![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
50 Cards in this Set
- Front
- Back
|
Calculate SV |
LVEDV-LVESV |
|
|
Calculate EF |
Ejection fraction: (SV/LVEDV)x100 |
|
|
Calculate cardiac output |
Q= SVxHR |
|
|
myocardial oxygen consumption estimated by.. |
RPP= (HRxSBP)/100 rate pressure product |
|
|
Hemodynamic Response RPP |
High > 300High Intermediate 250 - 300Intermediate 200 - 250Low Intermediate 150 - 200Low 100 - 150 |
|
|
Arteries |
deliver blood |
|
|
Arterioles |
Resistance vessels - another name for arterioles due to their ability to vasodilate and vasoconstrict; changing diameter allows them to control the flow of blood |
|
|
Capillaries |
Exchange vessels – all exchange of oxygen and carbon dioxide occur here |
|
|
Venules |
made of smooth mm, affect capillary pressure, dump into veins |
|
|
veins |
Capacitance vessels - another name for veins, owing to their distensibility, which enables them to pool large volumes of blood and become reservoirs for blood |
|
|
Hematocrit? in men.. in women |
the ratio of blood cells to total blood volume, expressed as a percentage Adult males: 42-54%Adult females: 38-46% |
|
|
Mean Arterial Pressure (MAP) |
MAP = (PP/3) + DBP2 (5th Korotkoff sound) MAP = (PP/2) + DBP1 (4th Korotfoff sound) Determines organ and tissue perfusion |
|
|
Total Peripheral Resistance (TPR) |
Q = MAP/TPR |
|
|
medulla oblongata has 3 control centers which are |
vasomotor center cardiac accelerator center cardiac inhibitor center |
|
|
vasomotor center responsible for |
vasodilation of skeletal muscle arterioles vasoconstriction of visceral arterioles (sympathetic outflow, accelerator N) |
|
|
Cardio accelerator center and cardio inhibitor center work with... |
CA: inc. heart rate and contractility CI: heart dec. and so does contractility (parasympathetic outflow, vagus N) |
|
|
Anatomical Sensors and FactorsAffecting Control |
a. Higher brain centersb. Systemic receptorsa. Baroreceptorsb. Stretch receptorsc. Chemoreceptorsd. Muscle joint receptors |
|
|
high brain centers |
cerebral cortex: emotional factors, motor cortexhypothalamus: input from cortex, body temp |
|
|
chemoreceptors |
inc. in CO2 pressure, inc. in H ions, dec. in pressure of O2 leads to general vasoconstriction |
|
|
Muscle receptors |
mechanical: inc. movement leads to inc. sympathetic outflow metabolic: inc. activity causes in. in metabolites which leads to inc. in sympathetic flow |
|
|
systemic receptors |
Baroreceptors (aortic and carotid bodies): respond to inc. MAP leads to inc. parasymp. outflow and dec. symp. outflow Stretch receptors (R atrium): inc. venous return leads to inc. symp. outflow |
|
|
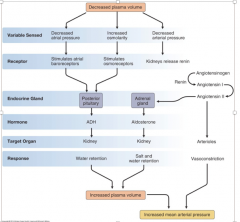
Neurohormonal Control |
• Epinephrine/Norephinephrine• Alosterone/ADH |
|
|
memorize this hahahaha |
|
|
|
Fick equation |
Q = (VO2/a-vO2diff) |
|
|
what is inotropic and what is chronotropic |
Stroke volume.. heart rate |
|
|
VO2 max |
greatest amount of oxygen that the body can take in,transport, and utilize during heavy exercise VO2max= (HR max) * (SVmax) * (a-vO2 diff max) |
|
|
diastole systole |
filling phase (relaxation) ejection phase (contraction) |
|
|
fluids move from ____ to _____ |
high pressure to low pressure |
|
|
Primer pump power pump |
atrium ventricle |
|
|
the pressure changes in the _____ side of the heart are greater than _____ side of the heart but the volume of blood is the _________ |
left, right, same volume |
|
|
why does left have greater pressure |
volume of blood taken to greater distances than right |
|
|
why must volumes stay the same with left and right |
otherwise there would be a backdrop of blood in one of the circuits. Leads to congestive heart failure
|
|
|
as the electrical impulse passes from atrium to ventricle there is approx. ____ delay allowing for greater filling time for the ventricle |
0.10 sec |
|
|
blood moves passively to ventricle and fills_____ but contracts to top it off to fill with ____ |
70-75%, 100% |
|
|
EDV |
end diastolic volume: amt. of blood in each vent. at the end of vent. diastole |
|
|
ESV |
end systolic volume: amt. of blood remaining in each vent. at the end of vent. systole |
|
|
Ejection fraction definition |
percentage of EDV represented by SV |
|
|
cardiac reserve |
difference btween resting and maximal CO |
|
|
Factors controlling SV |
For EDV: filling time, venous return For ESV: preload, contractility, afterload |
|
|
Factors affecting EDV: inc. _____ decreases _____ |
heart rate, filling time |
|
|
During exercise venous return is increased by 3 principle mechanisms |
vasoconstriction: dec. vol. capacity of the veins to store blood>>> movement back to the heart via symp. constriction of smooth mm in the veins Muscle pump: one way valves in the veins, rhythmic muscle contractions facilitate movement of blood back to the heart respiratory pump: rhythmic pattern of breathing also acts as a mechanical pump inc. thoracic pressure>>> inc. abdominal pressure, blood moves from high to low pressure |
|
|
Preload |
degree of stretching experienced during ventricular diastole |
|
|
length tension relationship |
stretching beyond its optimal length generally does not occur bc ventricular expansion is limited by myocardial CT, fibrous skeleton and pericardium |
|
|
frank starling mechanism |
inc. blood in the ventricles causes a stronger ventricular contraction to inc. the amt. ejected "more in more out" |
|
|
Contractility changed in contractility caused by.. |
amt. of force produced by each contraction 1. autonomic stimulation>> symp. stimulation inc. HR (NE and E stimulate cardiac muscle) 2. hormones>> E, NE, glucagons and thyroid hormones inc. contractility 3. changes in ion concentration: hypercalcemia: inc. cardiac muscle excitability hypocalcemia: dec. cantractation hyperkalemia: depol. and inhibition of repol. therefore contractions become weak and irregular hypokalemia: hyperpol. and HR and BP dec. |
|
|
afterload |
amt. of tension the contracting vent. must produce the force necessary to force open the semilunar valve and eject blood. inc. in afterload= inc. isovolumetric contraction dec. duration of ventricular ejection inc. ESV and dec. SV |
|
|
Factors affecting HR: |
1) autonomic NS: symp. inc. HR; parasymp. dec. HR 2) hormones: E, NE, thyroid hormone inc. HR and contractility 3) changes in ion concentration: dec. K produces hyperdepol and dec. HR, changes in Ca have more important effects on contractility 4) changes in body temp-- dec. temp= dec. HR (depol. of SA node) |
|
|
mammalian dive reflex |
massive vasoconstriction and HR < 46 bpm (parasymp) inc. in temp>> inc. sweating and dec. plasma vol. (dec. SV>> inc. HR) |
|
|
how to find TPR why important |
viscosity* total length/ radius^4 total length only changes with age so only viscosity changes really... TPR goes up with viscosity and total length get blood at high speeds with tissues that need it (vasodilate w/ tissues that need it most, vasoconstrict w/ tissues that dont need it) |
|
|
rise in HR after 45 min causes___ |
dec. SV |