![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
154 Cards in this Set
- Front
- Back
|
What are the names of the diseases caused by a Vitamin D deficiency? |
- Osteomalacia in adults
- Rickets in children |
|
|
What causes osteomalacia (adults) and rickets (children)? Implications?
|
Vitamin D deficiency
- Defective mineralization / calcification of osteoid → soft bones that bow out - ↓ Vitamin D → ↓ serum Ca2+ → ↑ PTH → ↓ serum PO4(3-) - Hyperactivity of osteoblasts → ↑ ALP (osteoblasts require alkaline environment) |
|
|
What is the implication of osteoblast hyperactivity in Osteomalacia / Rickets?
|
Increased Alkaline Phosphatase (ALP) because osteoblasts require an alkaline environment
|
|
|
What disorder is characterized by increase in both osteoblastic and osteoclastic activity?
|
Paget Disease of Bone (Osteitis Deformans) |
|
|
What are labs found in Paget Disease of Bone (Osteitis Deformans)?
|
- Serum Ca2+, Phosphorus, and PTH are all normal
- ↑ ALP |
|
|
What is the appearance of bone in Paget Disease of Bone (Osteitis Deformans)? |
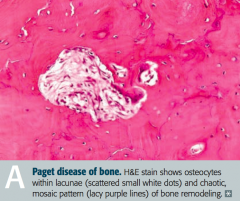
Mosaic pattern of women and lamellar bone
|
|
|
What are the potential complications of Paget Disease of Bone (Osteitis Deformans)?
|
- Long bone chalk-stick fractures |
|
|
In what disease is there a characteristic "increase in hat size"? Why?
|
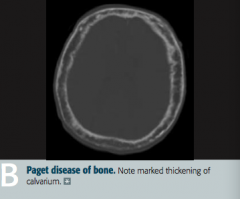
Paget Disease of Bone (Osteitis Deformans)
- Marked thickening of calvarium |
|
|
What are the stages of Paget Disease? Which cells are active during these stages?
|
- Lytic: osteoclasts
- Mixed: osteoclasts and osteoblasts - Sclerotic: osteoblasts - Quiescent: minimal osteoclast/osteoblast activity |
|
|
What can cause Osteonecrosis (avascular necrosis)?
|
Infarction of bone and marrow
- Trauma - High dose corticosteroids - Alcoholism - Sickle cell disease |
|
|
What happens in Osteonecrosis? Most common location? Why?
|
- Infarction of bone and marrow, usually very painful
- Most common site is femoral head (d/t insufficiency of medial circumflex femoral artery) |
|
|
In which bone disorders are the serum Ca2+, PO4(3-), ALP, and PTH all normal? Implications?
|
- Osteoporosis → ↓ bone mass
- Osteopetrosis → dense, brittle bones; Ca2+ ↓ in severe malignant disease |
|
|
In which bone disorders are the serum Ca2+, PO4(3-), and PTH all normal, but with an elevated ALP? Implications? |
Paget Disease → abnormal mosaic bone architecture
|
|
|
In which bone disorders are the serum Ca2+ and PO4(3-) decreased, but the ALP and PTH are elevated? Implications?
|
Osteomalacia / Rickets → soft bones
|
|
|
In which bone disorders are the serum Ca2+ and PO4(3-) increased, with a normal ALP, and decreased PTH? Implications?
|
Hypervitaminosis D (caused by over-supplementation or granulomatous disease, such as sarcoidosis)
|
|
|
In which bone disorders are the ALP and PTH elevated, with opposite levels of Ca2+ and PO4(3-)?
|
Osteitis Fibrosa Cystica
- 1° Hyperparathyroidism: ↑ Ca2+ and ↓ PO4(3-) - 2° Hyperparathyroidism: ↓ Ca2+ and ↑ PO4(3-) |
|
|
What are "brown tumors"?
|
- Bone lesion that arises in settings of excess osteoclast activity, such as hyperparathyroidism
- It is not a true neoplasm, as the term "tumor" suggests; but, it may mimic a true neoplasm - Exhibits FIBROUS REPLACEMENT of bone, with SUBPERIOSTEAL THINNING |
|
|
What are causes of 1° hyperparathyroidism?
|
- Idiopathic or parathyroid hyperplasia
- Parathyroid adenoma - Parathyroid carcinoma |
|
|
2° hyperparathyroidism is often a compensation for what?
|
End-Stage Renal Disease / ESRD
- ↓ PO4(3-) excretion and production of activated vitamin D |
|
|
What are the types of benign primary bone tumors?
|

- Giant cell tumor
- Osteochondroma (exostosis) |
|
|
What is the most common benign bone tumor? Who is most likely to get this type of tumor?
|

Osteochondroma - males <25 years old especially
|
|

What type of bone tumor should you expect in a young patient, if present in the epiphyseal end of long bones, with a "soap bubble" appearance on x-ray? Characteristics?
|

Giant Cell Tumor
- Benign primary bone tumor - Locally aggressive, often around the knee - Multi-nucleated giant cells |
|
|
What type of bone tumor should you expect in a male <25 years that appears as an outgrowth from mature bone with a cartilaginous cap? Characteristics?
|

Osteochondroma (Exostosis)
- Most common benign tumor - Rarely transforms to chondrosarcoma |
|
|
What are the types of malignant primary bone tumors?
|
- Osteosarcoma (osteogenic sarcoma)
- Ewing sarcoma - Chondrosarcoma (Multiple Myeloma) |
|
|
What are the most common 1° malignant bone tumors?
|
1. Multiple Myeloma
2. Osteosarcoma (Osteogenic Sarcoma) |
|
|
What are the most likely malignant bone cancers by age?
|
- Boy < 15 years: Ewing Sarcoma
- 10-20 years: Osteosarcoma (1°) - 30-60 years: Chondrosarcoma - >65 years: Osteosarcoma (2°) |
|
|
What are the most common locations for the different malignant bone tumors?
|
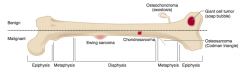
- Osteosarcoma: metaphysis of long bones, often around knee
- Ewing Sarcoma: diaphysis of long bones, pelvis, scapula, ribs - Chondrosarcoma: pelvis, spine, scapula, humerus, tibia, or femur |
|
|
Which type of bone pathology is associated with an elevation of the periosterum? What is the term for this?
|
Osteosarcoma
- Elevation of the periosterum = Codman Triangle |
|
|
Which type of bone pathology is associated with a "sunburst pattern" on x-ray?
|
Osteosarcoma
|
|
|
What are the predisposing factors for Osteosarcoma?
|
- Paget disease of bone
- Bone infarcts - Radiation - Familial retinoblastoma - Li-Fraumeni syndrome (germline p53 mutation) |
|
|
How do you treat Osteosarcoma?
|
Surgical en block resection (with limb salvage) and chemotherapy |
|
|
Which bone pathology has an "onion skin" appearance?
|
Ewing Sarcoma
|
|
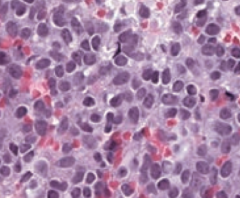
Which bone pathology is associated with anaplastic, malignant small blue cells?
|
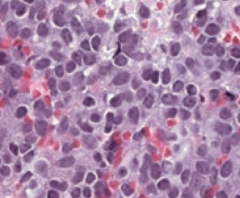
Ewing Sarcoma
|
|
|
Which genetic change is associated with Ewing Sarcoma?
|
t(11;22) translocation |
|
|
How do you treat Ewing Sarcoma?
|
Chemotherapy (responsive)
|
|
|
Which bone pathology typically appears as an expansile glistening mass within the medullary cavity?
|
Chondrosarcoma
|
|
|
What are the characteristics of Osteosarcoma (when is it more common? predisposing factors? location? signs on labs/imaging? treatment?)
|
- 2nd most common 1° malignant bone tumor |
|
|
What are the characteristics of Ewing Sarcoma (when is it more common? predisposing factors? location? signs on labs/imaging? treatment? other?)
|
- Boys < 15 years old
- Predisposing factors: t(11;22) translocation - Location: diaphysis of long bones, pelvis, scapula, ribs - Signs: anaplastic small blue cell malignant tumor, "onion skin" appearance in bone - Treatment: responsive to chemotherapy - Extremely aggressive w/ early metastases |
|
|
What are the characteristics of Chondrosarcoma (when is it more common? location? signs on labs/imaging? other?)
|
- Men 30-60 years old
- Location: usually in pelvis, spine, scapula, humerus, tibia, femur - Signs: expansile glistening mass within the medullary cavity - Rare, malignant, cartilaginous tumor - May be 1° origin or from osteochondroma |
|
|
What is the cause of Osteoarthritis vs Rheumatoid Arthritis?
|
- OA: mechanical - joint wear and tear destroys articular cartilage |
|
|
What are the findings in joints with Osteoarthritis vs Rheumatoid Arthritis?
|
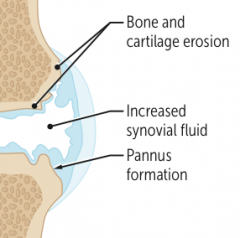
- OA: subchondral cysts, sclerosis, osteophytes (bone spurs), eburnation (polished, ivory-like appearance), Heberden nodes (DIP), and Bouchard nodes (PIP); no MCP involvement
- RA: pannus formation in joints (MCP and PIP); subcutaneous rheumatoid nodules (fibrinoid necrosis), ulnar deviation of fingers, subluxation, Baker cyst (in popliteal fossa); no DIP involvement |
|
|
What joints are classically affected by Osteoarthritis vs Rheumatoid Arthritis?
|
- OA: DIP and PIP (no MCP); weight-bearing joints
- RA: MCP and PIP (no DIP) |
|
|
What are the predisposing factors for Osteoarthritis vs Rheumatoid Arthritis?
|
- OA: age, obesity, joint deformity, trauma
- RA: female, 80% are + for rheumatoid factor (anti-IgG Ab); anti-cyclic citrullinated peptide Ab is more specific; strongly associated with HLA-DR4 |
|
|
What is the classic presentation of Osteoarthritis vs Rheumatoid Arthritis?
|
- OA: pain in weight-bearing joints after use (eg, at end of day), improves with rest; knee cartilage loss begins medially (bowlegged); non-inflammatory; no systemic symptoms
- RA: morning stiffness >30 minutes improves with use; symmetric joint involvement; systemic symptoms (fever, fatigue, pleuritis, and pericarditis) |
|
|
What is the treatment for Osteoarthritis vs Rheumatoid Arthritis?
|
- OA: NSAIDs, intra-articular glucocorticoids
- RA: NSAIDs, glucocorticoids, disease-modifying agents (methotrexate, sulfasalazine, TNF-α inhibitors) |
|
|
Which type of bone pathology is associated with subchondral cysts?
|
Osteoarthritis
|
|
|
Which type of bone pathology is associated with sclerosis?
|
Osteoarthritis
|
|
|
Which type of bone pathology is associated with pannus formation in the joints (MCP, PIP)?
|
Rheumatoid Arthritis
|
|
|
Which type of bone pathology is associated with osteophytes (bone spurs)?
|
Osteoarthritis
|
|
|
Which type of bone pathology is associated with ulnar deviation of the fingers?
|
Rheumatoid Arthritis
|
|
|
Which type of bone pathology is associated with subluxation?
|
Rheumatoid Arthritis
|
|
|
Which type of bone pathology is associated with eburnation? What does this term mean?
|
Osteoarthritis - eburnation means polished, ivory-like appearance of the bone
|
|
|
Which type of bone pathology is associated with Baker cysts? Location?
|
Rheumatoid Arthritis - Baker cysts in popliteal fossa
|
|
|
Which type of bone pathology is associated with Heberden nodes and Bouchard nodes? Location?
|
Osteoarthritis
- Heberden nodes: DIP - Bouchard nodes: PIP |
|
|
What type of antibodies are associated with Rheumatoid Arthritis? Which is more specific?
|
- Rheumatoid Factor (anti-IgG antibody)
- Anti-cyclic citrullinated peptide antibody (more specific) |
|
|
What HLA is Rheumatoid Arthritis associated with?
|
HLA-DR4
|
|
|
Which type of arthritis has pain in the weight bearing joints after use (eg, at the end of the day)?
|
Osteoarthritis
|
|
|
Which type of arthritis has morning stiffness lasting >30 minutes that improves with use?
|
Rheumatoid Arthritis
|
|
|
Which type of arthritis has cartilage loss that begins medially?
|
Osteoarthritis
|
|
|
How do you treat Osteoarthritis?
|
- NSAIDs
- Intra-articular glucocorticoids |
|
|
How do you treat Rheumatoid Arthritis?
|
- NSAIDs
- Glucocorticoids - Disease-modifying agents: methotrexate, sulfasalazine, TNF-α inhibitors |
|
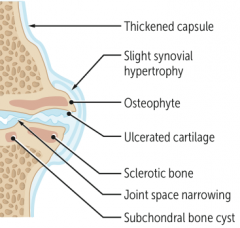
What type of arthritis has these features?
|
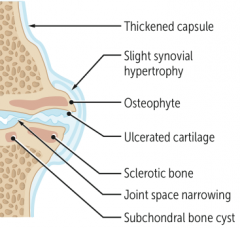
Osteoarthritis
|
|
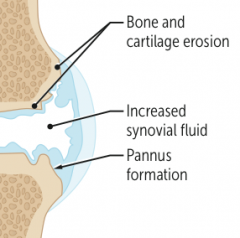
What type of arthritis has these features?
|
Rheumatoid Arthritis
|
|

What type of arthritis has this appearance?
|

Osteoarthritis
- X-rays of the knee show joint space narrowing and sclerosis |
|

What type of arthritis has this appearance?
|

Rheumatoid Arthritis
- Note boutonnière deformities of PIP joints with ulnar deviation |
|
|
What disorder causes destruction of exocrine glands via an auto-immune process? Which glands are especially affected? |
Sjögren Syndrome
- Especially affects lacrimal and salivary |
|
|
Which disorder causes xerophthalmia, xerostomia, and bilateral parotid gland enlargement? What do these terms mean?
|
Sjögren Syndrome
- Xerophthalmia: ↓ tear production and subsequent corneal damage - Xerostomia: ↓ saliva production |
|
|
What is the term for decreased tear production and subsequent corneal damage?
|
Xerophthalmia
|
|
|
What is the term for decreased saliva production?
|
Xerostomia
|
|
|
What antibodies are seen in Sjögren Syndrome?
|
Anti-nuclear antibodies: SS-A (anti-Ro) and/or SS-B (anti-La)
|
|
|
What can cause Sjögren Syndrome?
|
- Can be primary
- Can be secondary, associate with other auto-immune disorders (eg, rheumatoid arthritis) |
|
|
What are the potential consequences of Sjögren Syndrome?
|
- Dental caries |
|
|
What are the findings of Sjögren Syndrome?
|
- Xerophthalmia (↓ tear production and subsequent corneal damage)
- Xerostomia (↓ saliva production) - Presence of anti-nuclear antibodies: SS-A (anti-Ro) and/or SS-B (anti-La) - Bilateral parotid enlargement |
|
|
What are the characteristic findings of gout?
|
Acute inflammatory monoarthritis
|
|
|
What causes gout?
|
Precipitation of monosodium urate crystals in joints
Associated with hyperuricemia, which can be caused by: - Underexcretion of uric acid (90% of patients) - largely idiopathic, can be exacerbated by certain medications (eg, thiazide diuretics) - Overproduction of uric acid (10% of patients) - Lesch-Nyhan syndrome, PRPP excess, ↑ cell turnover (eg, tumor lysis syndrome), von Gierke disease |
|
|
What can cause underexcretion of uric acid? How often is this the cause of gout?
|
- Largely idiopathic
- Can be exacerbated by certain medications (eg, thiazide diuretics) - 90% of patients |
|
|
What can cause overproduction of uric acid? How often is this the cause of gout?
|
- Lesch-Nyhan syndrome |
|
|
What is the characteristic of the monosodium urate crystals found in gout?
|
- Needle shaped
- Negatively birefringent (yellow under parallel light, blue under perpindicular light) |
|
|
How does gout typically present?
|

- Asymmetric joint distribution (typically a monoarthritis) |
|
|
What are tophi? Where do they form?
|
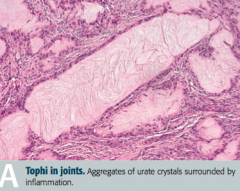
Tophus (deposit of crystalline uric acid and other substances at the surface of joints or in skin or cartilage)
- Often on external ear, olecranon bursa, or Achilles tendon |
|
|
When do acute attacks of gout often occur? Why?
|
- After a large meal
- After alcohol consumption: alcohol metabolites compete for same excretion sites in kidney as uric acid, causing ↓ uric acid secretion and subsequent buildup in blood |
|
|
What are the treatments for acute attacks of gout?
|
- NSAIDs (eg, indomethacin)
- Glucocorticoids - Colchicine |
|
|
What are the chronic preventive treatments for gout?
|
Xanthine oxidase inhibitors (Allopurinal and Febuxostat)
|
|
|
What is the mechanism of Allopurinol and Febuxostat? Uses?
|
Xanthine Oxidase inhibitors - used for chronic / preventative treatment of gout
|
|
|
What kind of crystals cause pseudogout?
|
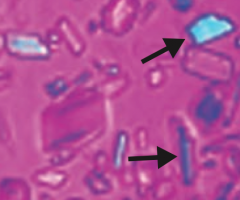
Calcium pyrophosphate crystals - basophilic, rhomboid crystals that are weakly birefringent (blue when parallel to light)
|
|
|
What is the typical presentation of pseudogout? Who is more often affected?
|
- Pain and effusion in joint
- Usually affects large joints (classically the knee) - >50 years old, both sexes affected equally |
|
|
What diseases are associated with pseudogout?
|
- Hemochromatosis
- Hyperparathyroidism - Hypoparathyroidism |
|
|
How does pseudogout appear on x-ray? |
Chondrocalcinosis - calcium pyrophosphate cyrstals within joint space
|
|
|
How do you treat pseudogout?
|
- NSAIDS for sudden, severe attacks
- Steroids - Colchicine |
|
|
How do gout and pseudogout compare in terms of the birefringence of their crystals?
|
- Gout: crystals are yellow when parallel to light
- Pseudogout: crystals are blue when parallel to light |
|
|
What are the most common causes of infectious arthritis?
|
- S. aureus
- Streptococcus - Neisseria gonorrhoeae |
|
|
In a sexually active patient, with asymmetric migratory arthritis, what should you consider as a cause?
|
Neisseria gonorrhoeae: gonococcal arthritis (STD)
|
|
|
What are the characteristics of infectious arthritis?
|
Joint is swollen, red, and painful
|
|
|
What are the specific signs of Gonococcal Arthritis?
|
STD: |
|
|
What is the term for arthritis without rheumatoid factor (anti-IgG Ab)? What is it associated with?
|
Seronegative Spondyloarthropathies:
- Strong association with HLA-B27 |
|
|
What are the types of Seronegative Spondyloarthropathies?
|
PAIR: |
|
|
What are the characteristics of arthritis in a patient with psoriasis?
|

- Joint pain and stiffness |
|
|
How common is arthritis in patients with psoriasis?
|
1/3 of patients with psoriasis
|
|
|
What is the name of the chronic inflammatory disease of the spine and sacroiliac joints? Implications?
|
Ankylosing Spondylitis
- Ankylosis (stiff spine d/t fusion of joints) - Uveitis - Aortic regurgitation |
|

In what condition do you see "bamboo spine"? Cause?
|

Ankylosing spondylitis
- Vertebral fusion |
|
|
What are the characteristics of arthritis in patients with Inflammatory Bowel Disease?
|
Crohn disease and ulcerative colitis are often accompanied by ankylosing spondylitis or peripheral arthritis
|
|
|
What is the classic triad of findings in Reactive Arthritis (Reiter Syndrome)?
|
"Can't see, can't pee, can't bend my knee":
- Conjunctivitis (and anterior uveitis) - Urethritis - Arthritis |
|
|
What is Reactive Arthritis (Reiter Syndrome) in response to?
|
Post-GI (Shigella, Salmonella, Yersinia, Campylobacter) or Chlamydia infections |
|
|
What disease has the classic presentation of rash, joint pain, and fever?
|
Systemic Lupus Erythematosus
|
|
|
What mnemonic can help you remember the characteristics of Systemic Lupus Erythematosus?
|
RASH OR PAIN:
- Rash (malar or discoid) - Arthritis - Soft tissues / Serositis - Hematologic disorders (eg, cytopenias) - Oral / nasopharyngeal ulcers - Renal disease, Raynaud phenomenon - Photosensitivity, Positive VDRL/RPR - Anti-nuclear antibodies - Immunosuppressants - Neurologic disorders (eg, seizures, psychosis) |
|
|
What are the common causes of death in patients with Systemic Lupus Erythematosus?
|
- Cardiovascular disease
- Infections - Renal disease |
|
|
What kind of cardiac disease is associated with Systemic Lupus Erythematosus?
|
Libman-Sacks Endocarditis: wart-like vegetations on boths ides of valve
|
|
|
What kind of renal disease is associated with Systemic Lupus Erythematosus?
|
Lupus Nephritis (Type III hypersensitivity reaction):
- Nephritic: diffuse proliferative glomerulonephritis - Nephrotic: membranous glomerulonephritis |
|
|
What kinds of antibodies are associated with Systemic Lupus Erythematosus?
|
- Anti-nuclear antibodies (ANA)
- Anti-dsDNA antibodies - Anti-Smith antibodies - Anti-histone antibodies - Anti-cardiolipin antibodies |
|
|
What antibody is sensitive, but not specific for Systemic Lupus Erythematosus?
|
Anti-nuclear antibodies (ANA)
|
|
|
What antibody is specific and indicates a poor prognosis (renal disease) for Systemic Lupus Erythematosus?
|
Anti-dsDNA antibodies
|
|
|
What antibody is specific, but does not offer prognostic information?
|
Anti-Smith antibodies (directed against snRNPs)
|
|
|
What antibody is sensitive for drug-induced lupus?
|
Anti-histone antibodies
|
|
|
What antibody shows false positives for patients with syphilis and prolongs the PTT in patients with Systemic Lupus Erythematosus? Implications?
|
Anti-Cardiolipin antibody
- Pardoxically prolonged PTT, increases risk for arteriovenous thromboembolism |
|
|
What antibody increases the risk of arteriovenous thromboembolism?
|
Anti-cardiolipin antibodies |
|
|
How is complement affected in Systemic Lupus Erythematosus?
|
Decreased C3, C4, and CH50 due to immune complex formation
|
|
|
How do you treat patients with Systemic Lupus Erythematosus?
|
- NSAIDs
- Steroids - Immunosuppressants - Hydroxychloroquine |
|
|
What mnemonic can help you remember the characteristics of Systemic Lupus Erythematosus?
|
RASH OR PAIN:
- Rash (malar or discoid) - Arthritis - Soft tissues / Serositis - Hematologic disorders (eg, cytopenias) - Oral / nasopharyngeal ulcers - Renal disease, Raynaud phenomenon - Photosensitivity, Positive VDRL/RPR - Anti-nuclear antibodies - Immunosuppressants - Neurologic disorders (eg, seizures, psychosis) |
|
|
What disease is characterized by immune-mediated, widespread non-caseating granulomas and elevated serum ACE levels?
|
Sarcoidosis
|
|
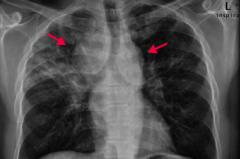
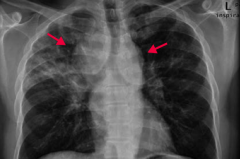
If your patient is a black female with enlarged lymph nodes and bilateral hilar adenopathy or reticular opacities incidentally found on CXR, what diagnosis should you consider? Why?
|
Sarcoidosis
- CXR shows bilateral suprahilar adenopathy (arrows) and right upper lung reticular opacity (often incidental findings on CXR) - Common in black females - Often asymptomatic except for enlarged lymph nodes |
|
|
What is sarcoidosis associated with?
|
- Restrictive lung disease (interstitial fibrosis) |
|
|
What are the characteristics of the granulomas in Sarcoidosis?
|
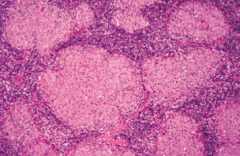
- Non-caseating
- Epithelioid - Contain Schaumann and asteroid bodies |
|
|
What electrolyte abnormality is associated with sarcoidosis? Cause?
|
Hypercalcemia - due to ↑ 1α-hydroxylase-mediated Vitamin D activation in macrophages
|
|
|
How do you treat sarcoidosis?
|
Steroids
|
|
|
What are the characteristics of Sarcoidosis?
|
- Immune-mediated, widespread non-caseating granulomas |
|
|
What diagnosis should you consider in a patient with pain and stiffness in their shoulders and hips, with fever, malaise, and weight loss?
|
Polymyalgia Rheumatica
|
|
|
What symptoms occur in patients with Polymyalgia Rheumatica?
|
- Pain and stiffness in shoulders and hips
- Fever, malaise, weight loss - No muscular weakness |
|
|
Who is more likely to have Polymyalgia Rheumatica?
|
- More common in women >50 years old
- Associated with Temporal (Giant Cell) Arteritis |
|
|
What are the lab findings in a patient with Polymyalgia Rheumatica?
|
- ↑ ESR
- ↑ C-reactive protein - Normal CK |
|
|
How do you treat a patient with Polymyalgia Rheumatica?
|
Rapid response to low-doe corticosteroids
|
|
|
Which disease is most commonly seen in females 20-50 years old with chronic widespread musculoskeletal pain, stiffness, paresthesias, poor sleep, and fatigue? How should you treat?
|
Fibromyalgia
- Regular exercise - Antidepressants (TCAs, SNRIs) - Anti-convulsants |
|
|
What are the symptoms of Fibromyalgia?
|
- Chronic, widespread musculoskeletal pain
- Associated with stiffness, paresthesias, poor sleep, and fatigue - Most commonly in females 20-50 years old |
|
|
How do you treat Fibromyalgia?
|
- Regular exercise
- Antidepressants (TCAs, SNRIs) - Anti-convulsants |
|
|
What is the cause of progressive symmetric proximal muscle weakness, characterized by endomysial inflammation with CD8+ T cells? Most common location?
|
Polymyositis - most often involves shoulders
|
|
|
What disease can cause present similarly to polymyositis (progressive symmetric proximal muscle weakness) with the addition of malar rash (similar to SLE), Gottron papules (on knuckles), heliotrope (erythematous periorbital) rash, "shawl and face" rash, and/or "mechanic's hands" appearance? What type of inflammation causes this presentation?
|

Dermatomyositis: perimysial inflammation and atrophy with CD4+ T cells |
|
|
How does Polymyositis compare to Dermatomyositis in terms of location of symptoms? |

- Polymyositis: symmetric, progressive, proximal muscle weakness, especially in shoulders |
|
|
What type of inflammation is responsible for Polymyositis and Dermatomyositis?
|
- Polymyositis: endomysial inflammation with CD8+ T cells |
|
|
What lab findings are associated with polymyositis and dermatomyositis? |
- ↑ CK |
|
|
How do you treat a patient with polymyositis or dermatomyositis?
|
Steroids
|
|
|
What is the pathophysiology responsible for Myasthenia Gravis?
|
Auto-Abs to post-synaptic ACh receptor
|
|
|
What are the symptoms of Myasthenia Gravis?
|
- Ptosis
- Diplopia - Weakness - Worsens with muscle use |
|
|
What is Myasthenia Gravis associated with?
|
- Thymoma
- Thymic hyperplasia |
|
|
How do you treat Myasthenia Gravis?
|
AChE Inhibitor - reverses symptoms
|
|
|
Which neuromuscular junction disease is more rare than Myasthenia Gravis?
|
Lambert-Eaton Myasthenic Syndrome
|
|
|
What is the pathophysiologic cause of Lambert-Eaton Myasthenic Syndrome?
|
Auto-antibodies to presynaptic Ca2+ channels → ↓ ACh release
|
|
|
What are the symptoms of Lambert-Eaton Myasthenic Syndrome?
|
- Proximal muscle weakness
- Autonomic symptoms (dry mouth, impotence) - Improves with muscle use |
|
|
What is Lambert-Eaton Myasthenic Syndrome associated with?
|
Small cell lung cancer
|
|
|
What is the effect of AChE inhibitors in patients with Lambert-Eaton Myasthenic Syndrome?
|
Minimal effect
|
|
|
What are the two neuromuscular junction diseases and how do they compare in terms of the cause?
|
- Myasthenia Gravis: auto-Abs to post-synaptic ACh receptor
- Lambert-Eaton Myasthenic Syndrome: auto-Abs to presynaptic Ca2+ channel which decreases ACh release |
|
|
What are the two neuromuscular junction diseases and how do they compare in terms of the symptoms they cause?
|
- Myasthenia Gravis: ptosis, diplopia, weakness, worsens with muscle use
- Lambert-Eaton Myasthenic Syndrome: proximal muscle weakness, autonomic symptoms (dry mouth, impotence), improves with muscle use |
|
|
What are the two neuromuscular junction diseases and how do they compare in terms of associated conditions?
|
- Myasthenia Gravis: thymoma, thymic hyperplasia
- Lambert-Eaton Myasthenic Syndrome: small cell lung carcinoma |
|
|
If a patient has a suspicious "mass" at a site of trauma to their bone/muscle, what should you think of?
|
Myositis Ossificans: metaplasia of skeletal muscle to bone (muscle becomes calcified) following muscular trauma
|
|
|
Where is Myositis Ossificans more commonly found?
|
Most often in upper or lower extremity
|
|
|
What are the clinical findings in a patient with Myositis Ossificans?
|

May present as a suspicious mass at a site of known trauma or as incidental finding on radiography
|