Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
248 Cards in this Set
- Front
- Back
|
Colorectal cancer |
1. 3rd most common cancer in the United States (in men and women)
2. Virtually all colorectal tumors arise from adenomas and the majority are endoluminal adenocarcinomas arising from the mucosa-->adenocarcinoma. Rarely there are carcinoid tumors, lymphomas, and Kaposi's sarcoma (HHV 8 in AIDS pts) |
|
|
Colorectal cancer (CRC) screening
|

1. fecal occult blood test- poor sensitivity and specificity. PPV is only 20%, but all patients with a positive FOBT need a colonoscopy anyway
2. Digital rectal exam (DRE)- only about 10% of tumors are palpable by rectal examination 3. Colonscopy- the most sensitive and specific test-- the diagnostic study of choice for patients with a positive FOBT. Diagnostic and therapeutic-- biopsy or polypectomy. 4. Flexible sigmoidoscopy- can be used to reach teh area where approximately 50% to 70% of polyps and cancers occur (with a 60cm scope). Can be diagnostic in about 2/3 of all CRCs 5. Barium enema- evaluates entire colon- complementary to flex sig. Disadvantage is the any abnormal findings need to be evaluated by colonscopy 6. Carcinoembryonic antigen (CEA)- not useful for screening--useful for baseline and recurrence surveillance. Has some prognostic significance-- patients with a preoperative CEA >5 ng/mL have a worse prognosis. |
|
|
Clinical staging of CRC
|
CT scan of chest, abd, pelvis and by physical exam (ascites, hepatomegaly, lymphadenopathy etc)
|
|
|
CRC patterns of spread (4)
|
1. Direct extension- circumferentially and then through the bowel wall to later invade other abdominoperitoneal organs
2. Hematogenous- portal circulation to liver - liver is the most common site of distant spread. Or lumbar/vertebral veins to lungs 3. lymphatic- regionally 4. transperitoneal and intraluminal |
|
|
Risk factors for Colorectal Cancer (CRC)
|
1. Age- everyone over the age of 50 years is at increased risk
2. adenomatous polyps- these are pre-malignant lesions, but most do not develop into cancer. villous adenomas have higher malignant potential than tubular adenomas. The larger the size and the greater the number of polyps the higher the risk of cancer 3. personal history of prior CRC of adenomatous polyps 4. Inflammatory bowel disease (IBD) - both Ulcerative Colitis (UC) and Crohn's disease pose an increased risk for CRC, but UC poses a greater risk. Incidence of CRC is 5-10% at 20 years and 12-20% at 30 years with UC 5. Family history- multiple first degree relatives with CRC or any first-degree relative diagnosed with CRC or ademona under age 60 6. dietary factors- high fat, low-fiber diets 7. major polyposis syndromes (FAP, Gardner's syndrome, Turcot's syndrome, Peutz Jeghers, Familiar juvenile polyposis coli, hereditary non polyposis CRC (HNPCC) |
|
|
Familial adenomatous polyposis (FAP)
1. what is it? 2. what is the risk of CRC? 3. tx |

1. autosomal dominant disease characterized by hundreds of adenomatous polyps in the colon. the colon is always involved and the duodenum is involved in 90% of cases. Polyps may also form in the stomach, jejunum, and ileum.
2. The risk of CRc is 100% by the 3rd to 4th decade of life 3. prophylactic colectomy is usually recommended |
|
|
Gardner's Syndrome
1. what is it? 2. what is the risk of CRC? |

- polyps plus osteoma, dental abnormalities, benign soft tissue tumors, desmoid tumors, sebaceous cysts
- risk of CRC is 100% by age 40 |
|
|
Turcot's syndrome
1. inheritance pattern? 2. what does it affect? |
1. autosomal recessive
2. FAP tumors plus cerebellar medulloblastoma or gliobastoma multiforme (think Turcots- turban-- affects your brain) |
|
|
Peutz-Jeghers syndrome
1. what is it? 2. what are some clinical features? 3. malignant potential compared to ademonas? 4. which cancers are pts at increased risk for? 5. other potential complications? |

1. Single or multiple hamartomas that may be scattered through the entire GI tract: small bowel (78%), colon (60%), stomach (30%)
2. pigments spots around lips, oral mucosa, face, genitalia, and palmar surfaces 3. unlike adenoma, hamartomas have a very low malignant potential 4. slightly increased incidence in various carcinomas (e.g. stomach, ovary, breast, cervix, testicle, lung). 5. intussception or GI bleeding may occur |
|
|
Familial juvenile polyposis coli
|
1. rare, presents in childhood, only small risk of CRC
2. more than 10 and up to 100s of juvenile colon polyps |
|
|
Hereditary Nonpolyposis CRC (HNPCC- Lynch syndrome)
|
1. lynch syndrome I- site specific CRC- early onset CRC, absence of antecedent multiple polyposis
2. lynch syndrome II- (cancer family syndrome)- all features of Lynch I plus increased number and early occurrence of other cancers (e.g. female genital tract, skin, stomach, pancreas, brain, breast, biliary tract) |
|
|
Clinical features of CRC
1. most common symptom? 2. other symptoms |
1. the presence of symptoms is typically a manifestation of relatively advanced disease. Most symptoms include melena, hematochezia, abdominal pain, change in bowel habits, or unexplained iron deficiency anemia
2. Signs and symptoms are potentially common to all locations a. abdominal pain is the most common presenting symptom. Can be caused by partial obstruction or peritoneal dissemination. Remember that CRC is the most common cause of large bowel obstruction in adults. Colonic perforation can lead to peritonitis and is the most life-threatening complication. b. weight loss c. blood in stool d. may be asx |
|
|
Right-sided CRC tumors
|

- obstruction is unusual because of the large luminal diameter (the cecum has the largest diameter of any part of the colon) allowing the tumor growth to go undetected
- common findings - occult blood in stool, iron deficiency anemia, and melena (because blood is partially digested by the time it comes out giving it a darker hue) - triad of anemia, weakness and RLQ mass (occasionally) - change in bowel uncommon |
|
|
A patient presents with anemia, weakness and a RLQ mass on exam- what is a likely diagnosis?
|
Right sided colon cancer
|
|
|
Left-sided CRC tumors
|

- the descending colon has a smaller diameter than the right so signs of obstruction are more common
- change in bowel are more common- alternating diarrhea and constipation-- narrowing of the stools - "pencil stools" - hematochezia is more common (red blood-- since it doesn't have as far to go as in the case of a right sided tumor- the blood is less digested/dark) |
|
|
Rectal cancer
1. how common 2. symptoms and signs |

- 20-30% of all CRCs
- hematochezia- most common symptom - tenesmus- feeling the need to pass stool constantly even though the colon is empty- can be very painful - rectal mass- feeling of incomplete evacuation of stool (due to mass) |
|
|
Treatment of CRC
1. only cure 2. role of CEA levels 3. role of adjuvant therapy (chemo and radiation) 4. F/U 5. when do recurrences usually happen? |
1. Surgery is the only curative treatment of CRC- surgical resection of tumor containing bowel as well as resection of regional lymphatics
2. CEA level should be obtained before surgery- can given an indication of prognosis (> 5ng/mL = worse px), also used for F/U 3. chemo and radiation use depends on the stage of the cancer 4. F/U is important and varies a. Stool guaiac test b. annual CT of abd/pelvis and CXR for up to 5 yrs c. colonoscopy at 1 yr and then every 3 years d. CEA levels are check periodically (ever 3-6 months). - a subsequent increase in CEA is sensitive marker of recurrence. Often, 2nd look operations are based on elevated CEA levels post-op. Very high levels suggest liver involvement 5. about 90% of recurrences occur within 3 years after surgery |
|
|
Nonneoplastic colon polyps (types, which is most common?)
|
1. benign lesions with no malignant potential
a. hyperplastic (metaplastic) polyps are the most common (90%) nonneoplastic polyps-- generally remain small and asx b. no specific therapy required, but they can be difficult to distinguish from neoplastic polyps and so are commonly removed c. juvenile polyps-- typically in children younger than 10 years are high vascular and common so they should be removed d. inflammatory polyps- pseudopolyps-- associated with UC |
|
|
Adenomatous polyps
1. three types - and corresponding malignancy potential 2. what features help determine malignant potential? 3. treatment |
benign lesions, but have significant malignant potential, precursors of adenocarcinoma
1. can be one of three types-- villous, tubulovillous, and tubular. tubular is the most common- up to 60-80%-- smallest of malignancy. villous has greatest risk of malignancy 2. can determine malignant potential by following: a. size- the larger the polyp the greater the malignant potential b. histologic type- see above c. atypia of cells (increased nuclear to cytoplasmic ratio etc) d. Sessile (flat- more likely to be malignant) vs pedunculated (on a stalk) 3. tx- complete removal of the polyp |
|
|
Diverticulosis
1. cause 2. risk factors 3. prevalence with age 4. most common site affected |
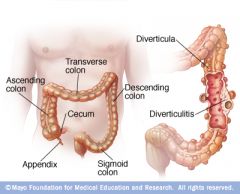
1. Caused by increased intraluminal pressure- inner layer of colon bulges through focal area of weakness in colon wall (usually an area of blood vessel penetration)
2. Risk factors- low fiber diets- constipation causes intraluminal pressures to increase. Positive family history 3. prevalence increases with age 4. The most common location is the sigmoid colon-- however diverticular may occur anywhere in the colon |
|
|
Clinical features of diverticulosis
1. sx |
- usually asymptomatic and discovered incidentally on barium edema or colonscopy done for another reason
- may have vague LLQ discomfort, bloating, constipation/diarrhea etc - only 10-20% become symptomatic-- develop complications such as diverticular bleeding or diverticulitis |
|
|
Diagnosis (test of choice, etc)
|
1. Test of choice- barium enema
2. abdominal Xrays are usually normal and are not diagnostic |
|
|
Treatment of diverticulosis
|
1. High fiber foods (such as bran) to increase stool bulk
2. psyllium (if patient cannot tolerate bran)- dietary fiber not absorbed by the small intestine |
|
|
Complications of diverticulosis
|
1. Painless rectal bleeding (up to 40% of patients) - bleeding is usually clinically insignificant and stops spontaneously. No further treatment is necessary in these patients. Bleeding can be severe in about 5% of patients. In many cases the bleeding stops spontaneously. Colonoscopy may be performed to locate the site of bleeding (or mesenteric angiography in certain cases). If bleeding is persistent and/or recurrent, surgery may be needed (segmental colectomy)
2. Diverticulitis- Occurs when feces become impacted in the diverticulum, leading to erosion and microperforation. Can be complicated or uncomplicated. Uncomplicated diverticulitis account for most cases and refers to diverticulitis without abscess formation, colovesical fistula (into bladder) , obstruction, and free colonic perforation |
|
|
Diverticulitis
1. cause 2. complicated vs uncomplicated 3. clinical features |
1. occurs in 15-25% of patients with diverticulosis when feces become impacted in the diverticulum, leading to erosion and microperforation
2. complications include- free colonic perforation, colovesical fistula (fistula between bowel and bladder- 50% of fistulas arising from diverticulitis), abscess formation, obstruction 3. clinical features- fever, LLQ pain, leukocytosis. May also see alteration in bowel habits (constipation or diarrhea), vomiting and sometimes a painful mass on rectal exam if inflammation is near the rectum - lower GI bleeding is rare in diverticulitis but common in diverticulosis |
|
|
Diagnosis of Diverticulitis
|
1. CT Scan of abdomen and pelvis with oral and IV contrast is the test of choice-- may reveal a swollen, edematous bowel wall or an abscess
2. Abdominal xrays are helpful in ruling out potential causes of LLQ pain, ileus, obstruction (indicated by air-fluid levels), distention and perforation |
|
|
Treatment of diverticulitis
1. mainstays of treatment 2. when is surgery indicated? |
1. uncomplicated diverticulitis is managed by IV antibiotics, bowel rest (NPO), IV Fluids. Mild episodes can be treated on an outpatient basis if patient is reliable and has few or no comorbid conditions. If symptoms persist after 3-4 days, surgery may be necessary. Antbiotics should be continued for 7-10 days. After successful treatment, about 1/3 have recurrence.
- Surgery is recommended for recurrent episodes (resection of the involved segment) - Complicated diverticulitis-- surgery is indicated |
|
|
Angiodysplasia-
|
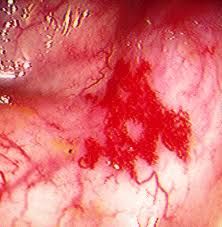
Tortuous, dilated veins in the submucosa of the colon (usually proximal) wall
- a common cause of lower GI bleeding in patients over the age of 60 - bleeding is usually low grade, but 15% of patients may have massive hemorrhage if veins rupture - diagnosed by colonoscopy (preferred over angiography) - in about 90% of patients, bleeding stops spontaneously - It can frequently be treated by colonoscopic coagulation of the lesion. If bleeding persists, a right hemicolectomy should be considered |
|
|
Acute Mesenteric Ischemia
1. cause 2. 4 causes 3. mortality |
1. Results from a compromised blood supply, usually due to superior mesenteric vessels
2. 4 causes- a. Arterial embolism (50% of cases), almost all emboli are of cardiac origin (atrial fibrillation, MI, valvular disease), b. Arterial thrombosis (25% of cases)- most of these patients have atherosclerotic disease (coronary artery disease (CAD, PVD, stroke) at other site, Acute occlusions occurs over pre-existing atherosclerotic disease. The acute event may be due to decrease in cardiac output (e.g. resulting from MI, CHF, or plaque rupture), Collateral circulation has usually developed. c. Non-occlusive mesenteric ischemia (20% of cases) - due to splanchnic vasoconstriction secondary to low cardiac output, typically seen in critically ill elderly patients. d. Venous thrombosis (<10% of cases)- many predisposing factors -- e.g infection, hypercoaguable states, oral contraceptives, portal HTN, malignancy, pancreatitis 3. mortality- the overall mortality rate for all types is about 60-70%. If bowel infarction has occurred, the mortality rate can exceed 90% |
|
|
Clinical features of acute mesenteric ischemia
|
1. classic presentation is acute onset of severe abdominal pain disproportionate to physical findings-- pain is due to ischemia and possibly infarction of intestines, analogous to MI in CAD
- the abdominal examination may appear benign even when there is severe ischemia which can lead to a delay in diagnosis - the acuteness and severity of the pain vary depending on the type of acute mesenteric ischemia - anorexia, vomiting - GI bleeding (mild) - peritonitis, sepsis, and shock may be present in advanced disease |
|
|
Diagnosis of acute mesenteric ischemia
|

1. mesenteric angiography- definitive diagnostic test
2. obtain a plain film of the abdomen to exclude other causes of abdominal pain 3. "Thumbprinting" on barium enema is due to thickened edematous mucosal folds |
|
|
Treatment of acute mesenteric ischemia
|
1. supportive measures- IV Fluids and broad spectrum antibiotics
2. direct intra-arterial infusion of papervine- vasodilator into the the superior mesenteric system during arteriography is the therapy of choice for all arterial causes of acute mesenteric ischemia. This relieves the occlusion and vasospasm 3. Direct intra-arterial infusion of thrombolytics or embolectomy may be indicated in some patients with embolic acute mesenteric ischemia 4. heparin anticoagulation is the treatment of choice for venous thrombosis 5. surgery (resection of non-viable bowel) may be needed in all types of acute mesenteric ischemia if signs of peritonitis develop |
|
|
Chronic Mesenteric Ischemia
1. Cause 2. Symptoms 3. Diagnosis 4. Treatment |
1. Caused by atherosclerotic occlusive disease of the main mesenteric vessels (celiac artery, superior and inferior mesenteric arteries)
2. Abdominal angina- dull pain, typically postprandial (when there is increased demand for splanchnic blood flow)-- analogous to anginal pain in CAD, significant weight loss may occur secondary to this 3. Mesenteric ateriography to confirm 4. Surgical revascularization - leads to pain relief in 90% of cases |
|
|
Ogilvie's Syndrome
1. what is it? 2. What are the common causes? 3. How diagnosed? 4. treatment |
1. An unusual problem in which signs, symptoms, and radiographic evidence of large bowel obstruction are present, but there is no mechanical obstruction
2. Common causes- recent surgery or trauma, serious medical illness (e.g. sepsis, malignancy) and medications (narcotics, psychotropic drugs, anticholinergics) 3. The diagnosis cannot be confirmed until mechanical obstruction of the colon is excluded 4. Treatment- stopping any offending agent (e.g. narcotics) and supportive measures (IV Fluids, electrolyte repletion), decompression with gentle enemas or NG suction may be helpful, however if this fails then colonoscopic decompression is usually successful, with surgical decompression and cecostomy/colostomy as a last resort |
|
|
Pseudomembranous Colitis
1. aka 2. cause-- and when does it happen in relation to this? |
1. antibiotic associated colitis- many patients do not have grossly visible pseudomembranes
2. Antibiotic treatment kills organisms that normally inhibit the growth of Clostridium difficile, leading to its overgrowth and toxin production. - almost all antibiotics have been associated with it, but the most frequently implicated are Clindamycin, Ampicillin and cephalosporins - symptoms usually begin within the first week of antibiotic therapy- however, it can start up to 6 weeks after cessation of antibiotic treatment - disease severity varies widely |
|
|
Clinical features of pseudomembranous colitis/ c. diff
|

1. profuse watery diarrhea (usually NO blood or mucus)
2. crampy abdominal pain 3. Toxic megacolon (in severe cases) with risk of perforation |
|
|
Diagnosis of pseudomembranous colitis/c. difficile
|

1. Demonstration of C. difficile toxins in the stool is diagnostic, but results take about 24 hours (95% sensitivity)
2. Flexible sigmoidoscopy is the most rapid test and is diagnostic, but because of comfort/expense it is infrequently used 3. Abd Xray to r/o toxic megacolon and perforation 4. leukocytosis is very common |
|
|
Treatment of pseudomembranous colitis/c. difficile
(including recurrence risk and adjuvant therapy) |
1. Discontinue the offending agent/antibiotic if possible
2. Metronidazole (flagyl) is the drug of choice but cannot be used in infants or pregnant patients 3. Oral vancomycin can be used if the patient is resistant to metronidazole or cannot tolerate it - regardless of the choice of antibiotic, recurrence may occur within 2-8 weeks after stopping the antibiotic. This occurs in 15-35% of successfully treated patients - Cholestyramine may be used as an adjuvant treatment to improve diarrhea |
|
|
Colonic Volvulus
1. definition 2. potential complications 3. most common sites affected |
1. Twisting of the a loop of intestine about its mesenteric attachment site
2. may result in obstruction or vascular compromise with the potential for necrosis and/or perforation if untreated 3. most common site is the sigmoid colon (75% of all cases), and the cecum (25% of all cases) |
|
|
Risk factors for volvulus (sigmoid vs cecal volvulus)
|

1. chronic illness, age, institionalization, and CNS disease increase the risk of sigmoid volvulus
2. cecal volvulus- due to congenital lack of fixation of the right/descending colon and tends to occur in younger patients 3. chronic constipation, laxative abuse, and antimotility drugs 4. prior abdominal surgery |
|
|
Clinical features of volvulus
|
1. Acute onset of colicky abdominal pain
2. obstipation (no passing gas or stool) and abdominal distention 3. anorexia, nausea and vomiting |
|
|
Diagnosis of volvulus
|

1. Plain films of the abdomen- a. sigmoid volvulus- omega loop sign (or bent inner-tube shape)- indicates a dilated sigmoid colon. b. cecal volvulus- distention of the cecum and small bowel- coffee bean sign indicates a large air-fluid level in the RLQ
2. Sigmoidoscopy- preferred diagnostic and therapeutic test for sigmoid volvulus-- can treat during this procedure by untwisting and decompressing the bowel in many cases 3. barium enema- reveals the narrowing of the colon at the point where it is twisted "bird's beak" DO NOT perform barium enema if strangulation is suspected. |
|
|
Treatment of volvulus
1. sigmoid 2. cecal |
1. sigmoid volvulus- nonoperative reduction- decompression via sigmoidoscopy is successful in 70% of cases. The recurrent rate is high so elective sigmoid colon resection is recommended
2. cecal volvulus- emergent surgery is indicated DO NOT perform barium enema if strangulation is suspected |
|
|
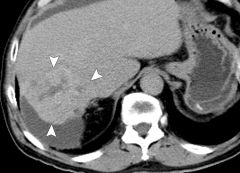
Cirrhosis
1. definition 2. reversible vs irreversible |
1. chronic liver disease characterized by fibrosis, disruption of the liver architecture, and widespread nodules in the liver. The fibrous tissue replaces damaged or dead hepatocytes
2. cirrhosis is generally irreversible when advanced. In early stages, specific treatment of the cause of cirrhosis may improve or reverse the condition. The point at which the disease becomes irreversible is unclear. |
|
|
What does the distortion of liver anatomy cause in cirrhosis (2 major events)?
|
1. Decreased blood flow through the liver with subsequent hypertension in the portal circulation (portal hypertension)-- this has widespread manifestations, including ascites, peripheral edema, splenomegaly, and varicosity of veins "back stream" in the circulation (gut, butt, caput-- gastric/esophageal varices, internal hemorrhoids, and caput medusa-dilated abdominal veins)
2. hepatocellular failure-- leads to impairment of biochemical functions, such as decreased albumin synthesis and decreased clotting factor synthesis |
|
|
Assessment of hepatic functional reserve in cirrhosis
|
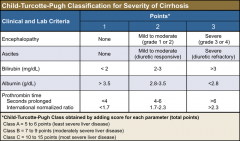
1. Child's classification- estimates hepatic reserve in liver failure-- used to measure disease severity and is a predictor of morbidity and mortality (based on ascites, bilirubin, encephalopathy, nutritional status, and albumin)
2. Child's class C indicates the most severe disease, while class A is milder |
|
|
Causes of cirrhosis (10)
|
1. Alcoholic liver disease - most common cause. Refers to a range of conditions from fatty liver (reversible, due to acute ingestion) to cirrhosis (irreversible). 15-20% of heavy drinkers develop alcoholic cirrhosis
2. Chronic hepatitis B or C infections- next most common causes 3. Drugs (acetaminophen toxicity, methotrexate) 4. Autoimmune hepatitis 5. Primary Biliary Cirrhosis (PBC), Secondary biliary cirrhosis 6. Inherited metabolic diseases (hemachromatosis, Wilson's disease) 7. Hepatic congestion secondary to right-sided heart failure, constrictive pericarditis 8. Alpha-1 antitrypsin deficiency (also causes emphysema) 9. hepatic veno-occlusive disease- can occur after a bone marrow transplantation 10. Non-alcoholic steatohepatitis (NASH) |
|
|
Clinical features of cirrhosis
|
1. some patients have no overt clinical findings, especially early in the disease
2. patients may have signs or symptoms suggestive of one or more of the complications of cirrhosis (portal hypertension, varices, ascites, hepatic encephalopathy, hepatorenal syndrome, spontaneous bacterial peritonitis (SBP), hyperestrinism, Coagulopathy, Hepatocellular carcinoma (HCC) |
|
|
Treatment of portal hypertension
|
TIPS - transjugular intrahepatic porto-systemic shunt
|
|
|
Esophageal varices
1. evaluation 2. clinical features 3. treatment |

1. variceal hemorrhage has a high mortality rate. patients with cirrhosis should be evaluated to document the presence of varices and risk of hemorrhage-- if present prophylactic measures should be taken such as non-selective beta blocker
2. massive hematemesis, melena, and exacerbation hepatic encephalopathy. 3. Fluids to maintain BP. IV abx prophylactically. IV octreotide is initiated and and continued for 3-5 days. Perform emergent upper GI endoscopy once the patient is stabilized for diagnosis and treatment of hemorrhage either with variceal band ligation or sclerotherapy. Give beta blockers in the long term to prevent re-bleeding - rectal hemorrhoids and caput medusae (distension of abdominal wall vessels are also possible) |
|
|
Ascites
1. definition 2. clinical features 3. diagnosis 4. treatment |

1. accumulation of fluid in the peritoneal cavity due to portal HTN - increased hydrostatic pressure and hypoalbuminemia - decreased oncotic pressure
2. abdominal distention, shifting dullness, and fluid wave 3. abd ultrasound can detect as little as 30 mL of fluid. Diagnostic paracentesis determines whether ascites is due to portal HTN or another process-- indications include new onset ascites, worsening ascites or suspected spontaneous bacterial peritonitis 4. treatment- bed rest, low sodium diet, and diuretics (furosemide and spironolactone), perform therapeutic paracentesis if tense ascites, shortness of breath or early satiety present. Peritoneovenous shunt or TIPS to reduce portal HTN |
|
|
Hepatic encephalopathy
1. cause (build up of?) 2. how prevalent in cirrhosis? 3. precipitants? |
1. toxic metabolites (there are many but ammonia is believed to be the most important)-- normally detoxified by the liver- accumulates and reaches the brain
2. occurs in 50% of cirrhosis to varying extent 3. alkalosis, hypokalemia (due to diuretics), sedating drugs (narcotics, sleep meds), systemic infection and hypovolemia |
|
|
Hepatic encephalopathy
1. clinical features 2. treatment |
1. decreased mental function, confusion, poor concentration, even stupor or coma.
- asterexis - "flapping tremor"- have the patient extend arms and dorsiflex the hands - not specific - rigidity, hyperreflexia - fetor hepaticus-- musty odor of breath 2. lactulose - prevents absorption of ammonia- metabolism of lactulose by bacteria in the colon favors formation of NH4+, which poorly absorbed from the GI tract-- thereby promoting excretion of ammonia - neomycin - antibiotic- neomycin - kills bowel flora, so decreases ammonia production by intestinal bacteria - diet: limit protein to 30-40 g/day |
|
|
Hepatorenal syndrome
1. what is it indicative of? 2. definition 3. precipitants 4. clinical features 5. treatment |
1. indicates end-stage liver disease
2. progressive renal failure in advanced liver disease, secondary to renal hypoperfusion resulting from vasoconstriction of renal vessels - this is a functional renal failure- kidneys are normal in terms of morphology, and no specific causes of renal dysfunction are evident. Does not respond to volume expansion 3. precipitated by infection or diuretics 4. clinical features- azotemia (inc BUN), oliguria, hyponatremia, hypotension, low urine output (<10 mEq/L) 5. Liver transplantation is the only cure-- in general the prognosis is very poor, and the condition is usually fatal without liver transplant |
|
|
Spontaneous Bacterial Peritonitis (SBP)
1. definition 2. etiologic agents 3. clinical features 4. diagnosis 5. treatment |
1. infected ascitic fluid, occurs in up to 20% of patients hospitalized for ascites
- usually occurs in patients with ascites caused by end-stage liver disease-- associated with a high mortality - 20-30% - high recurrence rate - up to 70% in the first year 2. e. coli (most common), klebsiella, strep pneumo 3. clinical features- abd pain, fever, vomiting, rebound tenderness, may lead to sepsis 4. diagnosis established by paracentesis and examination of ascitic fluid for WBCs (esp PMNs), gram stain with culture and sensitivities (WBC > 500, PMN >250) - positive ascites culture - culture negative SBP is common as well 5. treatment0 broad spectrum antbiotics- give specific antibiotic therapy once the organism is identified. clinical improvement should be seen in 24-48 hours. - repeat paracentesis in 2-3 days to document decrease is ascitic fluid PMN (<250) |
|
|
Hyperestrinism is liver failure/cirrhosis
|

1. spider angiomas- dilated cutaneous arterioles with central red spot and reddish extensions that radiate outward like a spider's web
2. palmar erythema 3. gynecomastia 4. testicular atrophy |
|
|
Coagulopathy secondary to liver failure
1. cause - what is elevated in terms of clotting tests? 2. treatment |
decreased clotting factors- prolonged PT (prothrombin time)--liver uses vitamin K to synthesize clotting factors in this pathway (II, VII, IX, X). PTT may be prolonged in severe disease
- vitamin K is ineffective in treatment because it cannot be used by a diseased liver 2. treatment - fresh frozen plasma (FFP) |
|
|
signs of acute liver failure
|
- coagulopathy
- jaundice - hypoglycemia (liver stores glycogen) - hepatic encephalopathy - infection - elevated LFTs - any complication associated with cirrhosis |
|
|
What should you look for in diagnosing SBP?
|
- fever and change in mental status in a patient with ascites
- if not treated early the mortality is high- so always be suspicious in a patient with ascites and do the diagnostic paracentesis early |
|
|
Wilson's disease
- deficiency of what? - inheritance pattern? - build up of? - when diagnosed typically? |

1. autosomal recessive disease of copper metabolism
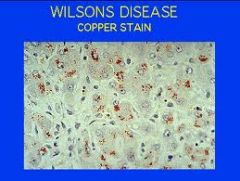
- normally excess copper is excreted by the liver, but the liver of patients with wilson's disease cannot do so because there is usually a deficiency in ceruloplasmin- a copper biding protein necessary for copper excretion - copper accumulates in hepatocytes causing them to die - copper leaks into plasma and accumulates in other organ including kidney, cornea and brain - most often apparent during childhood/adolescence (after age 5) and the majority of cases is present between 5 to 35 -- picture is of a Kayser-Fleischer ring-- build up of copper in the cornea- -does not interfere with vision - also known as hepatolenticular disease as it effects the liver and brain |
|
|
Clinical features of Wilson's disease
|

1. liver disease (most common initial manifestation)- varies but may include acute hepatitis, cirrhosis, and/or fulminant liver failure
2. Kayser-Fleisher rings- yellowish rings in the cornea caused by copper deposition-- does not interfere with vision 3. CNS findings-- extrapyramidal signs (EPS)- parkinsonian symptoms (resting tremor, rigidity, bradykinesia), chorea, drooling, incoordination due to copper deposition in the basal ganglia - psychiatric disturbances-- depression, neuroses, personality changes, psychosis 4. Renal involvement- aminoaciduria, nephrocalcinosis |
|
|
Diagnosis of Wilson's disease
|
1. hepatic disease- elevated LFTs, impaired synthesis of clotting factors and albumin
2. decreased ceruloplasmin levels-- although levels within the normal range do not exclude the diagnosis 3. liver biopsy- inc copper conc 4. if diagnosed first degree relatives must be screened |
|
|
Treatment of Wilson's disease
|
1. Chelating agents - D-penicillamine- removes and detoxifies the excess copper deposits
2. Zinc - prevents uptake of dietary copper. Given alone to presymptomatic or pregnant patients or in conjuction with chelating agents in symptomatic patients 3. Liver transplantation - if unresponsive to therapy or fulminant liver failure 4. monitor patient's copper levels, urinary copper excretion, ceruloplasmin, and liver function- physical examination for signs of liver or neurologic disease, psych health |
|
|
Hemochromatosis
1. cause 2. involved organs 3. secondary hemochromatosis |

1. autosomal recessive disease of iron absorption
- excessive iron absorption in the intestine leads to accumulation of iron (as ferritin and hemosiderin) in various organs. Over many years, fibrosis in the involved organs occurs secondary to hydoxyl free radicals that are generated by excess iron 2. affected organs -- liver (primary organ) , pancreas, heart, skin, joints, thyroid, gonads, hypothalamus - secondary hemochromatosis can also occur with multiple transfusions or in chronic hemolytic anemias |
|
|
Hepatocellular Adenoma
1. definition 2. risk factors 3. symptoms 4. malignant potential 5. Diagnosis 6. Treatment |
Benign liver tumor- most often seen in young women (15-40 years of age)
2. Risk factors include OCP use, female sex, and anabolic steroid use 3. May be asymptomatic or can have RUQ pain and fullness 4. Malignant potential is low (<1%), however the adenoma may rupture- leading to hemoperitoneum and hemorrhage 5. Dx by CT scan, US, hepatic arteriography (most accurate but invasive) 6. Treatment- discontinue OCPs. surgically resect tumors >5cm that do not regress after stopping OCPs due to risk of rupture |
|
|
Cavernous Hemangiomas
1. definition 2. symptoms 3. complications 4. diagnosis 5. treatment |

1. vascular tumors that are usually small and asymptomatic. Most common type of benign liver tumor.
2. As the size of the tumor increases (e.g. due to pregnancy or OCP use) the sx increase and may include RUQ pain and mass 3. Complications are uncommon unless the tumor is very large and may include rupture with hemorrhage, obstructive jaundice, coagulopathy, CHF secondary to large AV shunt and gastric outlet obstruction 4. Diagnose with US or CT with contrast. Biopsy is C/I due to risk of rupture 5. Most cases do not require treatment |
|
|
Focal Nodular Hyperplasia
1. definition 2. symptoms 3. Treatment |

1. benign liver tumor without malignant potential that occurs in women of reproductive age. No association with OCPs!!
2. Usually asymptomatic although hepatomegaly may be present. 3. Treatment not necessary in most cases |
|
|
3 types of benign liver tumors
|
1. Hepatocellular Adenoma
2. Cavernous Hemangioma 3. Focal Nodular Hyperplasia |
|
|
Hepatocellular Carcinoma
1. prevalence& where is it common 2. 2 pathologic types |
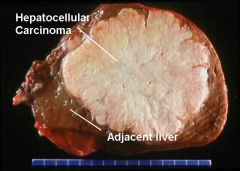
1. HCC - 80% of primary liver cancers-- common in Africa and Asia although rare in U.S.
2. Nonfibrolamellar (most common) - assoc with Hep B, C amd cirrhosis- usually unresectable and with a very short survival time (months) - fibrolamellar- usually not assoc with hep b,c or cirrhosis- usually resectable with a longer survival time- most common in adolescents and you adults |
|
|
Risk factors for hepatocellular carcinoma
|
1. Cirrhosis- especially in association with alcohol or hepatitis B or C- HCC develops in 10% of cirrhotic patient
2. chemical carcinogens- aflatoxin, vinyl chloride, thorotrast 3. Alpha-1-antitrypsin (AAT) deficiency 4. Hemachromatosis, Wilson's disease 5. Schitosomiasis 6. Hepatic ademona (10% risk of malignant transformation) 7. cigarette smoking 8. glycogen storage disease (type 1) |
|
|
Clinical features of hepatocellular carcinoma
|
1. abdominal pain (painful hepatomegaly)
2. weight loss, anorexia, fatigue 3. signs and symptoms of chronic liver disease- portal HTN, ascites, jaundice 4. paraneoplastic syndromes- erythrocytosis, thrombocytosis, hypercalcemia, carcinoid syndrome, hypertrophic pulmonary osteodystrophy, hypoglycemia, high cholesterol |
|
|
Diagnosis of Hepatocellular Carcinoma
|
1. Liver biopsy- required for definitive diagnosis
2. lab tests- hep B and C serology, LFTs, coags 3. Imaging studies- US, CT chest, abd, pelvis, MRI or MRI if surgery is an option 4. tumor marker elevation- AFP (alpha fetaprotein) is a useful screen tool as AFP may be elevated in 40-70% of patients with HCC- also helps monitor response to therapy |
|
|
Treatment and prognosis of Hepatocellular Carcinoma (HCC)
|
1. Liver resection (in 10% of patients who have resectable tumors)- liver regenerates
2. Liver transplant if diagnosis is made early Prognosis- If unresectable- less than 1 year, if resectable then 25% of patients are alive at 5 years |
|
|
What should you suspect in patients with cirrhosis and a palpable liver mass + inc AFP?
|
hepatocellular carcinoma
|
|
|
Nonalcoholic Steatohepatitis (NASH)
1. definition 2. associations 3. symptoms 4. how discovered? 5. treatment |
1. histology of the liver is identical to that in patients with alcoholic liver disease but these patients do not have a history of alcohol disease
2. associated with obesity, hyperlipidemia, diabetes mellitus 3. usually asymptomatic with a benign course (but cirrhosis develops in 10-15%) 4. Typically discovered on routine laboratory tests (mild elevation in ALT and AST) 5. No clearly established treatment |
|
|
Gilbert's syndrome
1. what is it? 2. what lab test is abn? 3. what are exacerbating factors? 4. how usually discovered/symptoms 5. treatment |
1. occurs in up to 7% of the population - autosomal dominant condition in which there is decreased activity of hepatic UGT)
2. common cause of isolated elevation of unconjugated bilirubin 3. exacerbated by fasting (crash diets), fever, alcohol, and infection 4. asymptomatic in most cases but occasionally mild jaundice maybe present 5. liver biopsy results are normal and usually no treatment is necessary |
|
|
Hemobilia
1. definition 2. causes 3. clinical features 4. diagnosis 5. treatment |
1. blood draining into the duodenum via the common bile duct- source of bleeding can be anywhere along the biliary tract, the liver or the ampullary region
2. causes- trauma (most common), papillary thyroid carcinoma, surgery (cholecystectomy), CBD exploration, tumors, infection 3. GI bleeding (melena, hematemesis), jaundice, and RUQ pain 4. Arteriogram is diagnostic- Upper GI endoscopy shows blood coming out of the ampulla of vater 5. treatment- resuscitation (may require transfusion)- if bleeding is severe, surgery is necessary (options include ligation of hepatic arteries, or arteriogram with embolization of vessels) |
|
|
Polycystic Liver Cysts
1. cause/inheritance 2. symptoms 3. treatment |
1. autosomal dominant- usually associated with polycystic kidney disease. PCKD often results in renal failure and is the main determinant of prognosis whereas liver cysts rarely lead to hepatic fibrosis and liver failure
2. usually asymptomatic, although some patients have abd pain and upper abd mass 3. treatment is usually not needed |
|
|
Hydatid Liver Cysts
1. cause 2. symptoms 3. treatment |
1. caused by infection from the tapeworm, Echinococcus granulosus. Cysts most commonly occur in the right lobe of the liver
2. small cysts are asymptomatic, larger cysts may cause RUQ pain and rupture into the peritoneal cavity causing fatal anaphylactic shock 3. Treatment- surgical resection (caution to avoid spilling cyst contents into peritoneal cavity). Give mebendazole after surgery |
|
|
Pyogenic Liver Abscess
1. most common cause 2. causative organisms 3. clinical features 4. diagnosis 5. treatment |
1. most common cause is biliary tract obstruction- obstruction of bile flow allows bacterial proliferation. Other causes include GI infection (diverticulitis, appendicitis) with spread via portal venous system and penetrating liver trauma (GSW, surgery)
2. Causative organisms include E. coli, Klebsiella, enteroccus, and anaerobes 3. fever, malaise, anorexia, weight loss, nausea, vomiting, RUQ pain, and jaundice- patients appear quite ill 4. Diagnosed by ultrasound or CT scan, elevated LFTs 5. fatal if untreated. Treatment (IV antibiotics and percutaneous drainage of abscess) reduces mortality to about 5-20%. Surgical drainage is sometimes necessary |
|
|
Amebic liver abscess
1. who is it most common in? transmission? 2. cause? 3. symptoms 4. diagnosis 5. treatment |

1. Most common in men (9:1), particularly in homosexual men, transmitted through fecal-oral contact
2. caused by intestinal amebiasis (entamoeba histolytica)- the amoebea reach the liver via the hepatic portal vein 3. fever, RUQ pain, nausea/vomting, HSM, diarrhea 4. serological testing (IgG enzyme immunoassay) establishes diagnosis, LFTs are often elevated. The E. histolytica antigen test (detects protozoa in stool) - not sensitive. Imaging studies (US, CT) identify abscess, but it is difficult to distinguish from pyogenic abscess 4. IV metronidazole is effective treatment in most cases. Therapeutic aspiration of abscess may be necessary if the abscess is large (high risk of rupture) or there is no response to medical therapy |
|
|
Budd-Chiari Syndrome
1. definition 2. course 3. causes 4. clinical features 5. dx 6. tx |
1. Liver disease caused by occlusion of the hepatic venous outflow, which leads to hepatic congestion and subsequent microvascular trauma
2. course is variable, but most cases are indolent, with gradual development of portal HTN and progressive deterioration of liver function. Rarely disease is severe and leads to acute liver failure 3. causes- hypercoaguable states, myeloproliferative disorders (polycythemia vera), pregnancy, chronic inflammatory diseases, infection, various cancers, trauma. Idiopathic 40% 4. resemble those of cirrhosis- hepatomegaly, jaundice, ascites, abd pain, variceal bleeding 5. dx- hepatic venography, serum ascites albumin gradient > 1.1 g/dL 6. tx- medical tx is usually unsatisfactory (anticoagulation, thrombolytics, diuretics). Surgery is eventually needed in most cases (balloon angioplasty with stent placement in inferior vena cava, portocaval shunts). liver transplant if cirrhosis is present |
|
|
Jaundice
1. definition 2. when evident? at what level? 3. conjugated vs unconjugated bilirubin |
1. yellow coloration of skin, mucous membranes, and sclerae due to overproduction or underclearance of bilirubin
2. clinical jaundice usually becomes evident when total bilirubin is > 2 mg/dL 3. conjugated (direct) bilirubin- loosely bound to albumin and therefore water soluble- gets excreted in the urine causing it to look dark. Nontoxic. - unconjugated (indirect) bilirubin- tightly bound to albumin and therefore not water soluble and cannot be excreted in the urine even when blood levels are high. Toxic unbound form can cross the blood-brain barrier and cause neuro deficits |
|
|
Causes of conjugated hyperbilirubinemia
|
1. decreased intrahepatic excretion of bilirubin
- hepatocellular disease (viral or alcoholic hepatitis, cirrhosis) - inherited disorders (Dubin-Johnson syndrome, Rotor's syndrome) - drug induced (OCPs) - Primary biliary cirrhosis (PBC) - primary sclerosis cholangitis (PSC) 2. extrahepatic biliary obstruction - gallstones - carcinoma in the head of the pancreas - cholangiocarcinoma - periampullary tumors - extrahepatic biliary atresia - |
|
|
Causes of unconjugated hyperbilirubinemia
|
1. Excess production of bilirubin- hemolytic anemias
2. Reduced hepatic uptake of bilirubin or impaired conjugation - Gilbert's syndrome - drugs - (sulfonamides, penicillin, rifampin, radiocontrast agents) - Crigler Najjar syndrome type I and type II - physiologic jaundice of the newborn- immaturity of conjugating system - diffuse liver disease (hepatitis, cirrhosis) |
|
|
Diagnosis and treatment of hyperbilirubinemia
|
1. serum levels of conjugated and unconjugated bilirubin
2. if unconjugated hyperbilirubinemia - check a CBC, reticulocyte count, hemoglobin, LDH, and peripheral smear (may aid in the diagnosis of hemolysis as the cause of jaundice) 3. if conjugated hyperbilirubinemia-- LFTs may point to the cause 4. US or CT to assess biliary tract for obstruction or anatomic changes 5. additional tests (Endoscopic Retrograde Cholangiopancreatography - ERCP) or percutaneous transhepatic cholangiography- depending on findings of above 6. liver biopsy may be indicated in some cases to determine cause of injury -treatment- treat the underlying cause. May want to give cholestyramine- bile acid sequestrant |
|
|
Liver Function Tests
1. what are they? What is most sensitive and specific for liver disease? 2. what indicates alcohol as a cause? 3. mild elevation indicates? 4. moderate elevation indicates? 5. severe elevation indicates? 6. what if patient has cirrhosis? |
1. Aminotransferases - ALT and AST
- ALT is more sensitive and specific than AST for liver damage 2. ALT and AST usually have a similar increase with the exception being alcoholic hepatitis - in which the AST-ALT ratio may be > 2:1 3. if ALT and AST levels are mildly elevated (low hundred) think of chronic viral hepatitis or acute alcoholic hepatitis 4. If ALT and AST are moderately elevated (high hundreds to 1000s) - think of acute viral hepatitis 5. if ALT and AST are severely elevated (>10,000) - extensive hepatic necrosis has occurred. Typical causes include- ischemia, shock liver (prolonged hypotension or circulatory collapse), acetaminophen toxicity, severe viral hepatitis 6. NOTE: liver transaminases are often normal or even low in patients with cirrhosis (without any active cell necrosis) or metastatic liver disease because the number of functioning hepatocytes is markedly reduced |
|
|
What are potential causes of elevated ALT and AST?
|
A- Autoimmune hepatitis
B- hepatitis B C- hepatitis C D- drugs or toxins E- Ethanol F- fatty liver (hypertriglyceridemia) G- growths (tumors) H- hemodynamic disorders (e.g. CHF) I- Iron- hemochromatosis, Copper (wilson's disease) or AAT deficiency |
|
|
Alkaline Phosphatase (ALK-P)
1. what does it measure? 2. what if levels are very high (10 fold increase)? 3. What should you also measure with this? |
- Not specific to liver- also found in bone, gut, and placenta
1. ALK-Phos is elevated when there is an obstruction of bile flow (e.g. cholestasis) in any part of the biliary tree. Normal levels make cholestasis unlikely 2. If levels are very high (10-fold increase), think of extrahepatic biliary tract obstruction or intrahepatic cholestasis (e.g. PBC or drug induced cirrhosis) 3. If levels are elevated, measure GGT (gamma-glutamyl-transferase) level to make sure the elevation is hepatic in origin (rather than bone or intestinal). If the GGT is also elevated, this strongly suggests a hepatic origin. If the GGT level is normal, but ALK-P is elevated, consider pregnancy or bone disease |
|
|
What can cause a decreased albumin level?
|
- chronic liver disease
- nephrotic syndrome - malnutrition - inflammatory states (burns, sepsis, trauma) |
|
|
Prothrombin time (PT)
|
The liver synthesizes clotting factors I, II, V, VII, IX, X, XII and XIII-- the function of which is reflected by PT
- PT is not prolonged until most of the liver's synthetic capacity is lost- which corresponds to advanced liver disease |
|
|
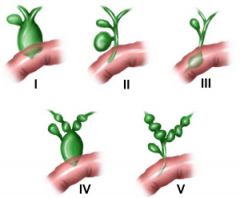
Cholelithiasis
1. definition 2. 3 types |
1. refers to stones in the gallbladder (gallstones)
2. There are 3 types of stones - a. cholesterol stones (yellow to green)- associated with: obesity, diabetes, and hyperlipidemia, multiple pregnancies, OCPs, Crohn's disease, ileal resection, advanced age, Native American ancestry, cirrhosis, cystic fibrosis b. Pigment stones- black stones are usually found in the gallbladder and are associated with either hemolysis (e.g. sickle cell disease, thalassemia, hereditary spherocytosis, artificial cardiac valves) or alcoholic cirrhosis. - brown stones are usually found in the bile ducts and are associated with biliary tract infections c. Mixed stones have components of both cholesterol and pigment stones and account for the majority of stones |
|
|
Clinical features of cholelithiasis
|
- most cases are asymptomatic. Majority of patients found to have incidental gallstones will remain asymptomatic.
- biliary colic is the cardinal symptom of gallstones and is due to temporary obstruction of the cystic duct by a gallstone. Pain occurs as the gallbladder contracts against this obstruction. - pain is typically located in the RUQ or epigastrium and may be mild, moderate, or severe - patients classically report pain after eating and at night - Boas' sign - referred right scapular pain of biliary colic |
|
|
Diagnosis of cholelithiasis
|

1. RUQ ultrasound has high sensitivity and specificity (>95%) for stones > 2 mm.
2. CT and MRI are alternatives |
|
|
Treatment of cholelithiasis
|
1. No treatment if the patient is asymptomatic
2. Elective cholecystectomy for patients with recurrent bouts of biliary colic |
|
|
Complications of cholelithiasis
|
1. cholecystitis (chronic or acute) with prolonged obstruction of cystic duct
2. choledocholithiasis with its associated complications 3. gallstone ileus- lack of peristalsis 4. malignancy |
|
|
What fraction of patients with biliary colic will develop acute cholecystitis within 2 years?
|
1/3
|
|
|
What causes the pain in acute cholecystitis? biliary colic?
|
Pain in acute cholecystitis is secondary to gallbladder wall inflammation, whereas the pain of biliary colic is secondary to contraction of the gallbladder against an obstructed cystic duct. The pain of acute cholecystitis persists for several days, whereas the pain of biliary colic lasts only a few hours.
|
|
|
Acute cholecystitis
1. definition/cause 2. chronic cholecystitis? 3. what percent of patients with gallstones will develop this? |
1. obstruction of the cystic duct (not infection) induces acute inflammaion of the gallbladder wall
2. chronic cholecystitis may develop with recurrent bouts of acute cholecystitis 3. 10% of patients with gallstones will develop acute cholecystitis |
|
|
Symptoms of acute cholecystitis?
|
- pain is always present and is located in RUQ or epigastrium. It may radiate to the right shoulder or scapula
- nausea and vomiting, anorexia |
|
|
Signs of acute cholecystitis on exam?
|
- RUQ tenderness, rebound tenderness in RUQ
- Murphy's sign is pathognomonic- inspiratory arrest during deep palpation of the RUQ, not present in many cases (if this happens with US-- it is called a sonographic Murphy's) - Hypoactive bowel sounds - low-grade fever, leukocytosis |
|
|
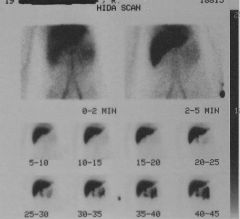
Diagnosis of acute cholecystitis?
|

1. RUQ ultrasound is the test of choice- high sensitivity and specificity. Findings include thickened gallbladder wall and pericholecystic fluid, distended gallbladder, and presence of stone(s)
2. CT scan is as accurate as ultrasound but is more sensitive in identifying complications of acute cholecystitis such as perforation, abscess and pancreatitis 3. Radionucleotide scan (hepatoiminodiacetic acid- HIDA) - used when US is inconclusive. Its sensitivity and specificity parallel that of US. If HIDA is normal, acute cholecystitis can be ruled out. - A positive HIDA scan means the gallbladder is not visualized - If gallbladder is not visualized 4 hours after injection, diagnosis of acute cholecystitis is confirmed |
|
|
Treatment of acute cholecystitis
|
1. patient should be admitted. Conservative measures include hydration with IV fluids, bowel rest (NPO), IV antibiotics, analgesics and correction of any electrolyte abnormalities
2. surgery- cholecystectomy is indicated in most patients with symptomatic gallstones. Early cholecystectomy is preferred (first 24 to 48 hours). Recurrence rate with nonsurgical treatment is as high as 70%. Timing of surgery depends on the severity of the symptoms and patients risk assessment for surgery, but in most patients, early cholecystectomy is preferred. |
|
|
Acalculous Cholecystitis
1. what is it? 2. cause/associations? 3. signs and symptoms? 4. diagnosis 5. treatment |
1. Acute cholecystitis without stones obstructing the cystic duct (up to 10% of the patients with acute cholecystitis)
2. usually idiopathic and seen in patients with severe underlying illness; possible association with dehydration, ischemia, burns, severe trauma, and post-operative state 3. signs and symptoms are the same as acute cholecystitis 4. diagnosis may be difficult because patients with this condition are often severely ill and have other medical problems, so clinical features are less apparent 5. emergent cholecystectomy is the treatment of choice. For patients who are too ill for surgery, perform percutaneous drainage of the gallbladder with cholecystostomy |
|
|
Choledocholithiasis
1. definition 2. primary vs secondary stones? |

1. gallstones in the common bile duct (CBD)
2. primary versus secondary stones. Primary stones originate in the CBD (usually pigmented stones), Secondary stones originate in the gallbladder and then pass into the CBD (usually cholesterol or mixed stones). - 95% of CBD stones are secondary |
|
|
Clinical features of choledocholithiasis
|
1. patients may be asymptomatic for years
2. symptoms when present include RUQ pain or epigastric pain and jaundice |
|
|
Diagnosis of choledocholithiasis
|
1. laboratory tests- total and direct bilirubin levels are elevated as well as alk-phos
2. RUQ US is usually the initial study, but is not a sensitive study for choledocholithiasis. It detects CBD stones in only 50% of the cases, so it cannot be used to rule out the diagnosis. 3. ERCP (endoscopic retrograde cholangiopancreatography) is the gold standard (sensitivity and specificity is 95%) and should follow US. ERCP is diagnostic and therapeutic. 4. PTC (percutaneous transhepatic cholangiography) is an alternative to ERCP |
|
|
Treatment of choledocholithiasis
|
1. ERCP with sphincterotomy and stone extraction with stent placement (successful in 90% of patients)
2. laparoscopic choledocholithotomy (in select cases) |
|
|
Cholangitis
1. definition and causes 2. treatment |
1. infection of the biliary tract secondary to obstruction, which leads to biliary stasis and bacterial overgrowth
- choledocholithiasis accounts for 60% of cases - other causes include pancreatic and biliary neoplasm, postoperative strictures, invasive procedures such as ERCP or PTC and choledochal cysts 2. cholangitis is a potentially life-threatening illness and requires emergency treatment |
|
|
Clinical features of cholangitis
|
1. Charcot's triad- RUQ pain, jaundice and fever-- this classic triad is present in only 50-70% of cases
2. Reynold's pentad- charcot's triad plus septic shock and altered mental status (CNS depression-- e.g. coma, disorientation) 3. patient is acutely ill, and abdominal symptoms may be lacking or may go unrecognized |
|
|
Diagnosis of cholangitis
1. initial study 2. lab findings 3. cholangiography options (2)- when would you choose each? |
1. RUQ ultrasound is the initial study
2. laboratory findings- hyperbilirubinemia, leukocytosis, mild elevation in serum transaminases 3. cholangiography (either PTC or ERCP) - this is the definitive test, but it should not be performed during the acute phase of the illness. - Once cholangitis resolves, proceed with PTC or ERCP to identify the underlying problem and plan treatment - perform PTC when the duct system is dilated (per US) and ERCP when the duct system is normal |
|
|
Treatment of cholangitis
|
1. IV antibiotics and IV Fluids
- close monitoring of hemodynamics, BP, urine output (UOP), 2. Most patients respond rapidly. Once the patient has been afebrile for 48 hours then proceed with cholangiography (PTC or ERCO) for evaluation of the underlying condition 3. decompress the CBP via PTC (catheter drainage), ERCP (sphincterotomy) or laparotomy (T-tube insertion) once the patient is stabilized, or emergently if the condition does not respond to antibiotics |
|
|
Carcinoma of the gallbladder
1. what type are they most often and who do they occur in? 2. associations/ risk factors 3. clinical features 4. treatment 5. prognosis |
1. most are adenocarcinomas. Typically occur in the elderly
2. associated with gallstones in most cases, other risk factors include cholecystoenteric fistula and porcelain gallbladder 3. Clinical features are non-specific and suggest extrahepatic bile duct obstruction: jaundice, biliary colic, weight loss, anorexia, and RUQ mass. Palpable gallbladder is a sign of advanced disease. 4. difficult to remove with surgery: cholecystectomy versus radical cholecystectomy (with wedge resection of liver and lymph node dissection) depending on the depth of invasion 5. prognosis is dismal - more than 90% of patients die of advanced disease within 1 year of diagnosis. Disease often goes undetected until it is advanced. |
|
|
Primary Sclerosing Cholangitis (PSC)
1. definition/general characteristics 2. associations |
1. a chronic idiopathic progressive disease of intrahepatic and/or extrahepatic bile ducts characterized by thickening of the bile duct walls and narrowing of their lumens, leading to cirrhosis, portal hypertension and liver failure
2. their is a strong association with ulcerative colitis (less so with Crohn's disease). UC is present in 50-70% with PSC, often the UC may dominate the clinical picture. (NOTE- the course of PSC is unaffected by colectomy done for UC) |
|
|
Clinical features of primary sclerosing cholangitis (PSC)
|
- signs and symptoms begin insidiously
- chronic cholestasis findings, including jaundice and pruritis; all patients eventually present with chronic obstructive jaundice - other symptoms: fatigue, malaise and weight loss |
|
|
Diagnosis of primary sclerosing cholangitis
|

1. ERCP and PTC are diagnostic studies of choice- see multiple area of bead-like stricturing and dilations of the intrahepatic and extrahepatic ducts
2. laboratory tests show cholestatic LFTS- inc LFTs plus inc direct bili, plus inc alk-phos |
|
|
treatment of primary sclerosing cholangitis
|
1. there is no curative treatment other than liver transplantation
2. when a dominant stricture causes cholestasis, ERCP with stent placement for biliary drainage and bile duct dilitation may relieve symptoms 3. use cholestyramine for symptomatic relief (to decrease pruritis) - bile acid sequestant that binds to it and prevents it from being reabsorped. The insoluble compound is then excreted in the feces |
|
|
Primary Biliary Cirrhosis (PBC)
1. definition - what is affected? 2. course? 3. cause? 4. who is most often affected? |
1. chronic and progressive cholestatic liver disease characterized by destruction of the intrahepatic bile ducts with portal inflammation and scarring
2. it is a slowly progressive disease with a variable course. It may progress to cirrhosis and end-stage liver failure 3. It is an autoimmune disease that is often associated with other autoimmune disorders 4. most common in middle-aged women |
|
|
Clinical features of primary biliary cirrhosis (PBC)
|

1. fatigue
2. pruritus (early in the course of the disease) 3. jaundice (late in the course) 4. RUQ discomfort 5. xanthoma and xanthalesmata (cholesterol deposits) 6. osteoporosis 7. portal HTN (with resultant sequelae) |
|
|
Diagnosis of Primary Biliary Cirrhosis (PBC)
1. labs 2. biopsy findings 3. Imaging |
1. labs- cholestatic LFTs (inc alk phos)
2. positive anti-mitochondrial antibodies (AMAs) found in 90% to 95% of patients. This is the hallmark of the disease (specificity of 98%). If serum is positive for AMAs, perform a liver biopsy to confirm diagnosis 3. abd US or CT scan to rule out biliary obstruction |
|
|
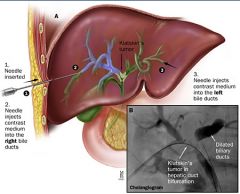
Cholangiocarcinoma
1. definition 2. mean age of diagnosis? 3. 3 regions affected- what is most common? 4. prognosis 5. risk factors |
1. tumor of the intrahepatic and extrahepatic bile ducts: most are adenocarcinomas
2. mean age of diagnosis is in the 7th decade 3. Located in three regions: proximal third of the CBD (most common, also called Klatskin's tumor), distal extrahepatic (best change of resectability), intrahepatic (least common) 4. prognosis is dismal- survival is less than 1 year after diagnosis 5. risk factors - ulcerative colitis, choledochal cysts, clonorchis sinesis (Chinese liver fluke) - hong kong |
|
|
Clinical features of cholangiocarcinoma
|
1. obstructive jaundice and associated symptoms (dark urine, clay-colored/acholic stools) and pruritis
2. weight loss |
|
|
Diagnosis of cholangiocarcinoma
|
1. cholangiography (PTC or ERCP)- for diagnosis and assessment of resectability
2. If the patient has an unresectable tumor (more likely the case with proximal than distal bile duct tumors), stent placement is an option during either PTC or ERCP and may relieve biliary obstruction |
|
|
Treatment of cholangiocarcinoma
|
1. most patients do have resectable tumors at the time of diagnosis
2. the survival rate is low despite aggressive chemotherapy, stenting or biliary drainage |
|
|
Choledochal cysts
1. definition and who is most likely to be affected? 2. clinical features? 3. complications 4. diagnosis 5. treatment |
1. cystic dilations of biliary tree involving either the extrahepatic or intrahepatic ducts or both-- more common in women (4:1)
2. clinical features: epigastric pain, jaundice, fever, and RUQ mass 3. Complications - cholangiocarcinoma (most feared complication- risk is about 20% over 20 years), hepatic abscess, recurrent cholangitis/pancreatitis, rupture, biliary obstruction, cirrhosis, and portal HTN 4. US is the best non-invasive test and ERCP is definitive for diagnosis 5. Treatment is surgery: complete resection of the cyst with biliary-enteric anastomosis to restore continuity of biliary system with the bowels |
|
|
Bile Duct Stricture
1. causes-- what is most common? 2. clinical features? 3. complications? 4. treatment |
1. most common cause is iatrogenic injury (prior biliary surgery such as cholecystectomy, liver transplantation), other causes include recurring choledocholithiasis, chronic pancreatitis, and primary sclerosing cholangitis (PSC)
2. clinical features are those of obstructive jaundice 3. complications can be life-threatening and include- secondary biliary cirrhosis, liver abscess, and ascending cholangitis 4. treatment involves endoscopic stenting (preferred) or surgical bypass if obstruction is complete or if endoscopic therapy fails |
|
|
Biliary dyskinesia
|
1. motor dysfunction of the spincter of Oddi, which leads to recurrent episodes of biliary colic without any evidence of gallstones on diagnostic studies such as US, CT, and ERCP
2. Diagnosis is made by HIDA scan (once the gallbladder is filled with labeled radionucleotide, give cholecystokinin (CCK) intravenously, then determine the EF of the gallbladder. If the EF is low, dyskinesia is likely. 3. Treatment options - laparoscopic cholecystectomy, endoscopic sphincterotomy |
|
|
1. Pathogenesis of appendicitis
2. peak age of incidence |
a. The lumen of the appendix is obstructed by hyperplasia of lymphoid tissue (60% of cases), a fecalith (35% of cases), a foreign body, or other rare causes (parasite or carcinoid tumor)- 5% of cases
b. obstruction leads to stasis (of fluid and mucus), which promotes bacterial overgrowth leading to inflammation c. distention of the appendix can compromise blood supply. The resulting ischemia can lead to infarction or necrosis if untreated. Necrosis can result in appendiceal perforation and ultimately peritonitis 2. peak incidence is in the teens to mid-20s. Prognosis is far worse in infants and elderly patients (high rate of perforation) |
|
|
Symptoms of acute appendicitis
|
1. Abdominal pain- classically starts in the epigastrium as ill-defined pain, moves toward umbilicus, and then to RLQ. with distention of the appendix, the parietal peritoneum may become irritate, leading to sharp pain
2. anorexia always present. Appendicitis is unlikely if the patient is hungry 3. nausea and vomiting (typically follow pain) |
|
|
Signs of acute appendicitis
|

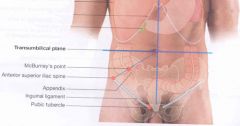
1. tenderness in RLQ (maximal tenderness at McBurney's point- 2/3 of the distance from the umbilicus to the right anterior superior iliac spine)
2. rebound tenderness, guarding, diminished bowel sounds 3. low grade fever (may spike if perforation is present) 4. Rovsing's sign- deep palpation in the LLQ causes referred pain in the RLQ 5. Psoas sign- RLQ pain when right thigh is extended as patient lies on left side 6. Obturator sign- pain in the RLQ when flexed right thigh is internally rotated when patient is supine |
|
|
Diagnosis of acute appendicitis
|

** Acute appendicitis is a clinical diagnosis. Laboratory findings (mild leukocytosis) are only supportive. Radiographs or other imaging studies re unnecessary unless the diagnosis is uncertain or the presentation is atypical
- CT scan (sensitivity of 98% to 100%)-- lowers the false positive rate significantly - ultrasound (sensitivity of 90%) |
|
|
Treatment of acute appendicitis
- risk of false positive? |
-appendectomy (usually laparoscopic)
- up to 20% of patients who are diagnosed with acute appendicitis are found to have a normal appendix during surgery. Because the illness is potentially life-threatening, this is an acceptable risk EVEN DURING PREGNANCY |
|
|
Carcinoid tumors and carcinoid syndrome
- origination and secretion? - most common site? |
1. carcinoid tumors originate from neuroendocrine cells and secrete serotonin
2. the most common site for these tumors is in the appendix, but they can be found in a variety of locations (small bowel, rectum, bronchus, kidney and pancreas) |
|
|
Pathogenesis of acute pancreatitis
|
1. Inflammation of the pancreas resulting from prematurely activated pancreatic digestive enzymes that invoke pancreatic tissue autodigestion
|
|
|
2 forms of acute pancreatitis
|
1. Mild - (75% have mild to moderate) - responds well to supportive treatment
2. severe (up to 25%)- necrotizing pancreatitis- significant morbidity and mortality |
|
|
Causes of acute pancreatitis
|
1. alcohol abuse (40%)
2. Gallstones (40%) - the gallstone passes into the bile duct and blocks the ampulla of vater (where bile enters the duodenum) 3. post ERCP- pancreatitis occurs in up to 10% of patients undergoing ERCP 4. viral infections- mumps, Coxackie virus B 5. drugs - sulfonamides, thiazide diuretics, furosemide, estrogens, HIV meds etc 6. post-operative complication (high mortality rate) 7. scorpion bites 8. pancreas divisum (controversial)- congenital problem 9. pancreatic cancer 10. hypertriglyceridemia, hypercalcemia 11. uremia 12. blunt abdominal trauma - most common cause of pancreatitis in young children (IGETSMASHED pneumonic) |
|
|
Symptoms of acute pancreatitis
|
1. abdominal pain, usually in the epigastric region-- may radiate to the back (50% of patients)
- often steady, dull, and severe, worse when supine and after meals 2. nausea and vomiting, anorexia |
|
|
Signs of acute pancreatitis
|

1. low grade fever, tachycardia, hypotension, leukocytosis
2. epigastric tenderness, abdominal distention 3. decreased or absent bowel sounds indicate partial ileus 4. the following signs are seen with hemorrhagic pancreatitis as blood tracks along fascial planes - grey turner's sign- flank ecchymoses - cullen's sign- periumbilical ecchymoses (pictured) - fox's sign- ecchymosis of the umbilical ligament |
|
|
Diagnosis of pancreatitis - Labs
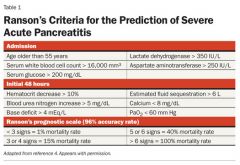
1. What labs should you order? What is most specific for acute pancreatitis? 2. prognostic predictors |
1. Lab tests
- serum amylase is the most common test- but many conditions cause hyperamalasemia (non-specific) and its absence does not rule out acute pancreatitis (non-sensitive) However, if levels are more than 5 times the upper limit of normal, there is a high specificity for acute pancreatitis -- serum lipase - more specific for pancreatitis than amylase 2. LFTs - to identify cause (gallstone pancreatitis) - inc Alk phos 3. hyperglycemia, hypoxemia, and leukocytosis may also be present 4. Order the following to assess for prognosis (ranson's criteria) -- glucose, calcium, hematocrit, BUN, arterial blood gas (PaO2, base deficit), LDH, AST, WBC count |
|
|
Why does hypocalcemia occur in acute pancreatitis?
|
Due to fat saponification - fat necrosis binds calcium
|
|
|
Diagnosis of acute pancreatitis - Imaging
|
1. Abdominal xray- limited role in the diagnosis of acute pancreatitis
- more helpful in ruling out other diagnosis- such as intestinal perforation (free air). The presence of calcifications can suggest chronic pancreatitis. - In some cases, one may see a sentinel loop (area of air-filled bowel usually in the LUQ, which is a sign of localized ileus) or colon cutoff sign (air-filled segment of the transverse colon abruptly ending or "cutting off" at the region of pancreatic inflammation 2. abdominal ultrasound- can help in identifying cause of pancreatitis - gallstone. Useful for following up pseudocysts or abscesses 3. CT scan of the abdomen- most accurate test for the diagnosis of acute pancreatitis and for identifying complications of the disease - indicated in patients with severe acute pancreatitis 4. ERCP indications - severe gallstone pancreatitis with biliary obstruction, to identify uncommon causes of acute pancreatitis if disease is recurrent |
|
|
Complications of acute pancreatitis
|
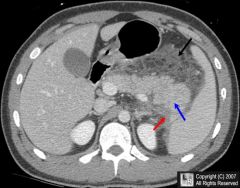
1. Pancreatic necrosis (may be sterile or infected)
- sterile pancreatic necrosis - infection may develop, but half of all cases resolve spontaneously. These patients should be monitored closely in an ICU. Prophylactic antibiotics is controversial but if necrosis involves more than 30% of pancreas, antibiotics should be strongly considered - infected pancreatic necrosis - high mortality rate (results in multiple organ failure in 50% of cases), surgical debridement and antibiotics indicated - the only way to distinguish sterile from infected necrosis is via CT-guided percutaneous aspiration with gram stain/culture of the aspirate 2. pancreatic pseudocyst- encapsulated fluid collection that appears 2 to 3 weeks after an acute attack-- unlike a true cyst, it lacks an epithelial lining - complications of untreated pseudocysts include rupture, infection, gastric outlet obstruction, fistula, hemorrhage into cyst, and pancreatic ascites. It may impinge on adjacent abdominal organs (duodenum, stomach, transverse colon) if large enough or if located in the head of the pancreas- it may cause compression of the CBD - diagnosis by CT scan = study of choice - treatment - cysts > 5cm- drain either percutaneously or surgically, <5 cm - observation 3. hemorrhagic pancreatitis - characterized by cullen's sign, grey turner's sign, and fox's sign, CT Scan with IV contrast is the study of choice 4. Adult respiratory distress syndrome - a life-threatening complication with high mortality rate 5. pancreatic ascites/pleural effusion- the most common cause is inflammation of peritoneal surfaces 6. ascending cholangitis - due to gallstone in ampulla of vater, leading to infection of biliary tract 7. pancreatic abscess (rare) - develops over to 4-6 weeks and is less life-threatening than infected pancreatic necrosis |
|
|
pancreatic pseudocyst
1. what is it? 2. complications 3. diagnosis 4. treatment |
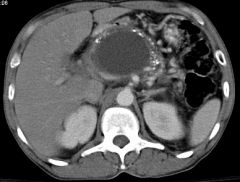
1. pancreatic pseudocyst- encapsulated fluid collection that appears 2 to 3 weeks after an acute attack-- unlike a true cyst, it lacks an epithelial lining
2. complications of untreated pseudocysts include rupture, infection, gastric outlet obstruction, fistula, hemorrhage into cyst, and pancreatic ascites. It may impinge on adjacent abdominal organs (duodenum, stomach, transverse colon) if large enough or if located in the head of the pancreas- it may cause compression of the CBD 3. diagnosis by CT scan = study of choice 4. treatment - cysts > 5cm- drain either percutaneously or surgically, <5 cm - observation |
|
|
Treatment of mild acute pancreatitis
|
mild pancreatitis treatment
- Bowel rest (NPO), - IV fluids - patients may have severe intravascular volume depletion. Correct electrolyte abnormalities - pain control - but be cautious in giving narcotics. Fentanyl and meperidine are preferred over morphine which causes an increase in sphincter of oddi pressure - NG tube if severe nausea/vomiting or ileus present, routine use is controversial |
|
|
Treatment of severe acute pancreatitis
|
If severe- patient should be admitted to the ICU. Early enteral nutrition in the first 72 hours is recommended through a nasojejunal tube.
- if the severe acute pancreatitis has not resolved in a few days, supplement parenteral nutrition should be started. - if more than 30% of the pancreas is necrosed, prophylactic antibiotics (imipenem) should be considered to prevent infection (which has high morbidity and mortality) |
|
|
Prognosis of acute pancreatitis
|
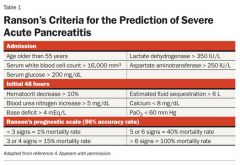
Ranson's criteria is used to determine prognosis and mortality rates
- patients with more than 3 or 4 of Ranson's criteria should be monitored in the ICU setting |
|
|
Chronic pancreatitis
1. definition 2. what is impaired? 3. causes? |
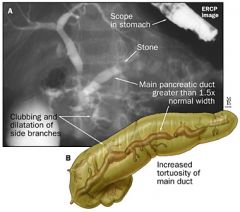
1. persistent or continuing inflammation of the pancreas, with fibrotic tissue replacing pancreatic parenchyma and alteration of pancreatic ducts (areas of stricture/dilation- "chain of lakes" appearance on ERCP)- eventually results in irreversible destruction of the pancreas
2. The endocrine and exocrine functions of the pancreas are impaired 3. Chronic alcoholism is the most common cause (>80% of cases). - other causes include hereditary pancreatitis, tropical pancreatitis, and idiopathic chronic pancreatitis |
|
|
Clinical features of chronic pancreatitis
|
1. severe pain in the epigastrium- recurrent or persistent abdominal pain
- often accompanied by nausea and vomiting - may be aggravated by a drinking episode or by eating - radiates to the back (in 50% of cases) 2. weight loss due to malabsorption, alcohol abuse and diabetes. Steatorrhea secondary to malabsorption |
|
|
Diagnosis of chronic pancreatitis
|
1. CT scan- the initial study of choice. It may show calcifications not seen on plain films. Mild to moderate cases may not be detectable, so a normal CT does not necessarily rule out chronic pancreatitis
2. abdominal radiograph- the presence of pancreatic calcifications is 95% specific, but is found in only 30% of cases 3. ERCP is the gold standard- but is not done routinely because it is invasive 4. laboratory studies are not helpful in the diagnosis. Serum amylase and lipase levels are not elevated in chronic pancreatitis |
|
|
Complications of chronic pancreatitis
|
1. narcotic addiction - probably the most common complication
2. diabetes mellitus/impaired glucose tolerance - caused by progressive loss of islets of langerhans - eventually appears in up to 70% of patients 3. Malabsorption/steatorrhea - caused by pancreatic exocrine insufficiency- occurs when pancreatic enzyme secretion decreases significantly - late manifestation of chronic pancreatitis 4. pseudocyst formation 5. pancreatic ductal dilation 6. CBD obstruction - may occur secondary to fibrosis in head of the gland 7. vitamin B12 malabsorption 8. effusions (e.g. pleural, pericardial, peritoneal) 9. pancreatic carcinoma - patients with chronic pancreatitis have an increased risk |
|
|
Treatment of chronic pancreatitis
|
1. Non-operative management
- narcotic analgesics for pain - bowel rest (NPO) - pancreatic enzymes and H2 blockers (give simultaneously) - pancreatic enzymes inhibit CCK release and thus decrease pancreatic secretions after meals. H2 blockers inhibit gastric acid secretion, preventing degradation of the pancreatic enzyme supplements by gastric acid - insulin - may be necessary due to severe pancreatic endocrine insufficiency - alcohol abstinence - frequent, small volume, low-fat meals- may improve abdominal pain 2. Surgery- main goal is relief of incapacitating abdominal pain - pancreaticojejunostomy- pancreatic duct drainage procedure to decompress dilated pancreatic duct- most common procedure - pancreatic resection - distal pancreatectomy, whipple's procedure |
|
|
Characteristics of pancreatic cancer
1. most common demographic affected 2. anatomic location 3. risk factors 4. prognosis |

1. most common in elderly patients (75% of patients are > 60 years old), rare before age 40- more common in African Americans
2. Anatomic location - a. pancreatic head (75% of cases), b. pancreatic body - 20% of cases, c. pancreatic tail - 5-10% of cases 3. Risk factors- cigarette smoking (most clearly establish risk), chronic pancreatitis, diabetes, heavy alcohol use, exposure to chemicals- benzidene and b-naphthylamine 4. the prognosis is dismal- most patients die within months of diagnosis |
|
|
Clinical features of pancreatic cancer
|

1. abdominal pain (90% of patients) - may be vague and dull ache
2. jaundice - most common with carcinoma of head of pancreas- less than 10% of patients with cancer involving body and tail of pancreas have jaundice. Indicated obstruction of intrapancreatic CBD and is a sign of advanced disease 3. weight loss (common due to decreased food intake and malabsorption), anorexia 4. recent onset of glucose intolerance, but the diabetes is mild 5. depression, weakness and fatigue 6. migratory thrombophlebitis- develops in 10% of patients 7. courvoisier's sign- palpable gallbladder = present in 30% of patients with cancer in the head of the pancreas, presents without pain ** The early clinical findings of pancreatic cancer are very vague and nonspecific. By the time a diagnosis is made, most patients have an incurable level of advanced disease |
|
|
painless jaundice and palpable gall bladder
|
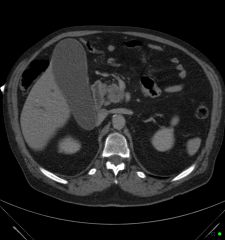
Courvoisier's sign - pancreatic carcinoma in the head of the pancreas (30%)
- however painless jaundice is not common in pancreatic cancer |
|
|
Diagnosis of pancreatic cancer
|
1. ERCP is the most sensitive test for diagnosing pancreatic cancer. It can also distinguish cancer of the head of the pancreas from tumors of the CBD, duodenum, ampulla, and lymphomas which have a more favorable prognosis
2. CT scan is the preferred test for diagnosis and assessment of disease spread 3. tumor markers - CA19-9 (sensitivity of 83% and specificity of 82%), CEA (sensitivity of 56% and specificity of 75%) |
|
|
Treatment of pancreatic cancer
|
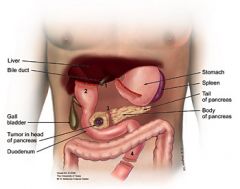
1. Surgical resection (whipple's procedure - pancreaticoduodectomy) is the only hope of cure-- however, only a minority of tumors are resectable (roughly 10%). The prognosis is grim even after resection, with a 5-year survival of 10%
2. If the tumor is unresectable and biliary obstruction is present, perform PTC (percutaneous cholangiopancreatography) or ERCP with stent placement across the obstruction for palliation |
|
|
Anatomic difference between upper and lower GI bleed -- where do you draw the line?
|

Upper GI bleeds occur above the ligament of Treitz in the duodenum, whereas lower GI bleeds occur below this point
|
|
|
Causes of upper GI bleeds
|
1. peptic ulcer disease (PUD)- duodenal ulcer (25% of cases), gastric ulcer (20% of cases), gastritis (25% of cases)
2. reflux esophagitis 3. esophageal varices (10% of cases) - venous bleeding 4. gastric varices 5. gastric erosions, duodenitis 6. Mallory-Weiss tear 7. hemobilia 8. dieulafoy's vascular malformation- submucosal dilated arterial lesions that can cause massive GI bleeding 9. aortoenteric fistula- after aortic surgery (ask about prior aortic aneurysm/graft)-- rare but lethal cause of GI bleeding 10. Neoplasm- bleeding is not rapid- usually not an emergency |
|
|
Causes of lower GI bleeds
|
1. diverticulosis (40% of cases)- most common source of GI bleeding in patients over age 60, usually painless
2. angiodysplasia- (40% of cases)- second most common source of GI bleeding in patients over age 60 3. IBD- (UC, Crohn's disease) 4. colorectal carcinoma 5. colorectal adenomatous polyps 6. ischemic colitis 7. hemorrhoids, anal fissures 8. small intestinal bleeding - diagnosed by excluding upper GI and colonic bleeding |
|
|
What is hematemesis and what does it suggest?
|
vomiting blood-- suggests an upper GI bleed (bleeding proximal to the ligament of Treitz). Indicates moderate to severe bleeding that may be ongoing
- if massive bleed may see signs of volume depletion and signs and symptoms of anemia-- fatigue, pallor, dyspnea |
|
|
What is "coffee ground emesis" and what does it suggest?
|
darker, "coffee ground" appearing emesis which suggests an upper GI bleeding at a lower rate-- enough time for the blood to be partly digested and take on the appearance of coffee grounds
|
|
|
What is "melena" and what does it suggest?
|

Black, tarry, liquid, foul-smelling stool
-- caused by degradation of hemoglobin by bacteria in the colon-- presence of melena indicates that blood has remained in the GI tract for several hours - the further the bleeding site is from the rectum, the more likely it is for melena to occur - note that dark stools can also result from bismuth, iron, spinach, charcoal and licorice - melena suggests upper GI bleeding 90% of the time. Occasionally, the jejunum or ileum is the source. It is unusual for melena to be caused by a colonic lesion, but if it is, the ascending colon is the most likely site |
|
|
What is "Hematochezia" and what does it suggest?
|
- Bright red blood per rectum
- this usually represents a lower GI source (typically left colon or rectum)-- consider diverticulosis, AVM, hemorrhoids or colon cancers - it may result from massive upper GI bleeding that is very brisk (5-10% of time) |
|
|
What is "occult" blood in the stool?
|
- blood that is discovered on fecal occult blood test-- cannot be seen grossly.
- source of bleeding may be anywhere along the GI tract |
|
|
what should you always ask patients with GI bleeding?
|
If they are on NSAIDs/aspirin, clopidogrel (plavix) or other anticoagulants
|
|
|
what should you always think of when you see a lower GI bleed or positive fecal occult blood test in someone over 40?
|
Colon cancer until proven otherwise
|
|
|
Aortoenteric fistula
|
- a rare but potential lethal cause of GI bleed
- classic presentation is a patient with a history (sometimes remote) of aortic graft surgery that develops a small amount of GI bleeding involving the duodenum before having a fatal, massive hemorrhage hours to weeks later - perform endoscopy or surgery during this small window of opportunity to prevent death |
|
|
What tests should you order in a patient with GI bleeding?
a. hematochezia b. hematemesis c. melena d. occult blood |
a. hematochezia- first rule out anorectal cause (hemorrhoids). Colonoscopy should be the initial test because colon cancer is the main concern in all patients over 50
b. hematemesis- upper GI endoscopy is the initial test c. Melena- upper endoscopy is usually the initial test because the most likely bleeding site is the upper GI tract. Order a colonoscopy if no bleeding site is identified from the endoscopy d. occult blood- colonoscopy is the initial test is more cases as colon cancer is the main concern. Order an upper endoscopy if no bleeding site is identified from the colonscopy |
|
|
Laboratory tests for diagnosis GI bleeds
|
1. stool guaiac for occult blood
2. hemoglobin/hematocrit-- may not be decreased in acute bleeds. A hemoglobin level > 7 to 8 g/dL is generally acceptable in young, healthy patients without active bleeding, however most elderly patients (especially those with cardiac disease) should have a hgb > g/dL 3. A low MCV is suggestive of iron deficiency anemia (chronic blood loss). Patients with acute bleeding have normocytic RBCs 4. Coagulation profile (platelets, PT, PTT and INR) 5. LFTs, renal function (BUN, Cr) 6. The BUN-Creatinine ratio is elevated with upper GI bleeding. This is suggestive of upper GI bleeding if patient has no renal insufficiency. The higher the ratio, the more likely the bleeding is from an upper GI source |
|
|
Role of upper endoscopy in evaluating a GI bleed
- when should it be performed? |
- most accurate diagnostic test in evaluation of upper GI bleeding
- both diagnostic and potentially therapeutic (coagulate bleeding vessel) - most patients with upper GI bleeding should have upper endoscopy within the first 24 hours |
|
|
Role of nasogastric tube (NG tube) in evaluation of upper GI bleeding?
|
- often the initial procedure for determining whether GI bleeding is from an upper or lower GI source
- use the NG tube to empty the stomach to prevent aspiration - false-negative findings are possible if upper GI bleeding is intermittent or from a lesion in the duodenum - Evaluation of aspirate- bile present, but no blood (upper GI bleed unlikely--probably from site distal to liagment of Treitz), bright red blood or "coffee ground emesis" (upper GI bleed), non-bloody aspirate--clear gastric fluid (upper GI bleed unlikely, but cannot be ruled out definitively (source may possibly be in the duodenum) |
|
|
Role of anoscopy or proctosigmoidoscopy in evaluation of GI bleed
|
can exclude an anal/rectal source. Perform this if there is no obvious bleeding from hemorrhoids
|
|
|
role of colonoscopy in the evaluation of GI bleeding
|
- identifies the site of lower GI bleeding in >70% of cases and can also be therapeutic
|
|
|
Role a of a bleeding/radionucleotide scan in evaluating GI bleeding
|
- reveals bleeding even with a low rate of blood loss
- it does NOT localize the lesion, it only identifies continued bleeding - its role is controversial, but it may help determine whether angiography is needed |
|
|
Role of arteriography in evaluation of GI bleeding
|
- definitively locates the point of bleeding
- mostly used in patients with lower GI bleeding - should be performed during active bleeding - potentially therapeutic (embolization or intra-arterial vasopressin infusion) |
|
|
role of exploratory laparotomy in evaluation of GI bleed
|
LAST RESORT
|
|
|
Treatment of GI bleed- all patients
|
If patient is hemodynamically unstable, resuscitation is always a top priority
- Remember the ABCs. Once the patient is stabilized, obtain a diagnosis - supplemental O2 - place 2 large bore IV lines. Give fluids or blood if patient is volume depleted. - draw blood for hgb, hct, platelets, PT and PTT. Monitor hgb q 4-8 hours until the patient's hemoglobin has been stable for at least 24 hours - type and crossmatch adequate blood (PRBCs). Transfuse as clinical condition demands (e.g. shock, patients with cardiopulmonary disease etc) |
|
|
Treatment of upper GI bleed
|
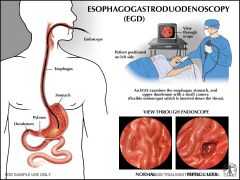
esophagogastroduodenoscopy (EGD/upper endoscopy) with coagulation of the bleeding vessel. If the bleeding continues, repeat endoscopic therapy or proceed with surgical intervention (ligation of the bleeding vessel)
|
|
|
Treatment of lower GI bleeding
|
- colonscopy- polyp excision, injection, laser, cautery
- arteriographic vasoconstrictor infusion - surgical resection of involved area- last resort |
|
|
Indications for surgery in GI bleed
|
1. hemodynamically unstable patient who has not responded to IV fluid, transfusion, endoscopic intervention or correction of coagulopathies
2. severe initial bleed or recurrence of bleed after endoscopic treatment 3. continued bleeding for more than 24 hours 4. visible vessel at base of ulcer (30% to 50% chance of rebleed) 5. ongoing transfusion requirement (5 unites within the first 4-6 hours) |
|
|
Two types of esophageal carcinoma
|
1. squamous cell carcinoma (used to be 90% of cases)
2. Adenocarcinoma - on the rise, risk factors include GERD-- now accounts for 50% of new cases in the US |
|
|
Squamous cell carcinoma of the esophagus
1. what population is the most affected? 2. where is it most common within the esophagus? 3. what are the risk factors? |
1. african american men
2. upper thoracic and mid thoracic esophagus. 1/3 may be in the distal 10 cm of the esophagus 3. alcohol and tobacco use, diet (nitrosamines, betel buts, chronic ingestion of hot foods and beverages such as tea), HPV, achalasia, Plummer-Vinson syndrome, caustic ingestion and nasopharyngeal carcinoma |
|
|
Adenocarcinoma of the esophagus
1. what population is the most affected? 2. where is it most common within the esophagus? 3. what are the risk factors? |
1. more common in caucasians and men (5:1 over women)
2. most common in distal third of esophagus/GE junction (in 80% of cases) 3. GERD and Barrett's esophagus are the main risk factors. Alcohol and tobacco are not as important as in SCC |
|
|
Prognosis for esophageal cancer of both types
|
Very poor- 5 year survival rate is about 5% to 15% for both types
|
|
|
Staging of esophageal cancer
I IIa IIb III IV |
I- tumor invades lamina propria or submucosa, nodes are negative
IIa. tumor invades the muscularis propria or adventitia, nodes negative IIb. tumor invades up to the muscularis propria, positive regional nodes III. tumor invades adventitia (positive regional nodes) or tumor invades adjacent structures (positive or negative nodes) IV. distant mets |
|
|
Clinical features of esophageal carcinoma
|
1. dysphagia- most common symptom (initially for solids only, then progression to liquids)
2. weight loss - second most common symptom 3. anorexia 4. odynophagia (pain with swallowing) - a late finding that suggests extraesophageal involvement (mediastinal invasion) 5. hematemesis- hoarseness of voice (recurrent laryngeal nerve involvement) 6. aspiration pneumonia- respiratory symptoms due to involvement of tracheobronchial tree 7. tracheoesophageal or bronchoesophageal fistula 8. chest pain |
|
|
Diagnosis of esophageal carcinoma
|
1. barium swallow useful in the evaluation of dysphagia-- a presumptive diagnosis can be made
2. upper endoscopy with biopsy and brush cytology is required for definitive diagnosis in 95% of cases 3. transesophageal ultrasound helps determine the depth of penetration of the tumor and is the most reliable test for staging local cancer 4. full metastatic workup (e.g. CT chest/abdomen, CXR and bone scan) |
|
|
Treatment of esophageal cancer
|
1. Palliation is the goal in most patients because the disease is usually advanced at presentation
2. surgery (esophagectomy) may be curative for patients with disease in stage 0, 1, or 2 a 3. chemotherapy plus radiation before surgery has been shown to prolong survival more than surgery alone |
|
|
Achalasia
1. definition 2. criteria for diagnosis |
1. acquired motor disorder of esophageal smooth muscle in which the lower esophageal sphincter (LES) fails to completely relax with swallowing and abnormal peristalsis of esophageal body replaces normal peristalsis of the esophageal body
2. Absolute criteria for diagnosis- incomplete relaxation of the LES, and aperistalsis of the esophagus |
|
|
Causes of achalasia
|
1. the majority of cases in the US are idiopathic
2. in the US, adenocarcinoma of the proximal stomach is the second most common cause 3. Worldwide, Chagas' disease is an important cause |
|
|
Clinical features of achalasia
|
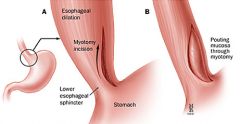
1. dysphagia (odynophagia is less common)
- equal difficulty swallowing solids and liquids (in contrast to esophageal cancer, in which dysphagia for solids is greater than for liquids). - patients tend to eat slowly and drink lots of water to wash down food. Also, they may twist their body, extend their neck, or walk about the room in effort to force food into their stomach 2. regurgitation-- food gets "stuck" in the esophagus and then comes back up. This may lead to regurgitation 3. chest pain 4. weight loss 5. recurrent pulmonary complications secondary to aspiration, which may cause lung abscesses, bronchiectasis or hemoptysis Picture is of heller myotomy- one of the treatments for achalasia |
|
|
Diagnosis of achalasia
|

1. Barium swallow - "bird's beak"- beak-like narrowing of distal esophagus and a large, dilated esophagus proximal to the narrowing
2. Upper GI endoscopy- to rule out secondary causes of achalasia (gastric carcinoma) and retention esophagitis or esophageal cancer 3. manometry - to confirm the diagnosis- reveals failure of LES relaxation and aperistalsis of the esophageal body |
|
|
Risk of esophageal carcinoma in patients with achalasia
|
Sevenfold increase in the risk of esophageal cancer (usually SCC)
- it occurs in 10% of patients 15-25 years after the initial achalasia diagnosis. - Often tumors go unnoticed (even when large) due to a dilated esophagus and chronic dysphagia. Therefore, perform a surveillance scope to detect the tumor at an early stage |
|
|
Treatment of achalasia
|
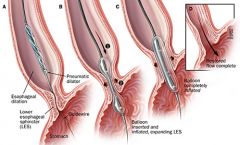
1. Instruct the patient on adaptive measures- chew food to consistency of pea soup before swallowing. Sleep with trunk elevated, avoid eating before sleep.
2. Medical therapy a. antimuscarinic agents (dicyclomine)- usually unsatisfactory b. sublingual nitroglycerin, long-acting nitrates, and calcium channel blockers. May improve swallowing in early stages of achalasia (before esophageal dilatation occurs). Most useful in the short-term treatment of achalasia (before more definitive therapy) 3. Injecting of botulinum toxin into the LES during endoscopy. Blocks cholinergic activity in the LES. Can be effective in up to 65% of cases. however repeat procedure needs to be performed every 2 years. 4. forceful dilatation- can be mechanical, pneumatic, or hydrostatic. Pneumatic balloon dilatation is most effective. Lowers basal LES tone by disrupting the muscular ring. can be effective, there is a 5% risk of perforation 5. surgical a. Heller myotomy- circular muscle layer of LEW is incised b. usually reserved for patients who do not respond to dilation therapy 6. Early results a promising (80-90% of patients experience good to excellent palliation of dysphagia at 1 year) 7. Long term data is still needed |
|
|
Diffuse esophageal spasm
1. definition/ general characteristics 2. clinical features 3. diagnosis |

1. Nonperistaltic spontaneous contraction of the esophageal body-- several segments of the esophagus contract simultaneously and prevent appropriate advancement of the food bolus. In contrast to achalasia, sphincter function is normal (normal LES pressure)
2. There is noncardiac chest pain that mimics angina and may radiate to the jaw, arms and back. Dysphagia is common, however there is no regurgitation of food usually. 3. Diagnosed by esophageal manometry - simultaneous, multiphasic, repetitive constractions that occur after a swallow, sphincter response is normal. Upper GI barium swallow shows "corkscrew esophagus"- in 50% of cases which represents multiple spontaneous contractions |
|
|
Treatment of diffuse esophageal spasm
|
1. In general, there is no completely effective therapy-- treatment failure rates are high
2. medical treatment involves nitrates and calcium channel blockers (decreases amplitude of contractions). Tricyclic antidepressants may provide symptomatic relief 3. esophagomyotomy is usually not performed, and its efficacy is controversial. Some support its use, whereas others only recommend it when a patient is incapacitated my symptoms |
|
|
2 types of esophageal hernia and characteristics of each
|
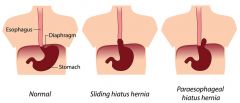
1. sliding hiatal hernia (type 1) - accounts for 905 of cases. Both the gastroesophageal (GE) junction and a portion of the stomach herniate into the thorax through the esophageal hiatus (so that the GE junction is above the diaphragm)- this a common and benign finding that is associated with GERD
2. paraesophageal hiatal hernia - accounts for <5% of cases. The stomach herniates into the thorax through the esophageal hiatus, but the GE junction does not. It remains below the diaphragm. This uncommon hernia can become strangulated and should be repaired surgically. These tend to enlarge with tim, and the entire stomach may ultimately move into the thorax 3. type 3 hernia are a combination of type 1 and 2 and are treated as type 2 hernias (surgically) |
|
|
Clinical features of esophageal hernias
|
1. The majority of cases are asymptomatic and are discovered incidentally
2. possible symptoms include heartburn, chest pain, and dysphagia 3. complications of sliding hiatal hernias include GERD (most common), reflux esophagitis (with risk of Barrett's esophagus/cancer), and aspiration 4. Complications of paraesophageal hernias are potentially life-threatening and include obstruction, hemorrhage, incarceration and strangulation |
|
|
Diagnosis of esophageal hernias
|
Barium upper GI series and upper endoscopy
|
|
|
Treatment of esophageal hernias by type
|
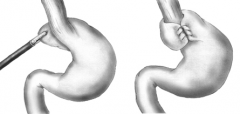
1. Type 1 hernias are treated medically (with antacids, small meals and elevation of the head after meals); 15% of cases may require surgery (Nissen's fundoplication) if there is no response to medical therapy or if there is evidence of esophagitis
2. Type 2 hernias treated with elective surgery due to risk of strangulation |
|
|
Mallory-Weiss Syndrome
|
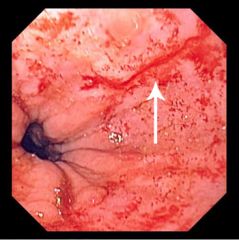
1. mucosal tear at (or just below) the GE junction as a result of forceful vomiting or retching. It usually occurs after repeated episodes of vomiting, but it may occur after one episode
2. it is most commonly associated with binge drinking in alcoholics, but any disorder that causes vomiting can induce the mucosal tear 3. hematemesis is always present- it varies from streaks of blood in vomitus to massive bright red blood 4. upper endoscopy is diagnostic 5. most cases (90%) stop bleeding without any treatment 6. Treatment is surgery (oversewing the tear) or angiographic embolization if bleeding continues, but this is rarely necessary. Acid suppression is used to promote healing |
|
|
Plummer-Vinson Syndrome
|
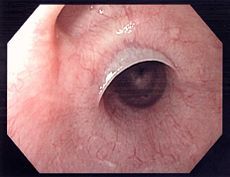
1. key features: upper esophageal web (causes dysphagia), iron deficiency anemia, koilonychia (spoon-shaped fingernails), and atrophic oral mucosa
2. 10% of patients develop SCC of the oral cavity, hypopharynx or esophagus, therefore, this is considered a premalignant lesion 3. treatment: esophageal dilatation, correct nutritional deficiency |
|
|
Schatzki's Ring
1. what is it? 2. symptoms 3. treatment 4. causes? 5. acid vs base ingestion 6. complications 7. treatment |

1. distal esophageal webs- a circumferential ring in the lower esophagus that is always accompanied by a sliding hiatal hernia
2. It is usually asymptomatic, but mild to moderate dysphagia may be present 3. If the patient is symptomatic (but has no reflux), consider esophageal dilatation. If the patient has reflux, consider antireflux surgery (e.g. nissen) 4. usually due to ingestion of alkali, bleach, or detergent 5. ingesting alkali is more dangerous than infesting acid because it may lead to liquefactive necrosis of the esophagus with full-thickness perforation. Acid ingestion does not cause full-thickness damage (only causes necrosis of esophageal mucosa). 6. Complications : stricture formation and risk of esophageal cancer 7. Treatment is esophagectomy if full thickness necrosis has occurred. Patient should avoid vomiting, gastric lavage, and all oral intake (can compound the original injury). Give the patient steroids and antibiotics. Perform bougienage for esophageal stricture |
|
|
Mallory Weiss syndrome vs Boerhaave's syndrome
|
During forceful vomiting, the marked increase in intra-abdominal pressure is transmitted to the esophagus. This can lead to two conditions, depending on the severity and location of the tear.
1. If the tear is mucosal at the GE junction, it is referred to as a mallory weiss tear 2. If the tear is transmural (causing esophageal perforation) it is referred to as Boerhaave's syndrome picture- boerhaave's syndrome |
|
|
Esophageal diverticula
1. most common cause 2. most common type 3. mechanism of most common type 4 and 5. clinical features of most common type, age affected 6. traction diverticula 7.epiphrenic diverticula 8. diagnosis 9. treatment |
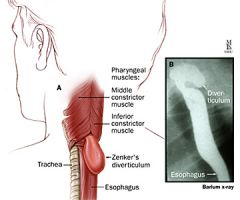
1. most esophageal diverticula are caused by an underlying motility disorder of the esophagus
2. Zenker's diverticulum is the most common type-- found in the upper 1/3 of the esophagus 3. Failure of the cricopharyngeal muscle to relax during swallowing leads to increased intraluminal pressure. This causes outpouching of mucosa through an area of weakness in the pharyngeal constrictors 4. clinical features include dysphagia, regurgitation, halitosis, weight loss and chronic cough 5. It is typically seen in patients > 50 years old 6. traction diverticula- located in the midpoint of the esophagus near the tracheal bifurcation. It is due to traction from contiguous mediastinal inflammation and adenopathy (pulmonary tuberculosis). Tuberculosis causes hilar node scarring, which causes retraction of the esophagus. It is usually asymptomatic and does not require treatment 7. epiphrenic diverticuli- found in the lower 1/3 of the esophagus. It is usually associated with spastic esophageal dysmotility or achalasia. Symptoms of dysphagia are more often related to the underlying motility disorder, unless the diverticulum is very large 8. Barium swallow is the best diagnostic test for divertula. 9. Treatment of Zenker's diverticula is surgery. Cricopharyngeal myotomy has excellent results. Treatment of epiphrenic diverticula is esophagomytomy. Diverticulectomy is of secondary importance in both cases Picture- Zenker's Diverticulum |
|
|
Esophageal perforation
1. etiology 2. clinical features 3. diagnosis 4. treatment- stable vs unstable pt |
1. blunt trauma, medical tubes and instruments, forceful vomiting (Boerhaave's syndrome) that is associated with alcoholic binges and bulimia
2. pain (severe retrosternal/chest/shoulder pain), tachycardia, hypotension, tachypnea, fever, Hamman's sign (mediastinal crunch- produced by heart beating against air-filled tissues), pneumothorax, pleural effusion 3. contrast esophagram is the definitive diagnostic study (soluble gastrogafin swallow preferred), CXR0 usually shows air in the mediastinum 4. if the patient is stable and the perforation is small (draining into lumen)- medical management is appropriate - IV fluids, NPO, antibiotics, and H2 blockers - if patient is ill and perforation is large- or there is communication into the pleural cavity, surgery should be performed within 24 hours of presentation (success rate is higher) - if gastric/esophageal contents leak into the mediastinum or pleura, infection and septic sequela may result - The time interval between esophageal perforation and surgery is the most important factor in determining survival. If surgery is delayed beyond 24 hours, the mortality rate and the likelihood of fistulization increase |
|
|
Peptic ulcer disease
1. most common causes 2. other causes |
1. most common causes- H. pylori infection, NSAIDs- inhibit prostoglandin production, which leads to impaired mucosal defenses. Zollinger-Ellison syndrome- acid hypersecretory states
2. Other causes- smoking- ulcers are twice as likely in smokers, alcohol and coffee- may exacerbate symptoms, but causal relationship is as yet unproven 3. other potential unproven causes- emotional stress, personality type A, and dietary factors |
|
|
Clinical features of peptic ulcer disease
|
1. epigastric pain- aching or gnawing in nature
- nocturnal symptoms and effect of food on symptoms are variable 2. may be complicated by upper GI bleeding 3. other symptoms- n/v, early satiety, and weight loss |
|
|
Diagnosis
1. most accurate method? 2. most convenient test? 3. lab tests 4. if considering a dx of Zollinger Ellison syndrome? |

1. Endoscopy- most accurate test in diagnosing ulcers, essential in diagnosis of gastric ulcers because biopsy is necessary to r/o malignancy- duodenal ulcers not require biopsy. Preferred when severe or acute bleeding is present (can perform electrocautery of bleeding ulcers)
2. Barium swallow- sometimes used initially but is less reliable than endoscopy. Double contrast techniques preferred due to improved accuracy 3. lab tests- for diagnostic evaluation of h. pylori infection- a. biopsy: histologic evaluation of endoscopic biopsy is the gold standard - urease detection via urea breath test - most convenient test (sensitivity and specificity > 95%). It documents active infection and helps to assess the results of antibiotic therapy - serology - lower specificity - the presence of h. pylori does not necessarily indicate current infection-- antibodies to h. pylori can remain elevated for months or even years after eradication of infection. There may also be false positives because of PPIs, bismuth, many abx and GI bleeding 4. serum gastrin measurement- if considering Zollinger-Ellison syndrome as diagnosis -- if a peptic ulcer is uncomplicated, a barium study or endoscopy is not needed initially. Initiate empiric therapy. However, if complications are suspected, order confirmatory tests |
|
|
Medical Treatment of peptic ulcer disease
|
1. Medical- the majority of patients with PUD can be successfully treated by curing H. pylori infection, avoidance of NSAIDs, and appropriate use of antisecretory drugs
a. supportive- discontinue aspirin, restrict alcohol use, but do not restrict any foods, stop smoking, decrease stress, avoid eating before bedtime (eating stimulates nocturnal gastric acid levels) b. acid suppression - H2 blockers- accelerate healing of ulcers, PPIs- most effective antisecretory agents (although expensive), antacids - somewhat outdates for primary therapy and most appropriate for adjunctive therapy/symptom relief c. Eradicate h. pylori with triple or quadruple therapy - once infection is cleared the recurrence rate is low. For initial therapy, triple therapy (PPI, amoxicillin, and clarithromycin), for 10 days to 2 weeks, For retreatment quadruple therapy - PPI, bismuth, and 2 antibiotics d. cytoprotection - sulcralfate- faciliates ulcer healing, must be taken frequently, is costly and can cause GI upset. misoprostol- reduces risk of ulcer formation associated with NSAID use, is costly, and cause GI upset (commonly) e. Treatment regimens - if h. pylori test is positive, begin eradication therapy with either triple or quadruple therapy. Also begin acid-suppression with antacids, an H2 blocker or a PPI - if the patient has an active NSAId induced ulcer, stop NSAID use (switch to acetaminophen), Also begin with either PPI or misoprostol. Continue for 4-8 weeks, depending on severity. Treat the h. pylori infection if present - antisecretory drugs can be discontinued after 4-6 weeks in patients with uncomplicated ulcers who are asymptomatic. Patients at increased risk of recurrence (especially if underlying cause of ulcer is not reversed) may benefit from maintenance therapy - h. pylori negative ulcers that NOT caused by NSAIDs can be treated with antisecretory drugs (H2 blockers or PPIs) |
|
|
Surgical treatment of peptic ulcer disease
|
- rarely needed electively
- required for complications of PUD - bleeding perforation, gastric outlet obstruction |
|
|
Complications of Peptic ulcer disease
|
1. perforation- acute severe abdominal pain, signs of peritonitis and hemodynamic instability- upright CXR or CT to detect free air under diaphragm. Tx- emergency surg to close perf and definitive ulcer operation- selective vagotomy or truncal vagotomy/pyloroplasty-- can progress to sepsis and death if untreated
2. gastric outlet obstruction- n/v of poorly digested food, epigastric fullness/early satiety and weight loss. Barium swallow and upper endoscopy, saline load test (empty stomach with NG tube, add 750 mL saline, aspirate after 30 min, test is positive if aspirate > 400mL. Tx- initially NG suction, replaced electrolyte/volume deficits. Supplemental nutrition if obstruction is longstanding. Surgery is eventually necessary in 75% of patients. Most common with duodenal ulcers and type III gastric ulcers 3. GI bleeding - bleeding may be slow (leading to anemic symptoms) or can be rapid and severe (leading to shock. Stool guaiac, upper GI. Tx- resuscitation, diagnose site of bleed via endoscopy and treat- perform surgery for acute bleeds that require transfusion of > 6 units. PUD is the most common cause of upper GI bleeding |
|
|
duodenal vs gastric ulcers
|
1. duodenal ulcers- caused by increase in offensive factors (higher rates of basal and stimulated gastric acid secretion), 70-90% of patients have h. pylori, Low (malignancy is very rare) should undergo biopsy to r/o. The majority are located 1-2 cm distal to pylorus (usually on posterior wall). Usually occurs in younger patients (<40), assoc with blood type O, NSAIDs- RF, eating usually relieves pain (food in duodenum stimulates bicarb secretion). Nocturnal pain is more common than in gastric ulcers
2. gastric ulcer- caused by a decrease in defensive factors (gastric acid level is normal/low unless ulcer is pyloric or pre-pyloric). 60-70% of patients have h. pylori, high malignant potential (5-10% are malignant), 4 types depending on location - type I is most common- on lesser curvature of stomach - 70%, occurs in older patients > 40, assoc with blood type A, smoking - RF, eating makes it worse- stimulates acid secretion, complication rates are higher than with duodenal ulcers. Higher risk of recurrence with medical therapy alone |
|
|
Acute gastritis
1. definition 2. causes 3. symptoms 4. treatment 5. if no response to tx after 4-8 weeks? |
1. inflammation of the gastric mucosa
2. there are multiple causes- NSAIDs/aspirin, h. pylori infection, alcohol, heave cigarette smoking, or caffeine, extreme physiologic stress- e.g. shock, sepsis, burns 3. it can be either asymptomatic or cause epigastric pain. The relationship between eating and pain is not consistent 4. if epigastric pain is low/mod and is not associated with worrisome sx/findings, empiric therapy with acid suppression is appropriate. stop NSAIDs 5. If there is no positive response after 4-8 weeks of treatment, consider a diagnostic w/u (include upper GI endoscopy and US to r/o gallstones) and test for h. pylori |
|
|
Chronic gastritis
1. most common cause 2. progression 3. symptoms 4. complications |
1. the most common cause is h. pylori (over 80% of cases)
2. autoimmune gastritis leads to chronic atrophic gastritis with serum antiparietal and anti-intrinsic factor antibodies (possible development of pernicious anemia) 3. most patients with chronic gastritis due to h. pylri are asymptomatic and never develop complications. The condition may manifest as epigastric pain similar to PUD. Other associated symptoms are n/v and anorexia. 4. complications include PUD, gastric carcinoma, and mucosa-associated lymphoid tissue (MALT) lymphoma 5. upper endoscopy with biopsy is the test of choice for diagnosis of chronic gastritis. Other tests should be used to find the cause (usually h. pylori) |
|
|
Gastric cancer
1. most common type 2. where is it common geographically? 3. morphology |

1. majority are adenocarcinomas
2. gastric cancer is rare in the US but more common in Japan (relation to smoked foods?) 3. a. ulcerative carcinoma- ulcer through all layers b. polypoid carcinoma- solid mass projects into stomach lumen c. superficial spreading- most favorable prognosis d. linitis plastic - "leather water bottle" - infiltrates early through all layers, stomach wall is thick and rigid, poor prognosis |
|
|
Risk factors for gastric carcinoma
|
1. severe atrophic gastritis, intestinal metaplasia, gastric dysplasia
2. adenomatous gastric polyps, chronic atrophic gastritis 3. h. pylori infection - 3-6-fold increase in risk 4. postantrectomy- many cases reported after Billroth II anastamosis - 15-20 yrs later 5. pernicious anemia - 3-fold increased risk 6. menetrier's disease - 10% develop cancer 7. high intake of preserved foods - high salt, nitrates, nitrites- smoked fish 8. blood type A |
|
|
Clinical features of gastric cancer
|
1. abdominal pain and unexplained weight loss are the most common symptoms
2. reduced appetite, anorexia, dyspepsia, early satiety 3. n/v, anemia, melena, guaiac-positive stool |
|
|
Diagnosis of gastric carcinoma
|
1. endoscopy with multiple biopsies- most accurate test
2. barium upper GI series- less accurate, but can complement upper endoscopy findings 3. abdominal CT scan- for staging and to detect presence of mets 4. FOBT |
|
|
Treatment of gastric carcinoma
|
1. surgical resection with wide > 5 cm margins - total and subtotal gastrectomy with extended lymph node dissection
2. chemotherapy may be appropriate in some cases |
|
|
Gastric lymphoma
|
1. a type of non-hodgkins lymphoma that arises in the stomach
2. clinical features are similar to those of adenocarcinomas of the stomach (e.g. abdomina pain, weight loss, anorexia) 3. complications include bleeding, obstruction, and perforation 4. diagnosis- EGD with biopsy is standard of diagnosi 5. tx- depends on stage of the disease and the presence of complications. options include surgical resection, radiation, and chemotherapy |
|
|
What is the best test for evaluating a patient with epigastric pain?
|
Upper GI endoscopy as it can diagnose PUD, gastritis and esophagitis. It can also rule out cancers of the esophagus and stomach, and h. pylori infection with biopsy
|
|
|
What are the 3 main points to consider in small bowel obstruction?
|
1. partial vs complete obstruction- with a partial obstruction, patients are able to pass gas or have bowel movements as opposed to a complete obstruction. However, patients with a complete obstruction may occasionally be able to pass gas or stool because they have residual stool or gas in the colon
2. Closed loop vs open loop obstruction - with closed loop obstruction, the lumen is occluded at 2 points by an adhesive band or hernia ring. This can compromise the blood supply and require emergent surgery. 3. Proximal versus distal small bowel obstruction (SBO)- distal obstruction causes distention of the proximal bowel segments, making a diagnosis easier on plain film |
|
|
Pathophysiology of small bowel obstruction
|
1. dehydration is the key event in SBO.
- Intestinal distention causes reflex vomiting, increased intestinal secretion proximal to the point of obstruction, and decreased absorption. This leads to hypochloremia, hypokalemia and metabolic alkalosis 2. The resulting hypovolemia leads to systemic findings such as tachycardia, hypotension, tachypnea, AMS, oliguria |
|
|
Causes of Small Bowel Obstruction
|
1. Adhesions from previous abdominal surgery- most common cause in adults
2. Incarcerated hernias- second most common cause 3. Malignancy, intussusception, Crohn's disease, carcinomatosis, and superior mesenteric artery syndrome (compression of the third portion of the duodenum) |
|
|
Clinical features of small bowel obstruction
|
1. crampy abdominal pain- if the pain is continuous and severe, strangulation may be present
2. N/v- may be feculent 3. obstipation - absence of stool and flatus 4. abdominal distention |
|
|
Diagnosis of small bowel obstruction
|
1. Abdominal plain films- dilated loops of small bowel, air0fluid levels proximal to the point of obstruction (on upright film), and minimal gas in colon (if complete SBO)
2. Barium enema- to rue out colonic obstruction if plain films do not distinguish small from large bowel obstruction. This identifies the site of obstruction 3. Upper GI series- with small bowel follow through if above are not diagnostic |
|
|
Treatment of small bowel obstruction
|
1. Nonoperative management- appropriate if bowel obstruction is incomplete and there is no fever, tachycardia, peritoneal signs, or leukocytosis
2. IV Fluids to establish adequate urine output, add potassium to fluids to correct hypokalemia (which is typically present) 3. NG tube to empty the stomach (gastric decompression) 4. Antibiotics 5. Surgery is indicated for complete obstruction, for partial obstruction that is persistent and/or associated with constant pain, or if strangulation is suspected. Perform an exploratory laparotomy with lysis of adhesions and resection of any necrotic bowel |
|
|
Paralytic Ileus
1. definition 2. causes 3. abd plain film appearance 4. diagnosis 5. treatment |
1. peristalsis is decreased or absent (no mechanical obstruction is present)
2. causes include medications (narcotics, drugs with anticholinergic effects), postoperative state (after abd surgery), spinal cord injury, shock, metabolic disorders (especially hypokalemia) and peritonitis 3. Abdominal plain films show a uniform distribution of gas in the small bowel, colon, and rectum (in contract to small bowel or colonic obstruction) 4. Failure to pass contrast medium beyond a fixed point is diagnostic 5. treatment- IV Fluids, NPO, correction of electrolyte imbalances (especially hypokalemia), NG suction if needed, and placement of a long tube if ileus persists postoperatively |
|
|
Celiac Sprue
1. what is it? 2. symptoms 3. diagnosis 4. treatment |
- characterized by hypersensitivity to gluten (in wheat products)
- results in weight loss, abdominal distention, bloating and diarrhea - biopsy in proximal small bowel reveals flattening of villi, which causes malabsorption - strict adherence to a gluten-free diet is essential |
|
|
Crohn's disease
1. definition 2. Distribution |
1. chronic transmural inflammatory disease that can affect any part of the GI tract (mouth to anus) but most commonly involves the small bowel (terminal ileum)
2. Distribution: There are three major patterns of disease. - 40% of patients have disease in the terminal ileum and cecum - 30% of patients have disease confined to the small intestine - 25% of patients have disease confined to the colon - Rarely, other parts of the GI tract may be involved (stomach, mouth, esophagus) |
|
|
Pathology of Crohn's disease
|
1. Terminal ileum is the hallmark location, but other sites of GI tract may also be involved
2. Skip lesions- discontinuous involvement 3. Fistulae 4. luminal strictures 5. non-caseating granulomas 6. Transmural thickening and inflammation (full-thickness wall involvement) - results in narrowing of the lumen 7. Mesenteric "fat creeping" onto the antimesenteric border of the small bowel |
|
|
Clinical features of crohn's disease
|

1. diarrhea (usually without blood)
2. malabsorption and weight loss (common) 3. abdominal pain (usually RLQ), n/v 4. fever, malaise 5. extraintestinal manifestations in 15-20% of cases (uveitis, arthritis, ankylosing spondylitis, erythema nodosum, pyoderma gangrenosum, apthous oral ulcers (cold sores), and nephrolithiasis |
|
|
Epidemiology of inflammatory bowel disease-- who is it most common in?
|
- more common in caucasians than other racial groups
- particularly common in Jewish populations - mean age of onset is 15-35 years of age |
|
|
Course of crohn's disease
|
- chronic indolent course characterized by unpredictable flares and remissions
- the effectiveness of medical treatment decreases with advancing disease and complications eventually develop, requiring surgery - There is no cure, and recurrence is common even after surgery |
|
|
Treatment of paralytic ileus
|
- usually resolves with time or when the cause is addressed medically
- surgery is usually not needed |
|
|
Diagnosis of crohn's disease
|

1. endoscopy (sigmoidoscopy or colonoscopy) with biopsy- typical findings are apthous ulcers, cobblestone appearance, pseudopolyps, patchy (skip) lesions
2. barium enema 3. upper GI with small bowel follow-through |
|
|
Complications of crohn's disease
|
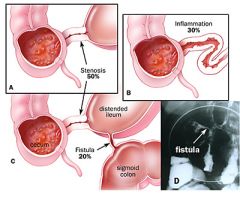
1. fistulae- between colon and other segments of the intestine (enteroenteral), bladder (enterovescial), vagina (enterovaginal), and skin (enterocutaneous)
2. anorectal disease (in 30% of patients)- fissures, abscesses and perianal fistulas 3. SBO (in 20-30% of patients) is the most common indication for surgery. Initially it is due to edema and spasm of bowel with intermittent signs of obstruction, later, scarring and thickening of bowel cause chronic narrowing of the lumen 4. malignancy- increased risk of colonic and small bowel tumors (but less than with UC) 5. Malabsorption of B12 and bile acids (both occur in the terminal ileum) 6. Cholelithiasis may occur secondary to decreased bile acid absorption 7. Nephrolithiasis- increased colonic absorption of dietary oxalate can lead to calcium oxalate kidney stones 8. Aphthous ulcers of lips, gingiva, and buccal mucosa (common) 9. toxic megacolon- less common in crohn's than in UC 10. growth retardation 11. narcotic abuse, psychosocial issues due to chronicity and often disabling nature of the disease |
|
|
Medical Treatment of crohn's disease
|
1. Sulfazalazine - this is useful if the colon is involved- 5-ASA (mesalamine) is the active compound and is released in the colon- it more useful in UC. 5-ASA compounds block prostoglandin release and serve to reduce inflammation. There are preparations of 5-ASA that are more useful in distal small bowel disease
2. Metronidazole (flagyl)- if no response to 5-ASA 3. systemic corticosteroids (prednisone) for acute exacerbations and if no response to metronidazole 4. Immunosuppressants (azathioprine, 6-mercaptopurine) - in conjunction with steroids if the patient does not respond to the above agents 5. bile acid sequestrants -cholestyramine or colestipol- for patients with ileal disease who cannot absorb bile acids 6. anti-diarrheal agents are generally NOT a good choice-- may cause ileus |
|
|
Surgical treatment of crohn's disease
|
- eventually required in most patients
- reserve for complications of crohn's disease - involves segmental resection of involved bowel - disease recurrence after surgery is high- up to 50% of patients experience disease recurrence at 10 years post-op - indications for surgery include SBO, fistulae (especially between bowel and bladder, vagina), disabling disease, and perforation or abscess - nutritional supplementation and support- parenteral nutrition is sometimes necessary |
|
|
Ulcerative colitis (UC)
1. definition and age at presentation 2. distribution |
1. chronic inflammatory disease of the colon or rectal mucosa that may occur at any age, but usually begins in adolescence of young adulthood
2. UC involves the rectum in ALL cases and can involve the colon either partially or entirely. - Rectum alone (in 10% of cases) - rectum and left colon (in 40% of cases) - rectum, left colon and right colon (in 30% of cases), - pancolitis (in 30% of cases) - the small bowel is not usually involved in UC, but it may reach the distal ileum in a small percentage of patients ("backwash ileitis" in 10% of cases) |
|
|
Clinical course of ulcerative colitis
|
The course is unpredictable and variable and is characterized by periodic exacerbations and periods of complete remission.
- less than 5% of patients have an initial attack without any recurrence |
|
|
Pathology of ulcerative colitis
|
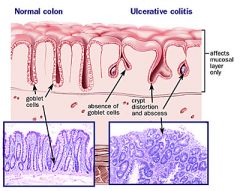
1. uninterrupted involvement of the rectum and/or colon - NO skip lesions
2. inflammation is no transmural as in crohn's-- it is limited to the mucosa, and submucosa 3. PMNs accumulate in the crypts of the colon (crypt abscesses) |
|
|
Clinical features (wide range of presentation)
|
1. hematochezia - may start as non bloody diarrhea and then progress to bloody as disease progresses
2. abdominal pain 3. bowel movements are frequent but small 4. fever, anorexia, and weight loss (severe cases) 5. tenesmus (rectal dry heaves) 6. Extraintestinal symptoms (jaundice, uveitis, arthritis, skin lesions) |
|
|
Diagnosis of ulcerative colitis
|
1. stool cultures for c. diff, ova, and parasites- to rulre out infectious causes of diarrhea
2. fecal leukocytes 3. WBCs can appear in UC, ischemic colitis and or infectious diarrhea 4. colonoscopy- to assess the extent of disease and the presence of any complications |
|
|
Complications of ulcerative colitis
|
1. iron deficiency anemia
2. hemorrhage 3. electrolyte disturbances and dehydration secondary to diarrhea 4. strictures, benign and malignant (usually malignant) 5. colon cancer- the risk correlates with extent and duration of colitis. In distal proctitis there is no increased risk of CRC 6. sclerosing cholangitis - the course is not parallel with bowel disease and is not prevented by colectomy 7. cholangiocarcinoma- half of all bile duct cancers are associated with UC 8. Toxic megacolon- leading cause of death in UC and affects <5% of patients. It is associated with risk of colonic perforation 9. growth retardation 10. narcotic abuse 11. psychosocial issues (e.g. depression) due to chronicity and often disabling nature of the disease |
|
|
Medical Treatment of ulcerative colitis
|
1. Medical
a. systemic corticosteroids are used for acute exacerbations b. sulfasalazine (topical application as a suppository) is the mainstay of treatment. Preferred over topical steroids because they are effective as maintenance therapy. Remission rates are as high as 93%. 5-ASA (mesalazine) is the active component. 5-ASA enemas can be used for proctitis and distal colitis c. immunosuppressive agents in patients with refractory disease may prevent relapses but are not effective for acute attacks |
|
|
Surgical Treatment of ulcerative colitis
|
- often curative (unlike Crohn's disease) and involves total colectomy
- indications for surgery include: - severe disease that is debilitating, refractory, and unresponsive to medical therapy - toxic megacolon (risk of perforation), obstruction (due to stricture), severe hemorrhage, and perforation - fulminant exacerbation that does not respond to steroids - evidence of colon cancer of increased risk of colon cancer - growth failure or failure to thrive in children - systemic complications |