Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
65 Cards in this Set
- Front
- Back
|
Secondary inputs to the vetibular system and their influence:
1: visual 2: cerebellum |
1) important but is not primary because there is lots of movement in the world
2) has motor memory which helps you know how much to correct a motor perturbation |
|
|
Utricle and saccule purpose:
|
sense of gravity and linear translation
|
|
|
1) Hair cells depolarize when:
2) Hiar cells hyperpolarize when |
1) they tilt toward the kinocilium
2) they tilt away from the kinocilium |
|
|
When you look left the hair cells on your left ____1____ and the hair cells on the right ____2____
|
1) depolarize
2) hyperpolarize |
|
|
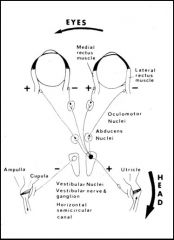
Be able to describe the wiring of the eyes to the inner ears. This includes excitatory and inhibitory connections, as well as the abducens and oculomotor nuclei.
|

When you turn your heal to the right, in order to keep stale gaze, the right sizes of your eyes (medial on the right and lateral on the left) must be stimulated. The left sides must be inhibited. Signals to the lateral side (both) must go through both the vestibular and abducens nucleui while signals to the medial side (nasal) must go through the vestibular and oculomotor nuclei.
|
|
|
Signals to the lateral side of the eye (both) must go through both the:
|
vestibular and abducens nucleui
|
|
|
signals to the medial side (nasal) of the eye must go through the:
|
vestibular and oculomotor nuclei.
|
|
|
If the eyes become uncoupled in their movements what should you do?
|
Neuro referral because the problems is central.
|
|
|
Utricle is in what plane?
|
axial
|
|
|
saccule is in what plane?
|
saggital
|
|
|
Left labyrinth activation causes what reaction contralaterally and ipsilaterally extensors
|
1) excitatory to contralateral extensory
2) inhibitory to ipsilateral extensors |
|
|
Where does your information come from in examining a dizzy patient?
|
history 70%
physical 10-20% Lab tests 10-20% |
|
|
Vertigo:
1) symptoms 2) findings 3) causes |
1) true sensations of disturbed motion
2)Nystagmus 3) 95% peripheral (labyrinthine or non-retrolabrynthine) or 5% CNS |
|
|
Dysequilibrium
1) symptoms 2) findings 3) causes |
1) Illusions of spatial disorientation or incoordination
2) no nystagmus 3) Systemis dosirder or vestibular CNS diseae |
|
|
Can we help:
1) vertigo 2) dysequilibrium |
1) yes
2) no |
|
|
Differentiation of Central vs. peripheral Dizziness:
Hallucinations of movement? |
Peripheral: definite
Central:less definite |
|
|
Differentiation of Central vs. peripheral Dizziness:
Onset |
Peripheral: paroxysmal
Central: usually constant |
|
|
Differentiation of Central vs. peripheral Dizziness:
Intensity |
Peripheral: usually severe
Central: seldom severe |
|
|
Differentiation of Central vs. peripheral Dizziness:
Duration |
Peripheral: seconds to hours
Central: up to days or weeks NO-ONE has real vertigo for hours |
|
|
Differentiation of Central vs. peripheral Dizziness:
Influenced by headposition? |
Peripheral: frequently
Central: seldom |
|
|
Differentiation of Central vs. peripheral Dizziness:
Nystagmus |
Peripheral: Present
Central: Present of absent |
|
|
Differentiation of Central vs. peripheral Dizziness:
ANS symtoms |
Peripheral:Definite
Central: Absent usually |
|
|
Differentiation of Central vs. peripheral Dizziness:
Tinnitus |
Peripheral:Frequent
Central:Seldom |
|
|
Differentiation of Central vs. peripheral Dizziness:
deafness |
Peripheral:Frequent
Central:Seldom |
|
|
Differentiation of Central vs. peripheral Dizziness:
Disturbances of conciousness |
Peripheral:NEVER
Central:FREQUENT |
|
|
Differentiation of Central vs. peripheral Dizziness:
Other neuro signs |
Peripheral:absent
Central: often present |
|
|
Which is true vertigo, central or peripheral?
|
Peripheral
|
|
|
Physical Exam for Vertigo (6)
|
Oculomotor Exam
Spontanous Nystagmus Evoked Nystagmus (Gaze-positional) VOR triad (headshake, head thrust, DVA) Cerebellar/coordination tests Posture and gait test |
|
|
Three tools for physical exam and why we use them
|
1) Frenzel lenses- take away vison but let us observe eyes
2) 128Hz tunig fork for vibrotactile sense in the feet (maybe the imbalance is due to spinal cord) 3) 4" cushion tests vestibular sense by taking away proprioception |
|
|
When you see no nystagmus with eyes open, but nystagmus with frenzel lenses, then think....
|
Vestibular neuritis (8th nerve viral infection)
|
|
|
1) Define gaze nystagmus
2) If you see Gaze nystagmus what is the most likley diagnosis? 3) what is a possible other diagnosis? |
1) direction of nystagmus changes with direction of gaze
2) EtOH intoxication 3) Cerebellar problem |
|
|
Saccades should have 4 characteristics
|
Cojugate
Accurate Fast Minimal Deay |
|
|
If a person has:
1) slow saccades--Dx? 2) other saccadic problem |
1)MS
2) brain problem |
|
|
Internuclear Opthalmoplegia
|
One eye drags because of uncoupling of saccadic reflex (indicates a CNS injury)
|
|
|
The three VOR triad of tests
|
1) heat thrust
2) Headshake 4) DVA (Dynamic visual acutiy) |
|
|
Frenzel lenses
1) put on and nystagmus gets worse: 2) put on and nystagmus gets better: |
1) inner ear problems
2) Brain Problem |
|
|
Head Thrust Test
1) how to do it 2) what reflex it tests 3) Findings |
1)passively jerk head ~20 degrees and look to see if the eyes are maintain gaze stabiliztion or if they move with the head and then have to correct with a saccade
2) Vestibulo-ocular refelx 3) corrective saccada is a positive finding. The eye with the ocorrctive saccade is the one with the deficit |
|
|
Headshake Test:
1) how to perform 2) positive finding |
1) Using Frenzel lenses, passively shake the head about 2o times, 30 degrees in wither direction
2) Positive finding is ANY nystagmus. Beats toward the Healthy side. |
|
|
Dynamic visual acuity test
1) how to perform 2) positive finding |
1) passively shake the pt.'s head at 2Hz while he reads a snellen chart
2) positive finding is a 3 or more decrease in lines correctly read. |
|
|
The most important sene for maintaining upright posture?
|
propioception
|
|
|
Hallpike Test
1) how to do 2)Findings (reported ans observed) 3) diagnostic for? |
1) tilt head 45 degrees to side of injury so as to get posterior SCC in midsaggital plane.
2) this should cause vertigo and both eyes to beat up and twist outward 3) diagnostic for benign positional vertigo |
|
|
Common complaint for BPV
|
“I get dizzy just for seconds, but only when I tilt my head in a certain way”
|
|
|
In a positive hallpike test do the eyes twist towards or away from the offending side?
|
Toward
|
|
|
Etiology of BPV?
|
Crystal comes off and finds way into posterior canal and when moves around, stimulates cupula so when lie down on that side, get short intense spin
|
|
|
a good question to ask a pt. who may have BPV.
|
Do you get dizzy rolling over in bed?
|
|
|
limb testing to determine if proprioception is in tact:
6examples |
finger-nose-finger
Heel-shin rapid alternating motion joint propriocpetion vibration detection flexibility/strength |
|
|
Romberg test is for what?
|
proprioception in the dorsal column
|
|
|
1) Electrooculogoraphy does what?
2) replaced by what? |
1) tracks eye movement
2) video |
|
|
If a pt has a UNILATERAL hearing deficit, what do you do?
|
SNED THEM FOR IMAGING, they may have an tumor!
|
|
|
1) What is another tool one ca use for low suspicion assymetric hearing loss?
2) what does it evaluates? |
1)Auditory brainstem response
2) fucntions of cranial nerves (1,3,5,7) |
|
|
Computerized dynamic posturography test what?
|
How well do you use your reflexes to maintain balance.
|
|
|
1)What kind of imaging is the gold standard for looking for imaging the 8th neve? (High suspicion assymetric hearing loss)
2) Contrast? |
MRI
2) Gadolinium |
|
|
When would we image a vertigo patient?
|
When they have an additional complaint (headahe, hearing loss)
|
|
|
What would you think of if a person has vertigo initated by sound?
|
Hole in the Superior SC
|
|
|
5 most common diagoses for vertigo
|
1) BPV
2) vestibular neuritis 3) meniere's syndrome 4) migrane-related vertigo 5) Small vessel CVD |
|
|
Most patients with vertigo do or do not need surgery?
|
Do not
|
|
|
Medical options for therapy of vertigo
|
dietary chages
diuretics steroids aminoglycosides allergy |
|
|
4 Indications for vertigo surgery?
|
Fluctuating endorgan disease
Inadequate medical control Adequate capacity for compensation Thorough informed consent |
|
|
3 types of surgery for vertigo?
|
Total ablative-labyrinthectomy
Selective ablative-nerve section Selective non-ablative- ELS surgery, SSC plugging |
|
|
3 Goals of vertigo rehab?
|
quantify functional deficits
promote optimal balance strategies Define alteration of lifestyle |
|
|
Mechanisms of vertigo rehab
(just be familiar) |
Recovery of VOR function
Central compensation/plasticity Substitution Reinforcement of remaining pathways Resolution of visual-somatosensory conflict Global conditioning Psychological reinforcement Alteration of lifestyle |
|
|
things that make someone a Candidate for Formal Vestibular
Rehabilitation Therapy |
1) moderate-severe bilateral loss
2) failed med and surg 3) head trauma 4) abnormal sensory conflict |
|
|
How do you tell btween someone with a stroke and someone with vertigo?
|
vertigo can stand, stroke cannot
|
|
|
if you have a utricle or saccule lesion which side do you fall to?
|
the side of the injury
|
|
|
VOR circuit
|
|