![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
79 Cards in this Set
- Front
- Back
|
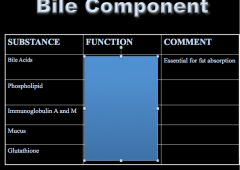
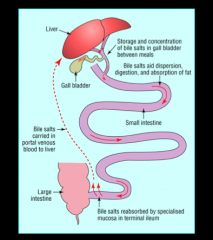
What is the volume of hepatic bile secretion? What are the components of bile? Where are they stored? What does the gall bladder do following a meal? |

|
|
|

|
|
|
What are the three different types of stones? |
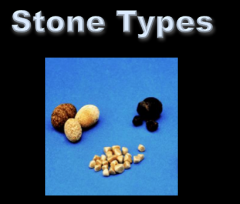
Pure and mixed cholesterol stones Pigmented stone: brown Pigmented stone: black |
|
|
- Most frequent type of stone
|
Pure and mixed cholesterol stones |
|
|
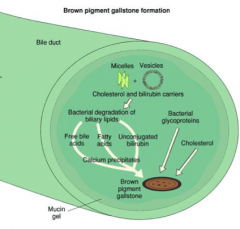
- Calcium salts and deconjugated bilirubin , cytoeskeleton of bacteria Which type of stone? |
Pigmented Stone brown |
|
|
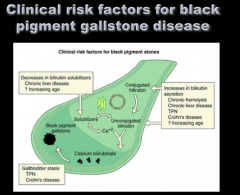
- Black pigmented: seen more in patients with liver disease, hemolysis, older age Which type of stone? |
Pigmented stone black |
|
|
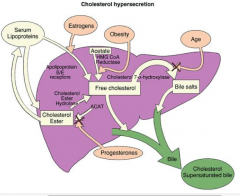
Draw out the pathway of cholesterol metabolism.
What are the three components of the total body pool of cholesterol?
What happens when cholesterol is secreted? |
|
|
|
What are the three components of the total body pool of cholesterol?
What happens when cholesterol is secreted? |

|
|
|
What is the rate limiting enzyme in bile acid synthesis? |
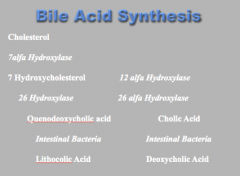
7-a-hydroxylase |
|
|
Draw the pathway of enterhepatic circulation.
How many times per day does this occur? Where is storage? Low absorption? Active and passive absorption? |
Gall bladder = storage Jejunum = low absorption Ileum = active and passive absorption |
|
|
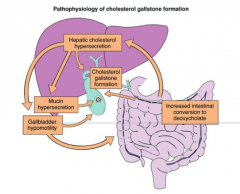
What is the pathophysiology of cholesterol stone formation (3 major components)? |
|
|
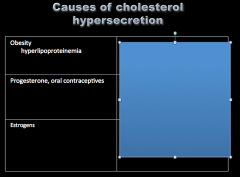
Identify the causes of each: |
|
|
|
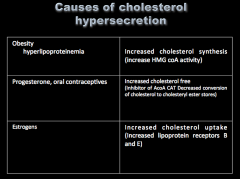
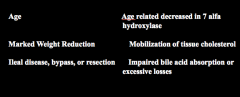
How do each of these cause cholesterol hyper secretion?
Age Marked weight reduction Ileal disease, bypass, or resection |
|
|
|
Are cholesterol molecules soluble in water? How are bile acids able to solubilize cholesterol or phospholipid? |
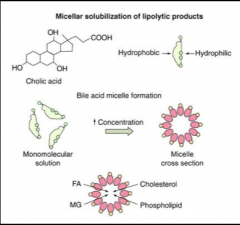
Cholesterol molecules are insoluble in water Amphipathic properties. |
|
|
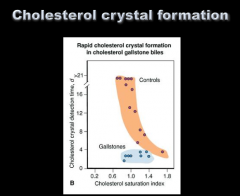
What is the cholesterol saturation index (CSI)?
What is the CSI of bile? |
Ratio of the amount of cholesterol in a given bile sample to the maximal cholesterol micellar-holding capacity of that sample in vitro.
CSI of bile > 1 = supersaturated |
|
|
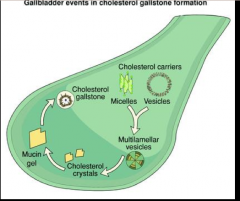
How can cholesterol be found in bile? What are the components of each?
Mixed micelle Simple micelle Vesicles Multilamelar vesicles |

Mixed micelle: bile acids, cholesterol, bilirubin, PC Simple micelle: bile acids, cholesterol, bilirubin Vesicles: 10 times larger, no bile salts Multilamelar vesicles: unstable and permit crystals formation |
|
Crystal formation Crystal generation |
Formation = aggregation process by which crystal particle is formed from supersaturated bile
Generation = vesicular fusion and aggregation |
|
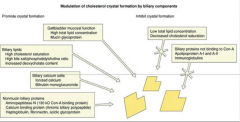
Look over inhibitors and promotors of crystal formation.
The gallbladder mucosa concentrates bile and secretes mucin glycoprotein/ changes in composition of bile (such as high cholesterol saturation and an increased deoxycholate content all enhance what? |
Several factors have been identified that either promote or inhibit the kinetics of cholesterol crystal formation. The |
|
|
Patients with gall-stones have a delay in gallbladder emptying. True or false? |
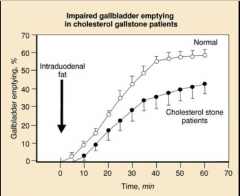
True |
|
|
Defective acidification of gallbladder bile > pH higher precipitation of calcium salts Gallbladder stasis can produce increase of mucin and interfere with mechanical emptying Decreased response to CCK
What are these all risk factors for? |
Gallstone formation |
|
|
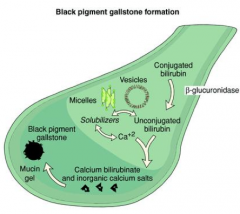
Draw out the pathophysiology of gallstone formation. |
|
|
|
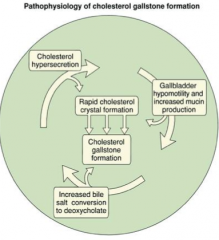
Draw it out again... |
|
|
|
Hemolysis |
Black stones |
|
|
What are some clinical risk factors for black pigment gallstone disease? |
|
|
|
Bacterial infection High activity of B-glucuronidase
What do all these cause? |
Brown stones
(In heart patients?) |
|
|
Draw the pathophysiology of brown pigment gallstone formation. |
|
|
|
What is a cholelith? What is more than 95% of all gallbladder disease? |
|
|
|
What percent of people have cholelithiasis? What countries have highest rates? Lowest? What are the two major types in the US? |
|
|
Review |
|
|
|
What are the clinical manifestations of each?
Biliary colic Acute cholecystitis Choledocholithiasis with cholangitis Biliary pancreatitis |
Choledocholithiasis = also have pain in RUQ |
|
|
What is the most common elective abdominal operation?
What is found in 12%-15% of patients who undergo cholecystectomy? |
|
|
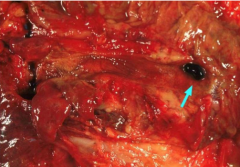
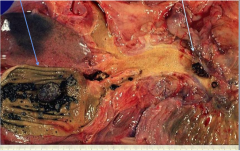
What is the arrow pointing to? |
|
|
|
biliary obstruction, What are these all complications of?
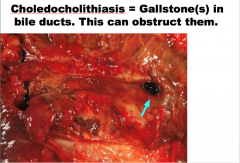
What is cholelithiasis? |
|
|
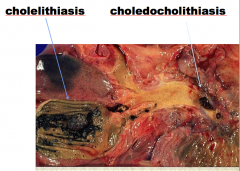
Identify cholelithiasis and choledocholithiasis |
|
|
|
|
|
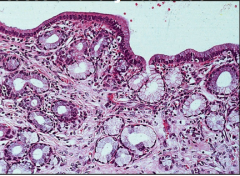
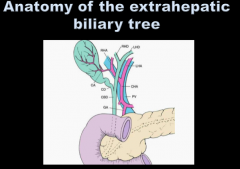
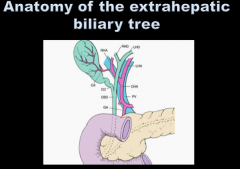
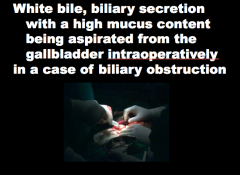
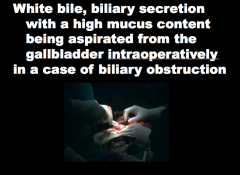
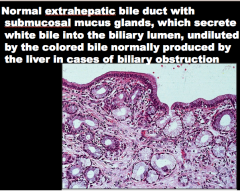
What is the organ? Normal or abnormal? What does it secrete into what? |
|
|
|
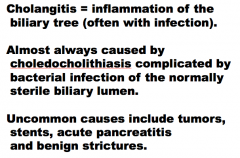
What is inflammation of the biliary tree (often with infection)?
What is is almost always caused by?
What are some uncommon causes? |
|
|
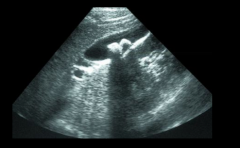
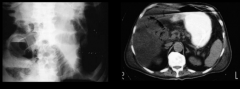
What is the diagnosis? How do you know? What is casting the shadow? |
Stone disease
Hyperechoic (white) structures within the gall-bladder with a shadow. This is the typical appearance of cholelithiasis by ultrasound |
|
What is the diagnosis? How do you know? |
Emphysematous cholecystitis
The presence of air at the gallbladder wall is a radiologic finding highly suggestive of acute cholecystitis |
|
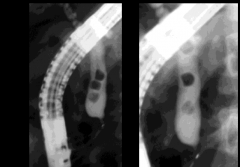
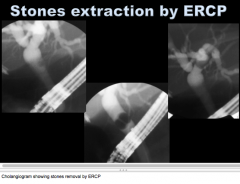
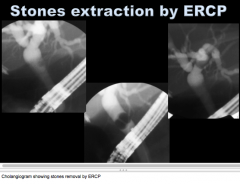
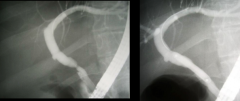
What is the procedure? What does it show?
What percent of patients with cholelithiasis will have this? |
Endoscopic rethrograde cholangiography (ERCP). This cholangiogram shows filling defects consistent with choledocholithiasis |
|
|
|
|
|
|
|
|

|
|
|
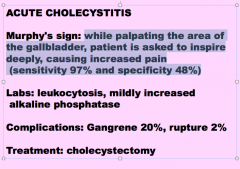
Acute cholecystitis:
Common or uncommon? What percent have gallstones obstructing the neck of the gallbladder or cystic duct
What are the symptoms? Location?
What are the signs? |
|
|
|
Acute cholecystitis:
While palpating the area of the gallbladder, patient is asked to inspire deeply, causing increased pain
What sign is this?
What two labs will you see? What are two complications? What is the treatment? |
|
|
|
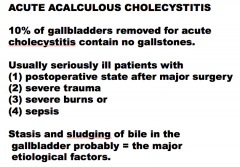
What percent of gallbladders removed for acute cholecystitis contain no gallstones?
What is the term for this?
What are four types of patients who may have this procedure?
What are the two major etiological factors? |
|
|
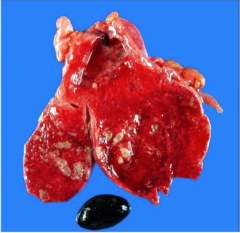
What is the diagnosis? |
|
|
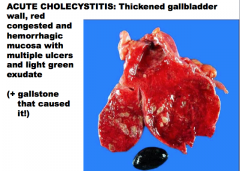
Describe. What is the diagnosis? |

|
|
|
Chronic cholecystitis:
Associated with what two things? What are the symptoms? How do you diagnosis it? What is the treatment? |
|
|
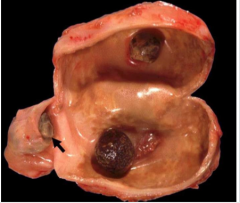
gray-tan wall thickened with fibrosis, 3 stones (one obstructing cystic duct, arrow), and
What is the diagnosis? |
Chronic cholecystitis |
|
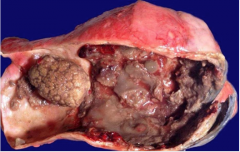
gray-tan wall thickened with fibrosis, one large and numerous small stones What is the diagnosis? |
Chronic cholecystitis |
|
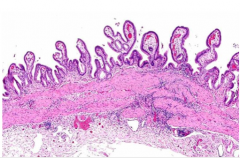
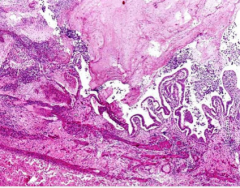
infiltration of the wall by lymphocytes, in this case with mucosal edema, congestion and hyperplasia combining to throw Diagnosis? |
Chronic cholecystitis |
|
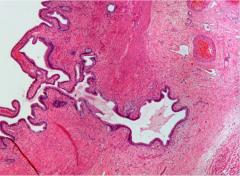
What is the term for this microscopic hernitation of gallbladder mucosa though the muscular wall? Is this cancer?
What is the diagnosis? |
Chronic cholecystitis |
|
|
What can cholestasis be the result of?
What are the intrahepatic and extra hepatic causes? |
|
|
What are these all causes of? |
Mechanical cholestasis |
|
How often do biliary complications occur after liver transplantation?
What do patients present with?
How is the diagnosis made? |

|
|
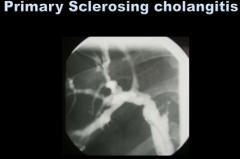
Primary sclerosing cholangitis:
Chronic cholestatic disease of the which bile ducts? Most frequent in which sex? 80% have what associated condition? Any risk for malignancy? How do you treat? Does HIV cholangiopathy present a similar finding? |
Chronic cholestatic disease of the intrahepatic and extrahepatic bile ducts |
|
|
What is the probably pathogenesis of primary sclerosing cholangitis? Associated with which disease? Age? Sex? |

|
|
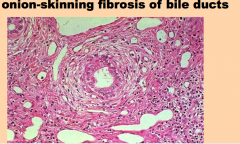
What is the diagnosis? |
Primary sclerosing cholangitis |
|
|
What three things does primary sclerosis cholangitis usually present with?
What do patients also commonly have (characteristic "beading" of bile ducts due to strictures and dilatations). |

|
|
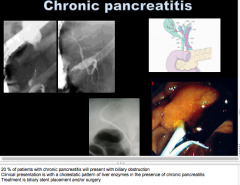
|
20% of patients with chronic pancreatitis will present with what? What is the clinical presentation? What is the treatment? |
|
|
|
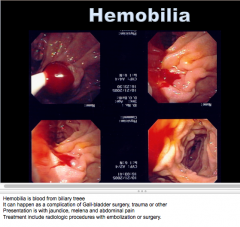
What is the term for blood from biliary tree? What are some things that can cause it? What three things do patients usually present with?
What is the treatment? |
|
|
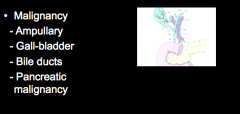
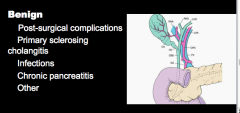
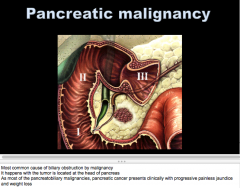
What are these all other causes of? What does malignancy usually present with? |
Mechanical cholestasis
Malignancy => progessive painless jaundice and weight loss |
|
|
Gallbladder carcinoma:
Which sex? Two races? What is the risk factor? |
|
|

Diagnosis? Type of growth pattern? |
Gallbladder carcinoma
Exophytic |
|
Diagnosis? Growth pattern? |
Gallbladder carcinoma Infiltrating |
|
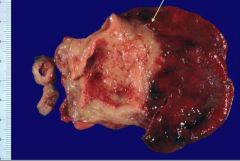
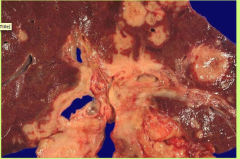
What is happening here? |
Gallbladder carcinoma invading the liver |
|
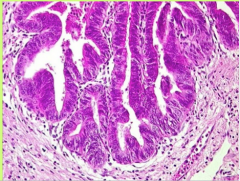
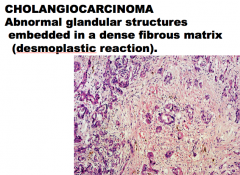
What type of cancer is gallbladder carcinoma? What is it lined by? Similar to what carcinoma? |
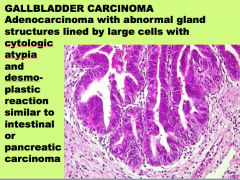
|
|
|
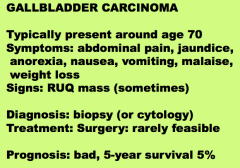
Gallbladder carcinoma:
Age of presentation? Symptoms? Sign? (sometimes)
How do you diagnose? Is surgery an option? What is the prognosis? |
|
|
What percent of all GI malignancies? Age and sex? What are some risk factors? Two things it commonly presents with? What will labs suggest? What tumor marker is sometimes present? |
3 % of all GI malignancies Most frequent in men at 50-70 years old |
|
|
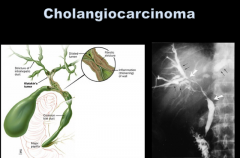
What are some common symptoms of EXTRAHEPATIC cholangiocarcinoma? Three signs? What labs will be high? |

|
|
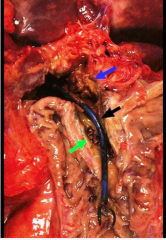
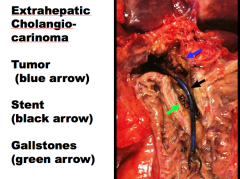
Extrahepatic cholangiocarcinoma. Identify what is indicated by the arrows. |
|
|
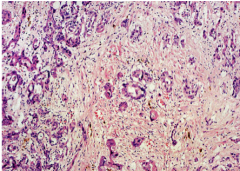
What is the disease? How do you know? |
|
|
|
What is the most common cause of biliary obstruction by malignancy? When does it occur (location)?
Two clinical presentations? |
|
|
|
Is ampullary malignancy common? Fast or slow growing? Treatment? |
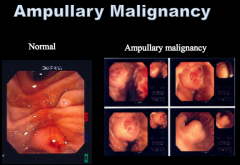
It’s not frequent |
|
|
44 yo black female, history of sickle cell disease, mother of four, history of obesity, alcohol, and tobacco use => tries weight loss
Following a meal she experiences RUQ abdominal pain radiating to her right shoulder. She developed anorexia progressing to nausea and vomiting associated with mild fever, sweating, and tachycardia. What is the most likely cause of her symptoms? |
Acute cholecystitis |
|
|
Which is not a risk factor for acute cholecystitis?
Age Alcohol use Female gender Hemolysis Obesity Prolonged fasting |
|
|
|
What do the risk factors for the development of gallstones include?
Decelerated cholesterol crystal nucleation Decreased hemoglobin breakdown Hypomotility of the gallbladder Hyposaturation of bile with cholesterol Hyposecretion of mucus in the gallbladder |
Hypomotility of the gallbladder |
|
|
Pigmented gallstones are more common in:
Alcoholics Female Hemolysis Obesity Pregnency |
Hemolysis |