![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
35 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
How do you stain a bacteria? |
1) Primary stain with crystal violet 2) Add iodine to trap stain in cells 3) Wash with EtOH 4) Counterstain with red safranin (or carbol fuchsin) |
|
|
|
Alpha Hemolytic vs Beta Hemolytic |
Alpha: partial lysis of RBCs = green rings around colonies on red backdrop; ex. S pneumo, Viridans (S mutans, S sanguis, S mitis)
Beta: complete lysis of RBCs= clear glowing halo on red backdrop; ex. S Aureus, GAS, GBS |
|
|
|
Staphylococci: Lab Identification Catalase (H2O2 -> H2O) Coagulase (Fibrinogen -> Fibrin) Capsule Hemolysis (𝜶, 𝜷, none) Urease (Urea -> Ammonia) Novobiocin/Bacitracin |
S aureus Catalase + Coagulase + Beta hemolysis Urease - Novobiocin Sensitive S epidermidis/saprophyticus Catalase + Coagulase - Non-hemolytic Urease + Novobiocin -Epi = sensitive -Saprophyiticus = resistant |
|
|
|
Golden colonies on blood agar |
S aureus |
Mannitol salt agar |
|
|
Yellow halophilic colonies on special medium |
S aureus
*All staphylococci are halophiles. (Mannitol - is pink) |
|
|
|
S aureus: Main virulence factor |
Protein A |
|
|
|
Protein A (mechanism and fuction) |
Binds Fc portion of Ig which prevents complement binding. Prevents opsonization & phagocytosis. |
|
|
|
S aureus: Location of normal flora |
Nares |
|
|
|
S aureus: Inflammatory diseases |
- Post Viral URI PNA - MCC septic arthritis - abscesses - Acute bacterial endocarditis in IVDA (Right sided= tricupsid) - MCC osteomyelitis |
|
|
|
S aureus: Toxin mediated diseases |
- Scalded skin syndrome: skin begins peeling via protease (exfoliative toxin) - Toxic Shock Syndrome: caused by prolonged presence of foreign backing. Meditated by TSST (superantigen) causing nonspecific binding of MHC-II & TCR = cytokine storm - Rapid onset food poisoning: Preformed toxins causing vommiting within 1-8 hrs of ingesting meats & creamy foods |
|
|
|
S Aureus: Diseases |
***SOFT PAINS*** Skin Infxns Osteomyelitis Food poisoning Toxic Shock syndrome Pneumonia Acute endocarditis Infective arthritis Necrotizing fasciitis Sepsis |
|
|
|
S aureus: Treatment & Resistance |
TX: Nafcillin, a penicillin ("Naf for staph")
MRSA: altered PBP (transpeptidase); Tx Vancomycin |
|
|
|
S epidermidis: Source of infection |
Normal skin flora that enters the body via adherent biofilms (polysaccharides) on indwelling catheters & prosthetic joints/valves that allows for adhesion and blocks Abx/Immune cells
**MCC Endocarditis on Artificial Heart Valves** |
|
|
|
Treatment of S Epi Endocarditis |
Vancomycin |
|
|
|
Streptococci: Lab Identification Catalase? Capsule? Hemolysis? Lancefield? Urease? Novobiocin/Bacitracin/Optochin? Special tests? |
S pyogenes (GAS): Catalase - Capsulated (hyaluronic acid = non-immunogenic) Beta hemolysis Lancefield A Urease - Bacitracin sensitive S agalactiae (GBS): Catalase - Capsulated (polysaccharide) Beta hemolysis Lancefield B Urease - Bacitracin resistant Hippurate + (hydrolyze sodium hippurate) CAMP + (Plate with S aureus = increasing zone of hemolysis) S pneumonia: Catalase - Capsulated (polysaccharide) Alpha hemolysis Lancefield None Urease - Optochin sensitive Bile soluble S viridans: Catalase - No Capsule Alpha hemolysis Lancefield None Urease - Optochin resistant Bile insoluble |
|
|
|
S Pyogenes: Pyogenic infections |
Impetigo: Honey crusted skin infxn (DDx s. aureus) Pharyngitis: Erythematous and inflamed throat (TX with Penicillin) Cellulitis/Erysipela: **MCC erythema of skin** |

|
|
|
S Pyogenes: Toxigenic infections |
Scarlet Fever: Strawberry tongue (red/swollen tongue) + Pharyngitis + Face-sparing rash Toxic Shock-like Syndrome: Superantigen mediated disease Necrotizing fasciitis: Invades the skin under fascia and spreads rapidly = surgical emergency |
|
|
|
S Pyogenes: SPE types |
Streptococcal Pyrogenic Exotoxin SPE-A: superantigen (Scarlet fever/TSLS) SPE-B: protease (nec. fasciitis) SPE-C: superantigen (Scarlet fever/TSLS) |
|
|
|
S Pyogenes: Virulence Factors |
***SMASHED*** S = Streptolysin O (beta-hemolysis; invasion) M = M protein (binds Protein H -> block opsonization by C3b; antiphagocytic/molecular mimicry) A = Anti-C5a peptidase (anti-phagocytic) S = Streptokinase (activates plasminogen -> plasmin -> fibrin breakdown; invasion) H = Hyaluronidase (invasion) E = Exotoxin D = DNAse/Dornase (invasion) |
|
|
|
S pyogenes: Rheumatic Fever |
Main Virulence Factor: M Protein (cell wall component; block opsonization by C3b & molecular mimicry to cardiac myosin) Site of attack: Mitral Valve Precipitating condition: Untreated/delayed treated pharyngitis Hypersensitive Rxn: Type 2 JONES Criteria |
|
|
|
Rheumatic Fever: JONES Criteria |
J = Joints (polyarthritis) <3 = Heart (valvular dmg leading to new murmurs, myocarditis, pericarditis) N = Nodules (subcutaneous nodules that appear on extensor surfaces of forearms or elbows/knees) E = Erythema marginatum (Rash with thick red borders) S = Sydenham's chorea (rapid, involuntary movements of hands and face) |

|
|
|
S Pyogenes: PSGN |
***"Sore throat, Face bloat, Pi$$ coke"*** Sore throat: 1-2 weeks ago Face bloat: facial edema Pi$$ coke: coke-coloured urine
Main Virulence Factor: Circulating Ag-Ab immune complex Site of attack: Glomerulus Precipitating condition: Untreated/delayed treated pharyngitis OR Impetigo Hypersensitivity Rxn: Type 3
UNLIKE Rheumatic Fever, Tx of Pharyngitis will not prevent PSGN. |
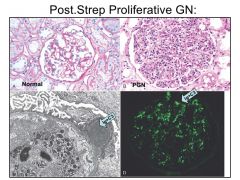
Immunofluorescence: Granular Location of IC Deposition: Subepithelial Compliment Type Activated: Classical |
|
|
S Pyogenes: ASO Titers |
ASO titers used to diagnose recent Strep infxn |
|
|
|
S agalactiae: Diseases & Pathogenesis |
**MCC Neonatal meningitis** Neonatal sepsis Pneumonia Pathogenesis: acquired during vaginal delivery Prevention: Test MOTHER rectum and vagina for colonization @ 35wks (+ = Tx MOTHER with intrapartum penicillin) |
|
|
|
Lancet shaped G+ diplococci |
S pneumoniae |
|
|
|
Bile soluble strep |
S pneumoniae |
|
|
|
S pneumonia: Disease |
**MCC of Community-acquired Pneumonia in Adults** (Lobar pneumonia with rust-colored sputum) ***Most common Bacterial cause of MOPS*** Meningitis Otitis media Pneumonia Sinusitits |
|
|
|
S pneumonia: Virulence Factors |
Capsule (polysaccharide; increased risk in splenectomy/autosplenectomy in Sickle Cell patients) IgA Protease: metallopeptidase that cleaves the Pro-Thr bond in hinge region of the heavy chain of IgA => colonize and evade |
|
|
|
S pneumonia: Treatment/Prevention |
Macrolides (ex. erythromycin) 3rd Gen Cephalosporin (ex. ceftriaxone) Vaccines: Adults = 23-valent polysaccharide vaccine; Tcell Independent response --> IgM (temporary) Children = 7-valent conjugated vaccine; Tcell Dependent response --> IgG |
|
|
|
Streptococci associated with dental carries |
S mutans & S sanguis |
|
|
|
S. Viridans: Diseases & Pathogenesis |
S sanguis invasion of blood => Subacute endocarditis in previously damaged heart valves (mitral valve) Pathogenesis: Tooth cleaning --> transient bacteremia --> adhere to fibrin-platelet aggregate by creating dextrans from glucose |
|
|
|
Enterococcus: Identification (E. Faecalis & E. Faecium) |
E. Faecalis is MC Identification: Catalase - No Capsule Non-hemolytic Lancefield None Urease - Bile insoluble Grow in 6.5% NaCl |
|
|
|
Enterococcus: Diseases |
UTIs Endocarditis Biliary tree infxn |
|
|
|
Enterococcus: VRE |
E. Faecium is most common agent of VRE VRE = nosocomial infxn that is resistant to most ABX (including Vancomycin) Tx = Linezolid or Tigecycline |
|
|
|
Staphylococci: Antibiotic sensitivity |
S auerus Novobiocin sensitive S epidermidis Novobiocin sensitive S saprophyticus Novobiocin resistant |
|