![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
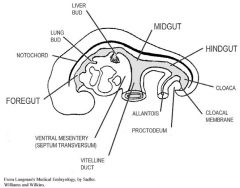
Through what kind of foldings is the primitive gut tube formed? |
Longitudinal - Head & Tail foldings Transverse folding |
|
|
When is the primitive gut tube formed (the week of development)? |
4th week of development |
|
|
What are the subdivisions of the primitive gut? |
- foregut, midgut, hindgut |
|
|
What are two kinds of mesenteries and what parts to they connect? |
- Ventral and Dorsal mesentery - Ventral: connects only the FOREGUT to the anterior abdominal wall - Dorsal: connects the foregut, midgut and hindgut to the posterior abdominal wall |
|
|
What is cloaca? |
Cloaca is the part at the end of the primitive hindgut. |
|
|
What separates the cloaca (sewer) and proctodeum? |
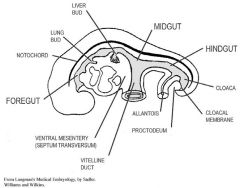
cloacal membrane |
|
|
What does cloacal membrane separates? |
cloaca and proctodeum |
|
|
What is vitelline duct? |
- this develops into the yolk stalk, which connects primitive mesoderm (endoderm) to the yolk sac |
|
|
What is another name for ventral mesentery? |
Septum transversum |
|
|
What lines and supports the primitive gut tube? |
- endoderm - splanchnic mesentery |
|
|
What does splanchnic mesentery provide to the primitive gut tube? |
- blood vessesls, connective tissue and smooth muscles associated with the gut |
|
|
What does endoderm forms in the gut tube? |
- lining of the digestive tract (epithelium ) - lining of the outgrowth of the digestive tract (respiratory system) - parenchyma cells (secretory cells) that outgrows from the digestive system - lung, pancreas, and gall bladder |
|
|
When does vellitine duct disappears? |
5th - 6th week of development
|
|
|
What is the remnant of the vellitine duct, when it does not disappear? |
Meckel's diverticulum |
|
|
Tell me about the Meckel's diverticulum (numeric) |
2% in population twice as common in males 2 feet from the ileocecal junction 2 inches long |
|
|
What are four uncommon conditions due to vetelline duct being remained? |
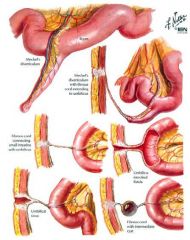
1. opened tube -> umbilical fistula 2. distal part is opened -> deep belly button; this traps the bacteria causing infection 3. medial part is opened -> forms a cyst 4. all collapsed but still connected to ileum -> limits the movement of the ileum |
|
|
What is SO special about the endoderm and what is the problem of that being special? |
- endoderm can form into anything - When endoderm remains in the digestive tract, such as Meckel's diverticulum, this develops into anything (pancreatic or gastric tissues) that secrete HCl and pancreatic tissue. However, the ileum is not grown to stand HCl and pancreati |
|
|
What other diverticulae and cysts are formed other than Meckel's diverticulum? How are they formed? |
- when the notochord (mesoderm) fails to separate from the endoderm, the vertebral column and gut tube are connected to each other. - This forms a diverticulae. If only the distal and proximal part of the diverticulae are collapsed, it forms a cyst. - This cyst becomes a tumor |
|
|
What are the derivatives of the foregut? |
- Respiratory tree from larynx and alveoli - esophagus - stomach - duodenum before the cystic duct - liver, pancreas, gall bladder |
|
|
What are the 8 steps of the foregut development? |
1. outgrowth of the larynotracheal ligament to from the respiratory system 2. foregut dilation 3. elongation of foregut to push the forgut into the abdominal cavity from the heart 4. proliferation of the endoderm at the proximal and distal part of the dilated foregut 5. recanalization occurs by the cavitation of the proximal and distal part of the foregut 6. Shaping of the stomach - the dorsal border of the stomach moves to LEFT. - dorsal mesentery forms the greater omentum (horizontal), splenorenal ligament, gastrosplenic ligament (vertical) - ventral mesentery forms the lesser omentum, Glisson's capsule, peritoneal lining of the liver and liver's ligament (coronal, triangular and falciform ligament) 7. the dorsal part of the stomach elongates more rapidly to from greater curvature 8. outgrowth of liver, pancreas and gall bladder |
|
|
What happens if the cavitation does not occur properly? |
- the foregut is partially (stenosis) or fully closed (atresia) |
|
|
The derivatives of the midgut? |
1. duodenum distal to the common bile duct 2. jejunum & ileum 3. cecum & appendix 4. ascending colon 5. proximal part of the transverse colon |
|
|
The steps of the midgut formation? |
1. umbilical herniation - the midgut elongates and moves into the umbilical cord (6th week) 2. Elongation of the proximal part of the midgut forms the coils of the small intestine & 90 degree counter-clockwise rotation 3. The proximal part of the midgut returns to the abdominal cavity and pushes the hindgut to the LEFT & 180 degrees counter-clockwise rotation puts the duodenal-jejunal junction in the adult position. (10th week) 4. Elongation of the distal part of the midgut pushes the cecum from sub-hepatic position to the right iliac fossa. |
|
|
When is the umbilical herniation occur? |
6th week |
|
|
When do the proximal part of the midgut returns to the abdominal cavity? |
10th week of the development |
|
|
in total of what angle, does the midgut turn? |
270 degrees counter-clockwise rotation |
|
|
How is the cecum moved from the sub-hepatic position to the right iliac fossa? |
Through further elongation of distal part of the midgut |
|
|
Due to further elongation of the distal part of the midgut, where does cecum end up in? |
right iliac fossa
|
|
|
What happens if the midgut fails to rotate at 180 as it returns to the abdominal cavity? |
The SI stays in the right side and LI stays in the left side but this does not cause a problem |
|
|
What is omphalocele? |
This is a condition when the midgut fails to return. The midgut is covered with the amniotic membrane. Treatment: the surgeon moves the midgut back to the abdominal cavity. However, the surgery has to be done several times to wait until the abdominal cavity grows enough to receive the midgut. - If the surgery was done at once, the baby's diaphragm starts to fall and makes the baby hard to breathe. |
|
|
What is the gastroschisis? Treatment? |
When the midgut comes out of the umbilical cord and exposed to the amniotic fluid. This causes the midgut to be fibrous, which limits the mobility of the midgut Treatment: the surgeon cuts part of the midgut and anastomoses with a good fit -> this cause the baby to have a short gut |