, unexplained weight loss, significant trauma, HIV, Drug (social + biologics) Exam - Cyanosis, pallor, dyspnoea at rest, fever, hypotension, tachycardia, tachypnoea, chest wall signs, altered GCS, elevated JVP, wheeze, urticaria |
|
|
DDX sudden onset SOB? |
pneumothorax PE AMI Arrhythmia Foreign body Anaphylaxis Flash APO Hyperventilation Tamponade |
|
|
DDx for rapid SOB - over hours (not minutes) |
AMI Pneumonia CCF/APO Asthma COPD exacerbation DKA Hyperventilation Poisons Pericardial tamponade Altitude - high |
|
|
Causes of SOB that develop over longer periods of time days/weeks/months/years |
CCF Pleural effusion Carcinoma of bronchus Months - years COPD TB Fibrosing alveolitis Pneumoconiosis Anaemia Hyperthyroidism Obesity |
|
|
Causes of pulmonary crackles? 2 most important tests? |
Pneumonia CCF/APO bronchiectasis Chronic bronchitits Absestosis Pulmonary fibrosis Extrinsic allergic alveolitis CXR + spirometry |
|
|
Describe the flow loop curve for asthma, COPD, restrictive lung disease, fixed major airway obstruction in relation to flow and volume. |
Asthma - normal volume but peaked with scooped out curve due to limitd flow COPD - eventually reduced volume with similar loop above Restrictive - relatively normal shape but reduced Volume Fixed obstruction - chopped off top limiting flow but normal volume |
|
|
Size of pleural effusion to be detected clinically? On CXR? |
Clinical 500ml CXR > 300ml Normal 20-30ml |
|
|
Causes of pleural effusion? |
cardiac failure - 90% Pneumonia Cancer - lung or ovarian or haematological Hypothyroidism Liver failure Hypoproteinaemia - nephrotic syndome Connective tissue - SLE, RA Sarcoid HIV Infarction |
|
|
Causes of interstitial pulmonary fibrosis? |
Sarcoidosis Idiopathic pulmonary fibrosis Hypersensitivity pneumonitis Drug induced Lymphangitis carcinomatosis Rheumatoid Vasculitis, Scleroderma, SLE |
|
|
Clinical features of pulmonary sarcoidosis? |
bilateral hilar Lymphadenopathy on CXR Cough, fever, malaise Arthralgia Erythema nodosum Ocular - anterior uveitis Any organ! |
|
|
Treatment of sarcoidosis? |
Prednisone |
|
|
Most common interstitial lung disease? |
idiopathic pulmonary fibrosis |
|
|
Types of extrinsic allergic alveolitis? |
Farmers lung - actinomycetes Bird fanciers lung - avian protein Mushroom workers Cheese washers Wood pulp workers rat handlers Coffee workers ...... many types!! |
|
|
Types of pneumoconioses? Associated work? |
Coal workers Siderosis (iron - mining and welding) Silicosis ( stone cutting, blasting, mining) Asbestosis (mining, shipbuilding, insulation, power stations) |
|
|
Different types of occupational pulmonary disease? |
Occupational asthma Pneumoconiosis / fibrosis - asbestosis, scilicosis Extrinsic allergic alveolitis - inflammatory reaction to the particles lung cancer, mesothelioma - asbestosis, hydrocarbons Pleural plaques - asbestosis |
|
|
Causes for hyperventilation? |
drugs Asthma Thyrotoxicosis Panic attacks/anxiety Poisons |