![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
249 Cards in this Set
- Front
- Back
|
Describe phases of spermatogenesis |
Phase 1: Spermatogonia ---meiosis I and II---> Spermatids Phase 2: Spermatids---spermiogenesis--->spermatozoa |
|
|
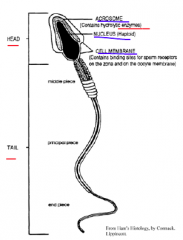
Describe morphology of spermatozoa |
|
|
|
What glands contributes to the seminal fluid? |

25. Seminal vesicle - 60% 14. Prostate gland - 30% 26. Bulbourethral Gland - 10% |
|
|
Lack of sperm in semen is called? Deficiency in sperm is called? The seminal fluid functions to? |
Azoospermia (zero), oligospermia (some) 1. provide a nutrient source for the spermatozoa 2. to neutralize vaginal acidity 3. promote sperm motility |
|
|
1. What is the normal site of fertilization? 2. The spermatozoa that do not get pumped up the fertilization site colonize what part of the uterus? |
1. Ampulla of the uterine tube 2. The cervical crypts |
|
|
Describe the two non disjunction events that could lead to aneuploidy |
non disjunction in meiosis I - Gametes are N = 24, 24, 22, 22. - Fertilization = 24 or 22 + normal 23 = 47 (trisomy) or 45 (monosomy). No gametes are normal. non disjunction in meiosis II - Gametes are N = 24, 22, 23, 23. - So one 1/4 will have 24 (will make trisomy) and 1/4 will have 22 (monosomy). 1/2 of gametes are normal. |
|
|
What can Aneuploidy arise from? |
Aneuploidy (abnormal chromosome numbers) can come from non disjunction - the failure of chromosomes to separate during meiosis I or II. |
|
|
What is capacitation? |
• A process that creates fully functional spermatozoa • After 4 – 6 hours in the female reproductivetract • Increased motility and metabolism • Necessary for: 1. Sperm – egg attachment 2. Acrosome reaction |
|
|
Follicles |
The cellular units that contain the developing egg (oocyte) |
|
|
Blastomeres |
- totipotential cells produced from mitotic divisions (cleavage) |
|
|
What is a Morula? What happens at this stage? |
8 cell (8 blastomeres) stage. Compaction: - increase contact of cells to make a circle. - Differentation starts - formation of trophoblast (implantation + placenta) and inner cell mass (embryo, amniotic mem. and yolk sac) - between 3rd and 4th cleavage |
|
|
# of chromosomes in somatic cell? # of chromosomes in gamete cell? |
46, 23 |
|
|
Trace the passage of sperm out of the penis |
Testis - rete testis- efferent tubules - epididymis - vas deferens - urethra
|
|
|
Describe the phases of oogenesis
|
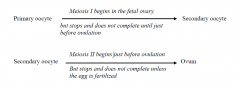
P. Oocyte -> S. Oocyte - Meiosis I in fetal ovary - Meisis I stops until just before ovulation S. Oocyte -> Ovum - Meiosis II just before ovulation - Meiosis II stops until fertilization |
|
|
1. graafian follicle
2. Stigma |
1. Large 2° follicles - It will go through Meiosis I before ovulation 2. ovarian surface from which graafian follicle will burst out of. |
|
|
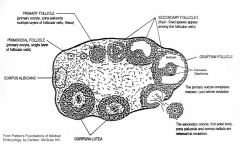
Describe the Primordial follicle |

- 1° oocyte
- single layer of follicular cells (AKA granulosa cells) - arrested in prophase of Meiosis I |
|
|
Describe the primary follicle |
- contains 1° oocyte - Zona Pellucida - multiple layers of follicular cells - outer layer: theca (make androgens, which is made into estrogen by follicular cells) |
|
|
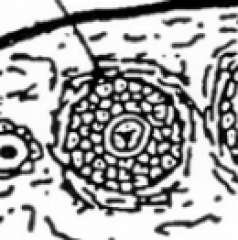
Describe the secondary follicle |
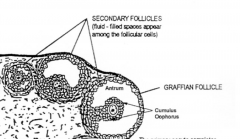
- like 1° follicle but has fluid filled space (antrum) - contains 1° oocyte - cumulus oophorus (The oocyte and the follicular cells immediately surrounding) |
|
|
What do the granulosa cells secrete to the inside of the oocyte over the ZP?
What structures allow for secreted proteins and metabolic support to transfer over the ZP? |
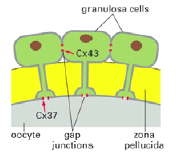
OMI: Oocyte Maturation Inhibitor - keep the 1° oocyte suspended in the meiosis I Gap junctions between the granulosa cells and occyte allow for this transfer |
|
|
1. mural follicular cells 2. cumulus oophorus |

1. follicular cells forming the wall of the antrum in a 2° follicle. - remain behind in ovary after ovulation - form granulosa lutein cells of corpus luteum 2. complex made of the occyte and follicular cells immediatly surrounding it. - project into antrum |
|
|
What is the Corpus Luteum and what is it a remnant of? |
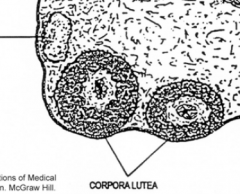
- Remnant of mural follicular cells left behind after ovulation and theca cells - will become corpus albicans after 2 weeks (if no fertilization, no hCG) - if they are maintained then the ovary will stay in a reproductive state |
|
|
Name of follicular cell layer surrounding ZP after ovulation? |
Corona Radiata - will fall away after a few days |
|
|
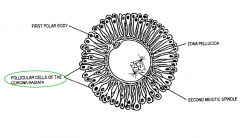
Describe the morphology of the egg as it leaves the ovary |
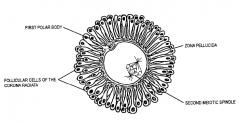
- 2° oocyte - Z.P. - Corona Radiata - 1st polar body (from Meiosis I) |
|
|
What will the binding of the sperm to the egg induce? |
- 2° oocyte start meiosis II - cortical granules exocytose and change the ZP3 protein so other sperm cannot bind to egg (zona reaction) |
|
|
acrosome reaction |
- acrosomal enzymes (hyaluronidase and acrosin) released from acrosome to get through ZP3 in the Z.P. - species specific |
|
|
male and female pronuclei |
- female pronucleus formed after meiosis II (discard the second polar body) - sperm will break down to the male pronucleus within 12 hours of entering the 2° oocyte. - the two nuclei join to restore diploid number of 46 |
|
|
Day 4 after fertilization? |
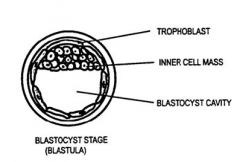
Blastocyst stage: ~ 32 cell stage - fluid enters morula making balstula - blastocyst cavity - still surrounded by ZP |
|
|
Cleavage |
A series of comparatively rapid mitotic divisions resulting in progressively larger numbers of progressively smaller cells. - 1st cleavage is 24 hours after meiosis II (production of 2nd polar body) - subsequent divisions are 12h-24h after - between 3rd and 4th cleavage division: compaction |
|
|
What happens at day 5 and 6 after fertilization? |
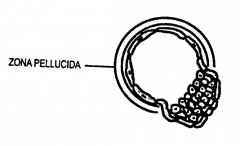
- Hatching (5 days) - trophoblasts make enzymes - The embryo breaks out of the zona pellucida - epithelial cells (of the endometrium) and trophoblast can now contact each other -Implantation (6 days) Contact occurs between the epithelial cells and the trophoblast. |
|
|
1. Syncytiotrophoblast 2. Cytotrophoblast |
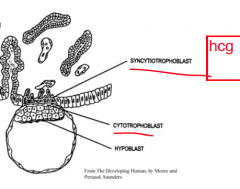
1. made by fusion of trophoblast cells, invades endometrium - multinucleated - source of human chorionic gonadotropin (hCG). 2. after syncytiotrophoblast formed, the trophoblast still on the embryo are called cytotrophoblast |
|
|
What consequences can a previous tubal inflammation (salpingitis) or scarring have for pregnant woman? |
- delayed passage of embryo through the fallopian tube - ectopic pregnancy (1:100) after ZP sheds off |
|
|
What happens to the inner cell mass as the embryo implants? |
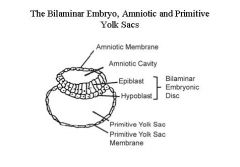
- the inner cell mass is converted into a two layered structure called the bilaminar embryonic disc: epiblast + hypoblast - the inner cell mass also create amniotic membrane surrounding the amniotic cavity |
|
|
Gestational age vs fertilization age |
Fertilization age: From point of fertilization Gestational age: From first day of menstrual cycle. - 2 weeks older than fertilization age. |
|
|
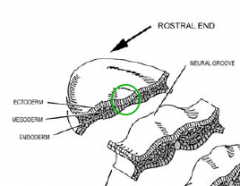
Describe gastrulation. |
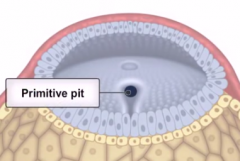
Bilaminar embryo becomes a trilaminar one. - epiblast cells migrate to one end to make the primitive streak (at the caudal midline i.e. in the middle of the caudal end) - The cranial end of the primitive streak is called the primitive knot (AKA primitive pit or Hensen's node). - The epiblast cells ingress at the primitive pit and along the primitive streak (primitive groove) and then begin to migrate laterally and rostrally to caudal end. |
|
|
Describe the three layers formed from gastrulation.
|
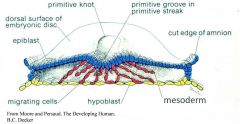
- 3 layers, all coming from epiblast cells - endoderm (replace hypoblast) - mesoderm - ectoderm (amniotic cavity facing epiblast cells). |
|
|
Why is there a rostro - caudal gradient in developmental activity?
|
- first cells to migrate rostrally and make rostral structures. They are more advanced than the caudal end. - primitive streak is still developing the 3 layers in the cuadal end while the rostral tissues proceed with growth, differentiation and organ formation. - primitive streak gets smaller and smaller (finally dissapears at sacrococcygeal part) |
|
|
Where does the notochord come from? |
- mesoderm: Epiblast cells which ingress through rostral end of the primitive streak AKA Hensen's node, primitive knot, primitive pit. |
|
|
What does the ectoderm contribute to the formation of? |
- Nervous system - Tissues that cover the body surface (epidermis, hair, nails) - Body surface glands |
|
|
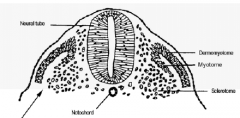
Describe Neurulation. |
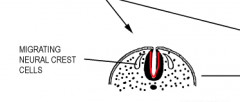
- Notochord + paraxial mesoderm sends signals to part of ectoderm -> differentiate to Neuroectoderm - Neural folds and Neural groove - Folds fuse to make the neural tube - surface ectoderm covers the tube - Mesoderm cells move up between tube and |
|
|
rostral neuropore and the caudal neuropore |

Last parts to close in the neurulation process. |
|
|
What does the Neural tube develop into? What about the surface ectoderm flanking the neural plate? What about the mesoderm that migrated up between the ectoderm and neural tube? |

The neural tube develops into the brain and the spinal cord. The non-neural ectoderm will contribute to the skin covering the brain and spinal cord. The mesoderm will form the bones of the calvarium, covering the brain and the vertebrae covering the spinal cord. |
|
|
Describe what has happened with Anencephaly or myeloschisis |
Failure to close the neuropores. Rostral (anencephaly) and caudal (myeloschisis) neuropores 'Schisis' = breaking up of attachments or adhesions |
|
|
1. As the neural crest cells migrate out of the neural fold and into the body, what do they form? 2. What do the neural crest cells that migrate out from the cranial end of the neural tube also able to form? |
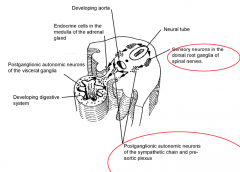
1. - DRG sensory neurons - Postganglionic sympathetic chain - Postganglionic in prevertebral ganglia - postganglionic in walls of viscera 2. cranial connective and skeletal tissues |
|
|
What does the endoderm develop into? |
- lining tissue (epithelium) of gastrointestinal tract - secretory cells of Liver, G.B. and Pancreas - lining of the ducts of the organs - lining of respiratory system |
|
|
Vitelline duct |
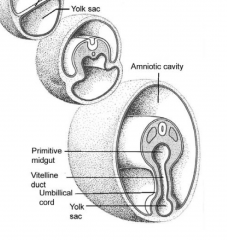
- connects the primitive gut to yolk sac - formed by the folding of the lateral plate endoderm into the primitive gut - this is due to somites enlargement |
|
|
What does the mesoderm divide into? |
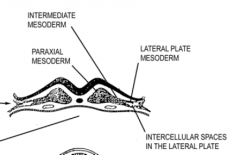
- paraxial mesoderm - lateral plate mesoderm - intermediate mesoderm |
|
|
What are the somites? Where are they derived from? What will they develop? |
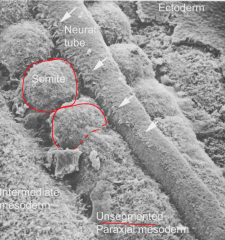
- derived from paraxial mesoderm - form blocks of cells in craniocaudal sequence - will develop vertebrae, intervetebral discs, ribs, skeletal muscles of body wall and limbs, connective tissue of the body wall |
|
|
What does the intermediate mesoderm form? |
Kidneys, ureter and gonads |
|
|
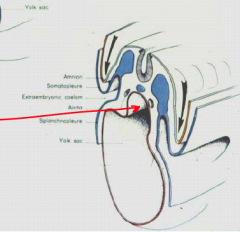
What is the intraembryonic coelom? What is it surrounded by? What does it form into? |

Cavity formed from the Lateral plate mesoderm. - somatic mesoderm (supports ectoderm) - splanchnic mesoderm (supports endoderm) - forms into the main body cavities: e.g the pleural, pericardial and peritoneal cavities. |
|
|
What does the intraembryonic (parietal) somatic mesoderm form into? What about the intraembryonic (visceral) splanchnic mesoderm? |

The somatic mesoderm contributes to the connective tissues, blood vessels and smooth muscle of the body wall and limbs. The splanchnic mesoderm contributes to the smooth muscle, blood vessels and connective tissue of the gastrointestinal tract and associated organs. |
|
|
What is the embryonic period? What is the fetal period? |
• Embryonic period… 0 to 8 weeks
- First two weeks … transport and implantation - 3 to 8 weeks … morphogenesis/organogenesis • Fetal period … 9 weeks to term |
|
|
Organogenesis |
- ectoderm, endoderm, and mesoderm develop into the internal organs of the organism. - Starts with the formation of the neural tube and primitive gut |
|
|
Placenta Accreta |
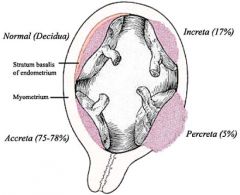
The placenta forms too deeply into the uterus wall |
|
|
Placenta Praevia |
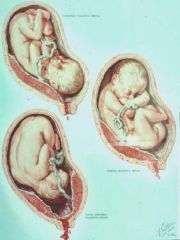
Placenta forms on the lower uterine segment |
|
|
What are the lacunae? |
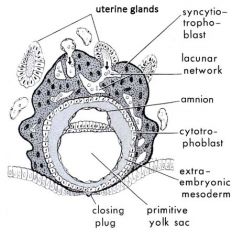
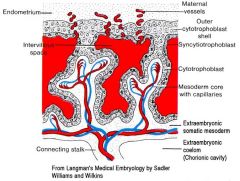
Spaces developed within the syncytiotrophoblast which are filled with mothers blood and secretions to provide nutrients for embryo (as the syncytiotrophoblast erodes) |
|
|
1. What is the Extra-embryonic mesoderm? 2. What can it be divided into? |
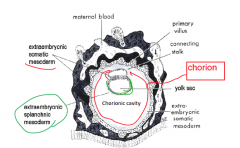
1. separates the embryo from the cytotrophoblast --> coelom formed within it 2. extraembryonic mesoderm lining the cytotrophoblast and covering the amniotic membrane is called the extraembyonic somatic mesoderm, and that covering the yolk sac is the extraembryonic splanchnic mesoderm. |
|
|
How is the extaembryonic coelom (AKA Chorionic cavity) formed? |
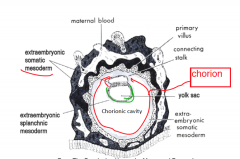
start off as small coelom in the extraembryonic mesoderm and group together - by the end the coelom has separated the embryo from the cytotrophoblast except from at the connecting stalk |
|
|
What is the Chorion? |
1. layer of extraembryonic somatic mesoderm 2. cytotrophoblast 3. syncytiotrophoblast |
|
|
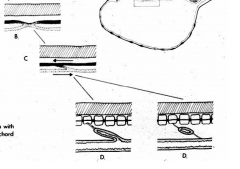
Describe the development of the villi:
Primary--> Secondary--> Tertiary Villi |
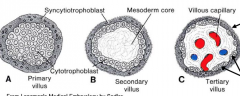
Primary Villi = finger like projections of cytotrophoblasts into syncytiotrophoblast into the decidua. Secondary Villi = Extraembryonic somatic mesoderm invades the cores of the primary villi Tertiary Villi = blood vessels develop from the mesoderm in the 2° villi. Spaces without cytotrophoblasts, mesoderm directly in contact with syncitiotrophoblast. Nutrients/waste only needs to cross 2 layers. |
|
|
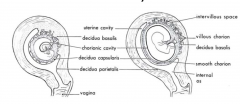
Describe the 3 regions of the decidua.
|
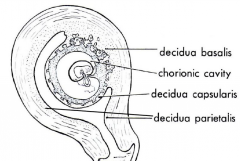
Inner endometrium of uterus = decidua Decidua basalis - under location of birth Decidua capsularis - capsulates embryo Decidua parietalis - everything else |
|
|
Cytotrophoblastic shell |
- cytotrophoblasts at the tip of 1° villi will push through syncitiotrophoblast to create shell to anchor chorion to decidua - these villi = anchoring villi |
|
|
Where are the umbilical arteries and veins derived from? |
Extraembryonic somatic mesoderm that create vessels which form in the connecting stalk |
|
|
Intervillious spaces |
Lacunae develop into intervilious spaces
Blood enters from spiral artery Leave from endometrial veins |
|
|
Smooth Chorion?
|
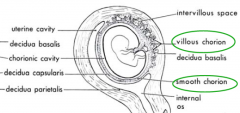
Villi recede in the decidua capularis, forming the smooth chorion and branch out in the decidua basalis, forming the villous chorion |
|
|
What is the fate of the chorionic cavity? |
- The amniotic cavity expands, surrounding the embryo. The amniotic membrane envelops the connecting stalk --> outer membrane of the umbilical cord. - The amniotic membrane becomes applied to the chorion (amniochorionic membrane). |
|
|
What is the fate of the uterine cavity? |
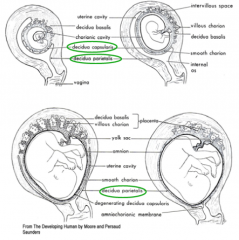
- implantation site expands into the uterine cavity until the decidua capsularis comes into contact with and fuses with the decidua parietalis. |
|
|
What are the features of a full term placenta?
|
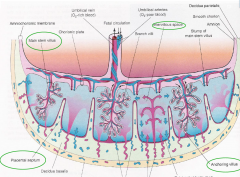
- placental septae (decidua basalis tissue between enlarged intervillous spaces) - cotyledons - collections of villous trees (cobble stones on outer placenta covering) |
|
|
What is inside the umbilical cord? |
- 2 umbilical arteries delivering oxygen depleted blood from the fetus to the placenta (becomes superior vesical arteries and the medial umbilical ligaments). - 1 umbilical vein delivering oxygen rich blood to the fetus (becomes ligamentum teres) - The vitelline duct (yolk stalk) and the allantois in the proximal portion. - Wharton's jelly; a gelatinous connective tissue that supports the vessels. |
|
|
monozygotic vs dizygotic twins? |

- anastamoses may occur in monochorionic, monozygotic twins causing twin-twin transfussion syndrome |
|
|
Name 3 placental pathologies |
- Placenta accreta = Abnormally deep attachment of the placenta – ie to the myometrium or deeper. - Placenta praevia= Placenta is abnormally placed, very close to partially or fully covering the internal os. - Placenta abruption = Partial or complete separation of the placenta from the uterus before labour. |
|
|
What does the splanchnic mesoderm form?
What does the endoderm form in the gut? |
Mesoderm: - smooth muscle, connective tissues and blood vessels that are associated with the derivatives of the primitive gut. Endoderm: - forms the tissue lining the digestive tract and lining its outgrowths - secretory cells (parenchyma) - lining of the ducts |
|
|
Meckel's diverticulum Where else can there be Diverticulae? |
- vitelline duct connects antemesenterically at the primitive midgut at the distal ileum. If it persists then it will form a diverticulum. - Diverticulae and cysts can also occur if the notochord and the endoderm fail to separate |
|
|
When week of development does the embryo start to fold? What is the cloacal membrane? |
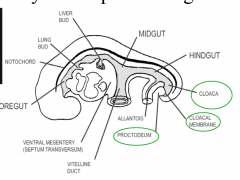
4th week: longitudinal and transverse folding Membrane separates the cloaca from the proctodeum, a pit-like depression on the external surface of the embryo. |
|
|
What does the foregut give rise to? |
- respiratory tree from the larynx to the alveoli. -esophagus - stomach - duodenum as far as the entrance of the common bile duct - liver, gall bladder, and pancreas |
|
|
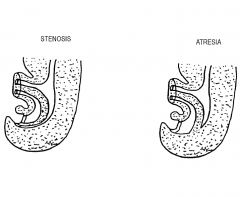
What reverses the process of occlusion in the foregut after gastric dilatation? |
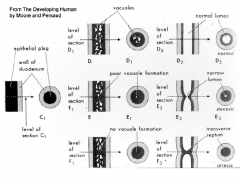
- recanalization by cavitation - failure to do so will give rise to stenosis or atresia |
|
|
What are the 8 steps of the foregut formation? |
1. formation of the laryngotracheal diverticulum 2. appearance of the gastric dilatation 3. elongation of the esophagus (stomach-->abdomen) 4. occlusion (promixal and distal to gastric dilation) 5. recanalization 6. stomach rotation 7. differential growth 8. outgrowth of the liver, gall bladder and pancreas |
|
|
The midgut develops into? |
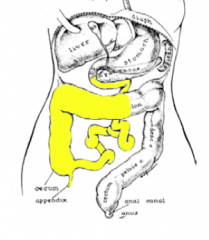
- duodenum distal to the opening of the common bile duct. - the jejunum and ileum - the cecum and appendix - the ascending colon and the proximal part of the transverse colon. roughly corresponding to the field supplied by the SMA. |
|
|
3 steps of the midgut formation? |
1. Elongation of the midgut and herniation of the midgut loop in the midline into the umbilical cord 2. Further elongation of the proximal half of the midgut loop creating the coils of the smallintestine. Rotation of the loop 90° counter – clockwise (towards the embryo's right). 3. Return of the midgut loop to the abdominal cavity. 180° further rotation counter-clockwise. Distal part of midgut elongates causing cecum to descend. |
|
|
Omphalocele |
- intestines lie within the umbilical cord because it failed to return back into the gut. It is covered with the translucent amniotic membrane that covers the cord externally. |
|
|
Gastroschisis |
- resulting from a rupture in the anterior body wall, usually on the right hand side of the umbilical cord. The intestines are not covered and float freely in the amniotic fluid 'Schisis' = breaking up of attachments or adhesions |
|
|
The hindgut gives rise to? |
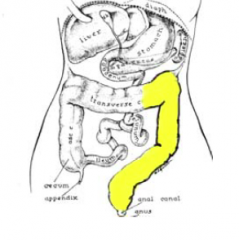
- the distal part of the transverse colon - the descending colon - the sigmoid colon - the rectum - the upper part of the anal canal |
|
|
Hindgut development: The urorectal septum partitions the cloaca into? |
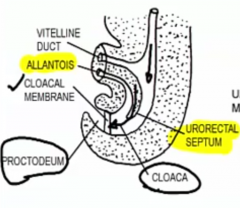
- urogenital sinus - rectoanal canal |
|
|
Imperforate Anus |
results from dorsal deviation in the path of the growth of the urorectal septum. If the urorectal septum fuses with the posterior wall of the cloaca, rather than the cloacal membrane, it will result in complete atresia. |
|
|
Fistulae during urogenital development |
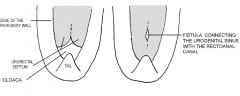
Incomplete fusion near the leading edge of the urorectal septum (bifid). Can cause the urogenital and rectoanal canals to maintain a connection. |
|
|
Meconium |
- made up of secretions, cells sloughed from the gut walls and cells and lanugo hairs that have been swallowed with the amniotic fluid. - makes up the contents of the fetal intestine |
|
|
What portion of the pancreas is from the dorsal pancreatic duct? |
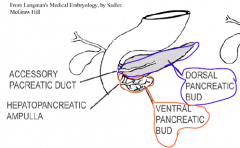
dorsal pancreatic bud = head, body, tail of pancreas, main + accessory pancreatic duct ventral pancreatic bud = Uncinate process, hepatopancreatic ampulla |
|
|
Causes of obstruction |
- Failure to recanalize (stenosis or atresia) - Fetal vascular accident (blood supply compromised to section of bowl) - Congenital hypertrophic pyloric stenosis - Annular pancreas - Congenital volvulus (twist of intestines) - Intussuception (small intestine go into large intestine) - Imperforate anus - Congenital membranous atresia (anal membrane fails to break down) - Meconium ileus |
|
|
Polyhydramnios |
- an excess of amniotic fluid in the amniotic sac due to obstruction of gut |
|
|
Meconium ileus |
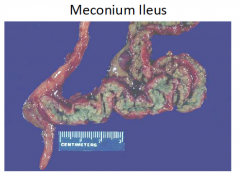
If the meconium is too viscous, the newborn may not be able to pass it and so it becomes a source of obstruction. |
|
|
When does the laryngotracheal diverticulum start to form and what does it form from? |
- 4th week - endoderm lining of foregut (ventral wall on rostral end) |
|
|
What does the endoderm of the laryngotracheal diverticulum develop into? What about the surrounding splanchnic mesoderm? |

Endoderm --> epithelium lining airways and pneumocytes lining the alveoli Splanchinc mesoderm --> pleura, connective tissue, muscles and vessels of the lungs - controls the branching of bronchi on the larygotracheal tube |
|
|
Tracheo-esophageal Fistula |
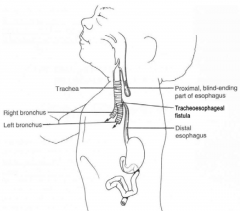
1:3000
|
|
|
What lines the primitive pleural cavities? The parietal pleura can be subdivided into? |
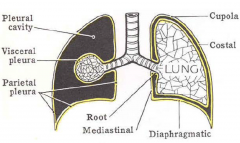
- The primitive pleural cavities are lined with a pleural membrane derived fromsplanchnic mesoderm.
- The costal pleura - The diaphragmatic pleura - The mediastinal pleura: middle area - The cervical pleura: AKA cupola. |
|
|
What do Type II pneumocytes secrete? |
Surfactants, to reduce the surface tension in the alveoli making lungs easy to inflate. |
|
|
What happens to a baby's breathing if there is not enough surfactant produced or if surfactants are over consumed? |
- increased work for respiration - hyaline membrane disease - respiratory distress - Infant respiratory distress syndrome |
|
|
What are 4 strategies to prevent respiratory distress? |
- baby stays in uterus longer - speed maturation by giving hormones to mother - predict those with pulmonary immaturity - administer surfactants to baby |
|
|
What are 4 things the growth of the lungs in utero depends on? |
- physical space in the thorax - fetal lung fluid (lung needs to produce its secretions) - amniotic fluid access (growth factors inside) - practice breathing (with amniotic fluid) |
|
|
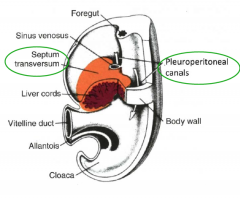
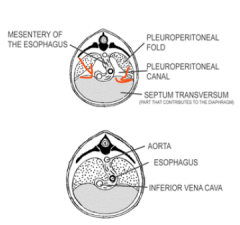
What forms the diaphragm in the fetus?
|
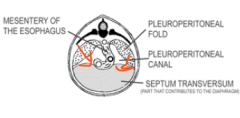
- cranial part of the septum transversum (ventral mesentery) - dorsal mesentery of foregut (abdominal esophageal portion) - pleuroperitoneal folds |
|
What seals the pleuroperitoneal canals in the 9th week of development? |
The pleuroperitoneal folds. The left fold is slower in growing over the canal. |
|
|
Congenital Diaphragmatic Hernia |
Left pleuroperitoneal fold doesn't close in time. In the 10th week, the abdominal organs move up into the thorax. Fetoscopic Tracheal Occlusion (FETO) can be used to counter this by plugging the trachea, lungs will grow and push viscera down. |
|
|
Describe the hierarchy of pleural branching starting with the trachea. |

- trachea
- 1° / principle bronchi (to each lung). - 2° / lobar bronchi (to each lobe) - 3° / segmental bronchi - terminal bronchiole - respiratory bronchiole - alveolus |
|
|
1. What does repeated branching of the larygotracheal tube form?
2. What controls this branching? |

1. Forms the bronchi 2. Mesoderm controls the branching and determines the identity of the airway |
|
|
What embryonic structure forms the bladder and urethra? What forms the kidneys and ureters? |
Cloeca ---> urogential sinus ---> bladder and urethra The intermediate mesoderm ---> nephrogenic cords ---> metanephric mass and ureteric bud ---> kidneys and the ureters. |
|
|
1. What cord does the intermediate mesoderm condensate to become? |
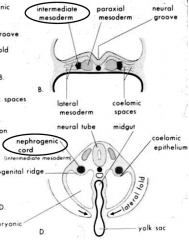
nephrogenic cords |
|
|
In the pronephric phase, the pronephric duct grows towards the sacral end of the embryo to open up to? |
The cloaca |
|
|
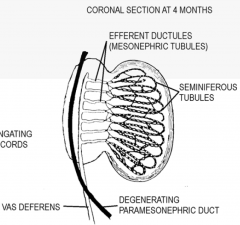
During the fourth week, the ________ part of the nephrogenic cord and the associated (cervical) part of the __________ duct degenerate and forms _________. The remainder of the duct persists and referred to as ____________ duct. |
Pronephric, Pronephric, Vesicles, Mesonephric |
|
|
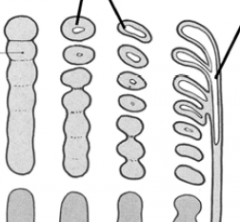
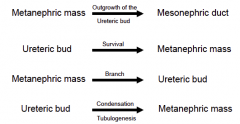
What does the metanephric mass signal (with GDNF) to mesonephric duct to do? |
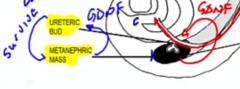
Make an outgrowth: The Ureteric Bud, which sends signals out to to the mass to make it survive. |
|
|
1. What are the derivatives of the ureteric bud? 2. What are the derivatives of the metanephric mass? |

1. The urine collecting system - i.e. Calyces, Renal pelvis, Ureter, collecting tubules, collecting ducts, etc. 2. The urine producing system - i.e. the nephrons of the kidney (renal corpuscles, proximal and distal convoluted tubules and the loops of Henle). |
|
|
The ends of the ureteric bud branches induce the metanephric mesoderm to organize into? |
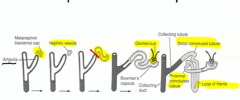
Metanephric vesicles, which end up attaching to the ducts. (bud = dark grey, mass = light grey) |
|
|
As the kidneys ascend and rotate medially, what happens to the renal arteries? |
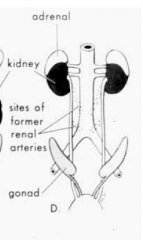
The renal arteries also ascend up the aorta. |
|
|
What is happening to the development of the kidney in Multicystic Kidney, Recessive Polycystic Kidney Disease, and RPKD? |
The nephric vesicles are not properly developing to the tubules. |
|
|
After the ureteric bud signals the metanephric mass to survive, what does the metanephric mass signal to the ureteric bud? |
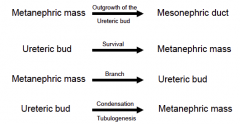
To start branching |
|
|
After the ureteric bud starts branching, what does the ureteric bud signal to the metanephric mass? |
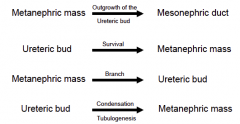
To start Tubulogenesis/condensation: start creating tubles |
|
|
What are some Abnormalities of the kidney ascent? |
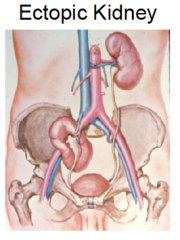
- accessory renal arteries - ectopic kidneys (if it doesn't asend, it will not rotate medially) - Fused kidneys (can't ascend past the SMA, therefore also ectopic) |
|
|
What are some abnormalities between the interaction of the metanephric mass and ureteric bud? |
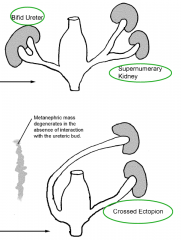
- bifid ureter (bud splits before entering mass) - supernumerary kidney (bud splits before entering mass with large distance in between buds or two buds develop from the mesonephric duct) - crossed ectopian - Renal Agenesis (failure of the bud and mass to interact) |
|
|
What are the two types of renal agenesis? |
Unilateral: failure of one kidney to form. Bilateral: leads to the oligohydramnios syndrome: Potter's facies, flexion contractions, pulmonary hypoplasia |
|
|
Pulmonary Hypoplasia |
Lungs do not fully develop. Can be caused by a deficiency of amniotic fluid. |
|
|
Oligohydraminos |
Deficiency of amniotic fluid, which is needed for fetus to move limbs, practice breathing and get growth factors going into lungs and intestines. |
|
|
The fetus regulates the volume of amniotic fluid. 1. How does it increase the amniotic fluid volume? 2. How does it decrease the amniotic fluid volume? |
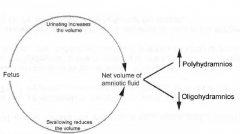
1. urinating 2. swallowing |
|
|
When the fetus swallows the extra amniotic fluid where does it go? |

It is absorbed through the fetal intestine into the fetal circulation. The volume is then passed across the placenta into the maternal circulation. Excess volume can then be cleared through the maternal kidneys. |
|
|
What could be some causes of oligohydramnios? |
Inability to urinate into amniotic fluid: • Bilateral renal agenesis • Posterior urethral valve (a remnant of the urogenital membrane) • Bilateral polycystic kidney disease • Premature rupture of the membranes (mother is leaking corionic fluid) |
|
|
What could be some causes of polyhydramnios? |
Inability to swallow amniotic fluid: - foregut obstruction - Anencephaly (distrupted cranial development, fetus has no reflexes to swallow) |
|
|
Patent Urachus |
Allantois does not close properly and so there is still a passage from bladder--->umbilicus |
|
|
Bladder Extrophy |
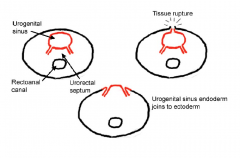
Urogenital sinus endoderm joins the ectoderm after a wound on ectoderm. Bladder will be facing the outside of the baby's body. |
|
|
What does the allantois regress to form? |
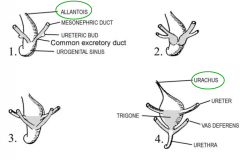
The urachus and subsequently the median umbilical ligament. |
|
|
Common excretory duct
|
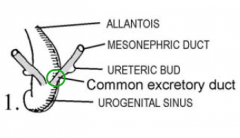
The segment of the mesonephric duct that lies between the urogenital sinus and the point at which the ureteric bud opens into the duct. |
|
|
What does the urogenital sinus develop into? |
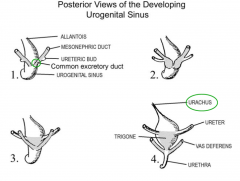
Bladder and urethra. Bladder = superior expansion of sinus Urethra = distal part of sinus remaining narrow |
|
|
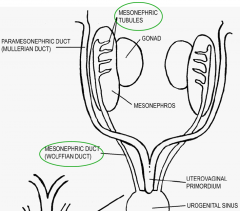
Indifferent stage |
Stage where you cannot tell the difference between M and F embryo. - first 7 weeks of development - can only tell M from Y chromosome, HY antigen |
|
|
At 3 weeks, the nephrogenic cord forms pronephric vesicles. What do these vesicles in the pronephros fuse to form? |
The pronephric duct |
|
|
What does the portion of the cloaca, which the pronephric duct grows into become? |
Urogenital sinus |
|
|
1. At 4 weeks, what part of the pronephric duct degenerates? 2. What is the name of the duct remaining after this degeneration? |
1. After the pronephric duct is formed, the pronephros part degenerates. 2. mesonephric duct |
|
|
What does the metanephric mass grow out from? |
mesonephric duct (AKA Wolffian ducts) |
|
|
The gonadal or genital ridge grows medially to which structure? |
mesonephros
|
|
|
What forms the sex cords in the gential ridge? |
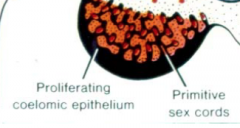
coelomic epithelium penetrating the intermediate mesoderm
|
|
|
If there is no Y chromosome, what do the primodrial germ cells and sex cords develop into? |
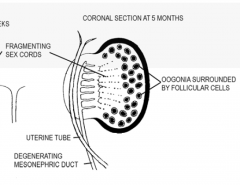
PMG ---> Oogenia (later becomes oocyte)
Sex cords ---fragment into---> Follicular cells |
|
|
If there is a Y chromosome (with SRY gene), what happens to: 1. Sex cords 2. Cells in the mesoderm of the genital ridge 3. PMG |
1. sex cords ----> seminferous tubules. The cells form the Sertoli Cells capable of secreting Antimuellerian hormone (AMH) 2. Differentiate into Leydig cells (secrete testosterone) 3. Spermatogonia |
|
|
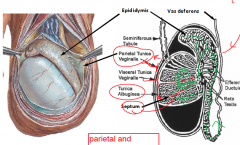
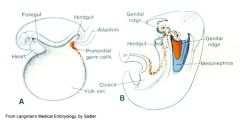
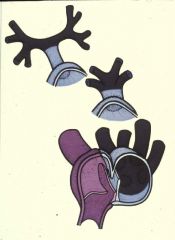
What happens in the trans-abdominal phase of the descend of the testis? |
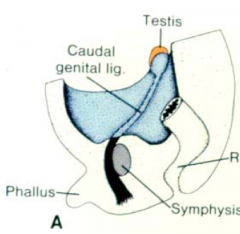
- passive process - gubernaculum (black in picture) pulls testis to mouth deep inguinal ring |
|
|
What happens in the trans-inguinal phase of the descend of the testis? |
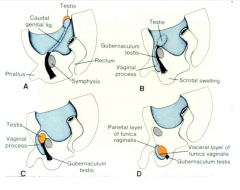
- active process - vaginal process follows gubernaculum to scrotum and acquires layers of abdominal wall to make the spermatic cord - testes and vas deferens follow the same path as the vaginal process, pushing it to the side. - distal end of process becomes the tunica vaginalis |
|
|
Name of condition where the testis do not descend. |
Cryptorchid Testes
|
|
|
What are some abnormalities of the processus vaginalis?
|
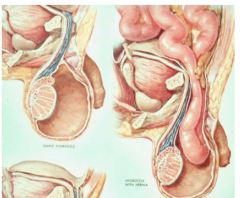
Hydrocele or congenital hernia |
|
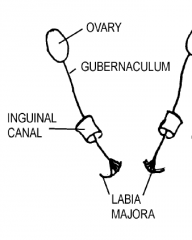
What does the gubernaculum form in the female? |
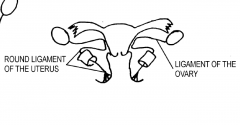
The part of the gubernaculum between the ovary and the uterus becomes the ligament of the ovary and the part between the uterus and the labium majus becomes the round ligament of the uterus. |
|
|
True or False: The Vaginal Process is present in both males and females. |
True. |
|
|
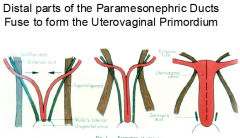
As the paramesonephric ducts enter the pelvis, they cross anterior to the mesonephric ducts and fuse together in the midline to form the? |
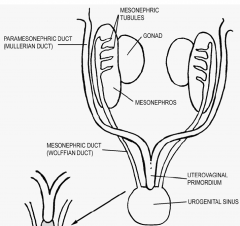
Uterovaginal Primordium. - lies posterior to the urogential sinus |
|
|
What is created from the endoderm of the urogential sinus when the uterovaginal primodium makes contact with it? |
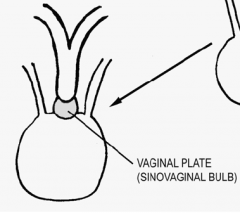
The sinovaginal bulb or vaginal plate |
|
|
What does the antimullerian hormone from the Sertoli cells of the seminiferous tubules induce? |
Cause the paramesonephric ducts and the uterovaginal primordium to degenerate. - prostatic utricle and appendix of testis are remnants of these |
|
|
The prostatic utricle and the appendix of the testis are thought to be remnants of? |
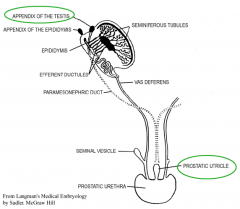
Uterovaginal primordium ---> Prostatic utricle Cranial end of the paramesonephric ducts ---> appendix of testis |
|
What do androgens from the Leydig cells of the developing testes induce with the mesonephric tubule and duct? |
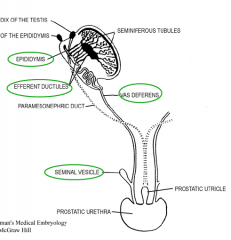
1. the mesonephric excretory tubules to link with the rete testis forming the efferent ductules. 2. the mesonephric duct to develop into the epididymis, vas deferens and ejaculatory duct. 3. the seminal vesicles to develop as outgrowths of the mesonephric ducts. |
|
|
What happens to the paramesonephric ducts and uterovaginal primordium in the absence of antimullerian hormone? |
Paramesonephric ducts ---> Uterine tubes Uterovaginal primordium ---fuse---> Uterus |
|
|
In the absence of testosterone, the mesonephric ducts degenerate. What are some remnants of the duct? |
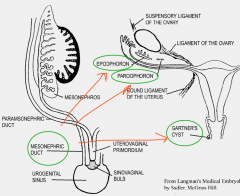
Found in the broad ligament:
- epoophoron - paroophoron In uterus: - gartner's cyst |
|
|
What can happen if the paramesonephric tubule does not fully fuse to create the uterovaginal primodium? |
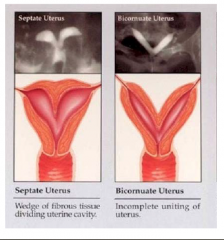
Divided uterus |
|
|
What does the vagina develop from? |
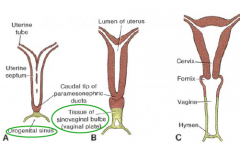
- uterovaginal primordium and the endoderm of the urogenital sinus via the vaginal plate. |
|
|
What is the hymen (covering over vagina) developed from? |
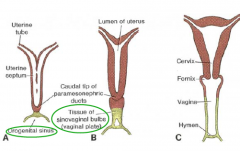
Endoderm of the urogenital sinus via the vaginal plate. |
|
|
What can happen if the hymen does not open at birth? |
Secretions from vagina and uterus can build up and get large (hydrometrocolpos). Can also lead to bladder being compressed and consequent hydronephrosis/kidney damage. |
|
|
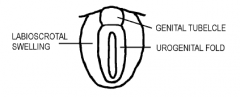
What are the 5 swellings present in the indifferent genitalia (up to 9 weeks of development)? |
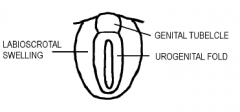
2 x swellings
2 x fold 1 x tubercle |
|
|
What do the 5 swellings of the indifferent genitalia form in the female? |
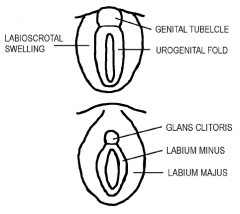
- the genital tubercle ---> glans clitoris - the urogenital folds ---> labia minora - the labioscrotal swellings ---> labia majora |
|
|
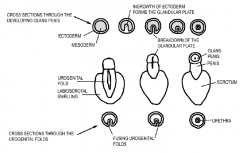
What does the ingrowth of epithelium on the ventral surface of the genital tubercle in males create? |
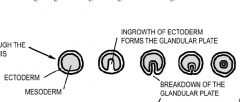
Glandular Plate |
|
|
True of False: The mesonephric duct will wait for androgen for an indefinite amount of time. |

False. The mesonephric duct will wait for chemical signals for a short amount of time. The external genitalia will wait for a longer amount of time. |
|
|
At 10 weeks, what causes the genitals to masculanize? |

Androgens from Leydig Cells in Testes, which are made into dihydrotestosterone in the target cell. Key point: reductase is vital for masculinization of the indifferent genitalia but not of the mesonephric duct and tubules. |
|
|
At 8 weeks, what causes the mesonephric duct and tubules to masculanize? |

Androgens from Leydig Cells in Testes |
|
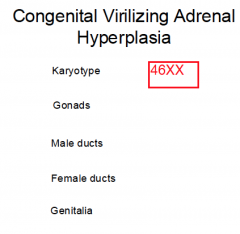
What would happen to a 46XX embryo producing too much testosterone? |

Gonads = Ovaries (XX genes) Male Ducts = No (androgen is being overproduced but the span of time the mesonephric ducts (MD) can respond to androgens is short.) Female Ducts = Yes (no testes, no AMH) Genitalia = masculanized (androgen is over produced and the ext. genitalia span of time it responds to the androgen is long) |
|
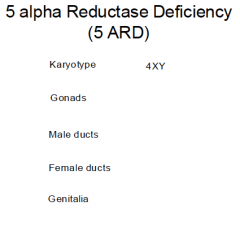
What would happen to a 46XY embryo unable to reduce testosterone? |
Gonads = Testes (listen SRY gene) Male Ducts = Yes (androgen is being picked up by target cell) Female Ducts = No (AMH is being produced by sertoli cells in testes) Genitalia = Feminized (androgen is picked up but not converted to dihydrotestosterone) |
|
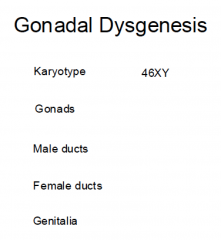
What would happen to a 46XY embryo where the indifferent genitals do not develop (streak ovary)? |
Gonads = streak ovary Male Ducts = No (no testes, no leydig cells, no androgen) Female Ducts = Yes (AMH is not produced) Genitalia = Feminized (no testes, no leydig cells, no androgens) |
|
|
1. How long does spermatozoa remain viable for in the female reproductive tract? 2. How long do oocytes live for? |
1. around 5 days 2. 24 hours |
|
|
What are the species specific and species non-specific phases of fertilization? |
Species specific = Acrosome reaction (ZP and sperm cell) Non-species specific = Ligand binding of sperm membrane to 2° oocyte membrane |
|
|
What is shed during parturition and menstruation? |
The endometrium's layers of epithelium and connective tissue that receive the embryo during implantation. - form contact with trophoblast in implantation |
|
|
True or False: While migrating from the ampulla to the uterus (via cilia and smooth muscle), there is no net growth in size of embryo |
True. The embryo is still retained in ZP until it hatches (day 5) so even though the cell numbers increase, the overall size does not get bigger. |
|
|
True or False: The hypoblast is responsible for the ectoderm formation. |
False. The hypoblast is replaced by endoderm in gastrulation. Consequently the hypoblastmakes no direct tissue contribution to the fetus. The epiblast will be responsible for the fetus. |
|
|
What happens to the corpus luteum if the embryo dies or no fertilization of the egg takes place? |
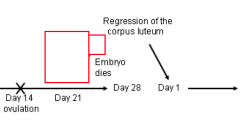
- if embryo dies, no hCG produced from syncytiotrophoblast. - If no hCG is present then the corpus luteum will regress, the uterus will slough and the next cycle starts |
|
|
What happens to the corpus luteum if the ovulated egg is fertilized? |
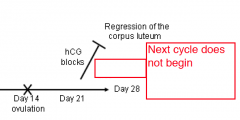
The syncytiotrophoblast of the embryo will produce hCG, which will block the regression of the corpus luteum |
|
|
What are the 2 layers before gastrulation and what are the 3 layers after gastrulation? |
Before: - epiblast (face amniotic sac) - hypoblast (face yolk sac) After: - ectoderm (face amniotic sac) - mesoderm - endoderm (face yolk sac) |
|
|
Describe medial, lateral sides and core of the neural folds |
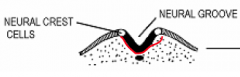
- Neuroectoderm medially - non-neural (surface) ectoderm laterally - Neural crest cells at the apices - mesoderm in core |
|
|
Primitive midgut |
During transverse folding, the endoderm in the middle of the embryo is rolled into aprimitive midgut.
The primitive midgut remains connected to the remains of the yolk sac by the vitelline duct(yolk stalk). |
|
|
4 Causes of birth defects |
1. Chromosomal abnormality - aneuploidy - structural abnormalities (alter chromosome segments) 2. Mutations 3. Environmental factors - maternal infections - physical factors - chemical factors - mechanical factors - maternal factors 4. Multifactorial causation: combination of multigenetic and environmental factors |
|
|
5 Principles of Teratology |
1. malformation depends on genotype and how the genotype interacts with the environment. 2. susceptibility to malformation varies depending on developmental stage 3. access of the adverse influence to developing tissues depends on the nature of the influence. 4. Four deviations (death, malformation, growth retardation and functional defect) 5. manifestation of deviant development increases in frequency and degree as dosage increases |
|
|
Clusters of malformations |
If a fetus has one defect then it will most likely have other defects associated with it too. |
|
|
Describe the mesenteries of the primitive gut. |
Foregut: Ventral + dorsal mesentery Midgut + Hindgut: only dorsal mesentery |
|
|
3 Abnormalities of Midgut Development |
- malrotation - omphalocele - gastroschisis |
|
|
What does the rectoanal canal contribute to the formation of? What is developed from the proctodeum? |
Rectoanal canal ---> rectum and upper part of anal canal Proctodeum ---> distal part of the anal canal |
|
|
What does the cloacal membrane become after the urorectal septum divides it? |
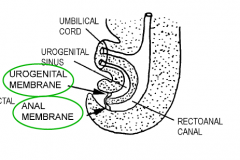
Urogenital and anal membranes
|
|
|
What initiates the development of the liver, gall bladder and pancreas? |
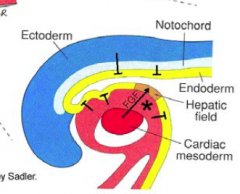
FGF from the cardiac mesoderm signal the endoderm on the distal part of the foregut to grow out. |
|
|
Where do the hepatic sinusoids andstroma (supporting connective tissue), the capsule of the liver, the lesser omentum, and thefalciform, triangular and coronary ligaments all arise from? |
- attenuation of the mesoderm in the ventral mesentery as the liver grows |
|
|
What are the two buds that form from the distal part of the forgut under FGF? |
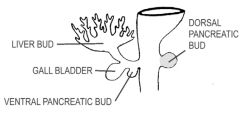
- dorsal pancreatic bud (into d. mesentery) - liver, gall bladder, and ventral pancreatic duct (into v. mesentery) |
|
|
What are some consequences of obstruction of the bowel? |
- Distension proximal to level of obstruction - reduced stool - reflux - polyhydramnios |
|
|
What are the general steps for the formation of the laryngotracheal diverticulum? |
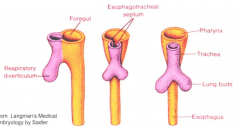
- endoderm lining of foregut makes a groove: laryngotracheal diverticulum - diverticulum pinch inwards to create tracheosophageal ridges - ridges fuse to create tracheoesophogeal septum |
|
|
True or false: Pain sensory fibres do not innervate the visceral pleura but they do innervate theparietal pleura. 2. Where are the visceral and parietal pleuras continuous with each other? |
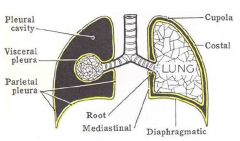
1. True 2. The root of the lung(where the bronchi and vessels enter into the lung from the mediastinum) |
|
|
Pronephric phase (3rd week) |
- vesicles from nephrogenic cord (derived intermediate mesoderm) form pronephric duct - at cervical segments - caudal tip grows and opens into cloaca - pronephric part of nephrogenic cord and duct degenerate. - remaining pronephric duct is called mesonephric duct |
|
|
Mesonephric phase (4th week) |
- thoracic and lumbar segments - mesonephric tubules form and fuse with mesonephric duct - mesonephros degenerates |
|
|
What happens in the Metanephric phase (5th week) |
- ureteric bud outgrows from mesonephric duct - GDNF released from metanephric mass of mesoderm - ureteric bud grows into the mass and releases growth factors to maintain the mass |
|
|
During the 4th week of development where can the Primodial Germ cells be found? Where do they migrate to next and what do they stimulate? |
- the yolk sac near the origin of the allantois - by 6th week enter sex cords - stimulate the further development of gonads |
|
What happens to these structures in males? |
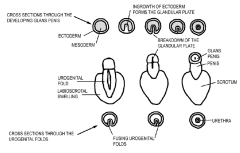
- genital tubercle elongates - urogenital folds get pulled along with urogenital groove in between - glandular plate forms by ingrowth of epithelium on the genital tubercle ---> glans penis - urogenital folds ---fuse---> penile urethra - labiosacral swellings ---> scrotum |
|
|
hypospadias
|
Condition where the urethra is on underside of penis (urogenital folds did not fuse properly) |
|
|
1. What is the name of the mesoderm that forms the developing heart? 2. What does this mesoderm develop into? |
1. Cardiogenic mesoderm - migrates cranially past the neural plate and oropharyngeal membrane. 2. Primary heart fields, which migrates even more crainially to the cardiac crescent |
|
|
Through what process do the primordial chambers of the heart develop?
|
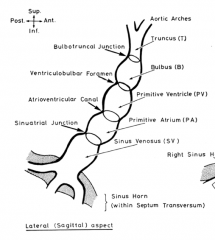
Pre-looping
- Sinus Venosus and primitive atrium will be on the caudal end - Truncus leading to the two aortic arches is on the cranial end. |
|
|
Through what process do the primordial chambers of the heart develop with an apex to the left (levocardia), RV rotated anteriorly and 3D geometry for further development? |

Dextra-looping (to the right) |
|
|
Compare the right and left atria Where are they derived from? |
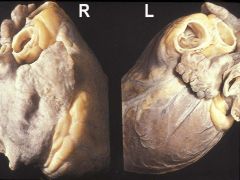
right: conical, triangular and broad left: elongated, serpiginous, with a scalloped lower border Primitive atrium |
|
|
1. What are atrial appendages derived from and what are they a good clue to? 2. What happens to the primary pulmonary vein? |
1. Primitive atrium. Sidedness on the body 2. shortens and disappears so that the pulmonary vein feed directly into the primitive atrium. |
|
|
1. What is the name of the first gap in the developing septum primum? 2. What is the name of the second hole formed and what is the significance of this hole? |
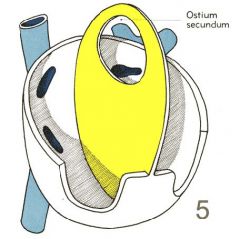
1. Ostium primum 2. Ostium secundum, allows to bypass the ventricles and lungs since in the developing heart receives oxygenated blood via the umbilical vein from the placenta to the right atrium. |
|
|
What layer covers the ostium primum? What does the foramen ovale become when this layer fuses with the septum primum? |
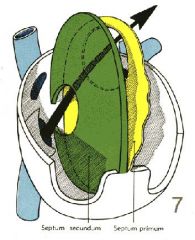
Septum secundum Fossa Ovalis |
|
|
What develops in the Atriventricular junction? What separates the common AV orifice into right and left AV junctions? |
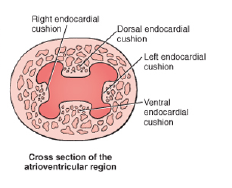
The tricuspid (right) and mitral (left) atroventricular valves develop in the junction. The separation is by endocardial cushions - mediated by neural crest cells |
|
|
What three things need to come together to separate the left and right ventricles? |
muscular wall, endocardial cushion, wall septum |
|
|
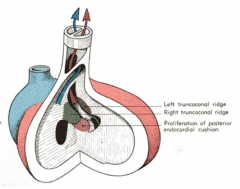
The division of the truncus is formed by?
|
Spiral septum, which separates the pulmonary artery from the aorta.
- mediated by neural crest cells |
|
|
What happens to the mesenchymal cells during the formation of a somite? |

They become polarized and acquire epithelial characteristics:
- elongate and orient around the myocoele (central cavity) - develop apical junction complexes with tight junctions - basement membrane |
|
|
What does the somite break up into? |
- ventromedial somite ---> sclerotome - dorsolateral aspect ---> dermomyotome + myotome |
|
|
What does the myotome portion of the somite split into and what do these portions contribute to the development of? |
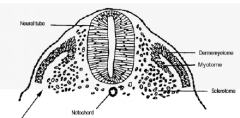
- dorsal (epaxial) myotome ---> back muscles - ventral (hypaxial) myotome ---> muscles of trunk and limbs |
|
|
What is the name of the remaining portion of the somite once the dermomyotome, myotome and sclerotome dissociate? What does this portion develop into? |
Dermatome - the dermatome cells re-acquire their mesenchymal phenotype and mix with the somatic layer of the lateral plate mesoderm to form the dermis |
|
|
True or False: The polarization and differentiation of the somite is not controlled by signals from adjacent tissues |
False.
During the breakup of the somite, the development and differentiation of its components is determined by positional cues in the form of secreted molecules from the notochord and ventral neural tube, the dorsal neural tube and the epidermis and the intermediate mesoderm. |
|
|
Where will the sclerotome cells migrate to and what will each migrated portion form? |
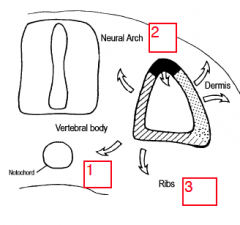
1. Ventromedially to surround the notochord. ---> vertebral bodies and intervertebral discs. 2. Dorsomedially between the neural tube and the surface ectoderm. ---> neural arches ofthe vertebrae and the meninges around the spinal cord. (spina bifida) 3. Ventrolaterally to form the costal processes. The costal processes ---> transverse processes of the vertebrae. In the thoracic region ---> the ribs |
|
|
What forms the annulus fibrosis, nucleus pulposis and bodies of the vertebrae? |
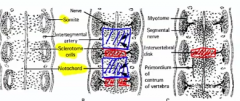
cellular middle portions of each sclerotome pair ---> annulus fibrosis notochord ---> nucleus pulposus intermingling of caudal/cranial ends of somite pairs ---> vertebral body Key point: Discs are segmental, Vertebrae are intersegmental |
|
|
1. Hemivertebra 2. Klippel Feil syndrome |
Defects of Sclerotome Development: 1. only half the vertebra forms. Thesclerotome cells of the caudal part of one somite pair failed to intermingle withthe cells of the cranial part of the following pair on half the vertebrae. 2. fusion of vertebrae |
|
|
What are the different types of spina bifida? |
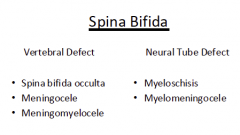
Spina bifida = gap in the vertebral arch of a vertebra. - spinal cord and vertebrae may get involved secondary to the defect in vertebral and neural tube formation, respectively. |
|
|
Spina Bifida: 1. Spina Bifida Occulta 2. Meningocele 3. Meningomyelocele |
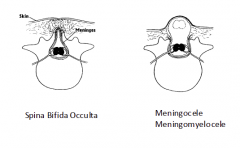
These defects result from abnormal formation of thevertebral arch. 1. most common, asymptomatic 2. Accumulation of CSF in the meningeal spaces surrounding the spinal cord 3. If in meningocele the cord is also herniated, thecondition is called meningomyelocele. |
|
|
Spina Bifida: 1. Myeloschisis 2. Myelomeningocele |
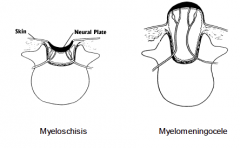
1. open spinal cord (neural plate) - paralysis - failure of neural tube to close (therefore vertebra also can't close). - causes Hydrocephalus 2. CSF accumulates in meningeal space and elevates the neural plate producing a sac. The covering of the sac = neural plate |
|
|
What is FGF 10 expression responsible for and how is it triggered?
|

Somitic/paraxial mesoderm triggers FGF 10 expression in the adjacent lateral plate mesoderm. - this induces the Apical Ectodermal Ridge (AER) between the dorsal and ventral ectoderm. |
|
|
What does the AER stimulate in the underlying lateral plate mesoderm? |

- rapid proliferation, creating the progress zone in the developing limb.
- this forms a self-differentiating system - first cells to leave the progress zone form the proximal limb. |
|
|
What is responsible for the interdigital tissues removal/apoptosis between the digits? |
BMP expression |
|
|
How is the craniocaudal organization of the limbs determined? |
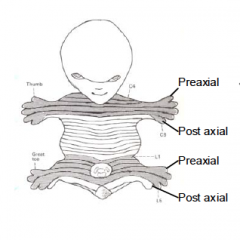
Determined by small area of mesoderm in the caudal part of the limb bud – the Zone of Polarizing Activity (ZPA) - this is in the postaxial mesoderm - identity is formed according to signal strength |
|
|
Where are bone, cartilage and muscles derived from for the limb? |
- Bone and Cartilage is derived from the somatic layer of lateral plate mesoderm - Skeletal muscle is derived from myoblasts that migrate in from the hypaxial part of the somite myotomes. |
|
|
The limbs have a dorsal (extensor) and a ventral (flexor) surface related to the expression of? What represses the expression of this? |
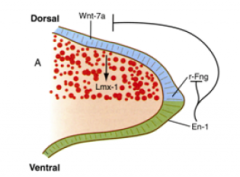
Wnt 7a in the ectoderm on the dorsal side of the limb bud Engrailed (En-1) expression in the ventral ectoderm represses Wnt 7a expression and limits its area of influence |
|
|
What is the Oropharyngeal membrane and what appears here at the 4th week of development? |
- membrane at rostral end where the ectoderm and endoderm are in direct contact. - frontonasal prominence and the pharyngeal arches appear at 4th week |
|
|
What causes the frontonasal prominence? What do the embryonic tissue found in the prominence develop into? |
proliferation of mesoderm cells and arrival of neural crest cells
- mesoderm ---> skeletal muscle cells and endothelium of blood vessels - neural crest cells ---> bone and connective tissue of the face, sensory and autonomic ganglia of head and neck mesoderm + neural crest cells ---> mesenchyme. The neural crest cells contribute mainly to the mesenchyme in the ventral parts of the pharyngeal arches and therefore contribute to the face. |
|
|
What does each pharyngeal arch contain? |
- An artery
- Cartilage - Muscle - A nerve -- 1st arch: trigeminal -- 2nd arch: facial -- 3rd arch: glossopharyngeal -- 4th arch: vagus |
|
|
What does the first pharyngeal arch divide into? |
- Maxillary and mandibular prominences
|
|
|
The ophthalmic division of the trigeminal nerve (V1) grows into the _____________ , the maxillary division (V2) into the _____________ , and the mandibular division (V3) into the_______________. |
frontonasal prominence
maxillary prominence mandibular prominence |
|
|
The oropharyngeal membrane disappears in the 4th week so that the stomatodeum opens up into the pharynx. What are the stomatodeum and pharynx lined with? |
Stomatodeum is lined with ectoderm
Pharynx with endoderm |
|
|
The face and palate develop from? |
The frontonasal prominence and the first pharyngeal arches.
|
|
|
What structures form on the ventrolateral frontonasal prominence? |
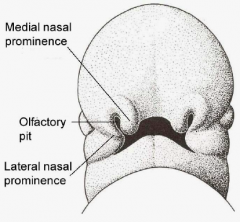
Olfactory placodes ---> nasal pits ---> medial and lateral nasal prominences with an olfactory pit in between. |
|
|
What separates the olfactory pit from the oral cavity? When does this structure separating the two disappear? |
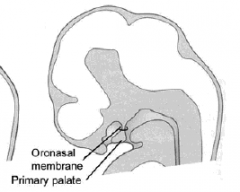
oronasal membrane disappears at 7th week |
|
|
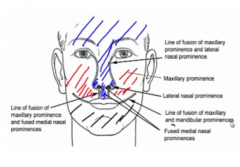
1. The mandibular prominences will merge to form the? 2. The medial nasal prominences will merge with each other to form the? |
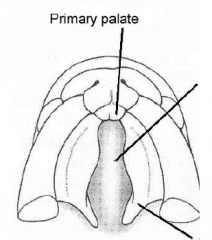
1. lower jaw 2. philtrum of the upper lip and the primary palate (premaxilla – the part that holds the upper incisor teeth). |
|
|
Nasal fin |
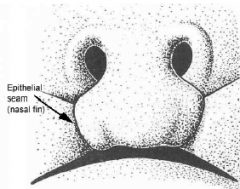
- Found between the medial nasal prominences and the maxillary prominences. - It will break down and the mesenchyme in the cores of each will merge together to complete the continuity of the upper lip. |
|
|
What is the nasolacrimal groove and what forms from it? |
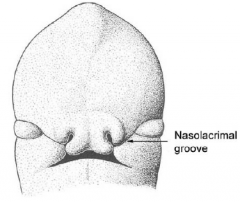
It separates the maxillary and lateral nasal prominences. - ectoderm of groove's floor forms a cord, which canalizes to form the nasolacrimal duct (connects lacrimal sac to inferior meatus of nasal cavity) |
|
|
What will each develop into? 1. Frontonasal prominence 2. Medial nasal prominence 3. Lateral nasal prominence |
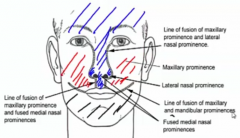
1. Frontonasal prominence – forehead, nasal bridge, nasal septum 2. Medial nasal prominence – primary palate, philtrum of upper lip, tip of the nasalseptum (columella) 3. Lateral nasal prominence – ala of the nose |
|
|
What will each develop into? 1. Maxillary prominence 2. Mandibular prominence |
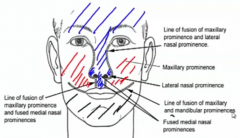
1. Maxillary prominence – maxillae (exclusive of the primary palate) and lateral part ofupper lip 2. Mandibular prominence – lower lip and jaw |
|
|
What are the 2 main sources that develop the palate? |
- The medial nasal prominences form the primary palate - The palatal process of the maxillae form the secondary palate, including the soft palate and the uvula. |
|
|
During the 7th and 8th week, what do the palatal processes fuse with? In what direction does this fusion take place? |
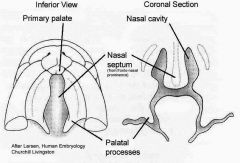
The palatal processes fuse with each other, with the primary palate, and with the nasal septum. Breakdown of the epithelial seams (fusion) between the shelves begins anteriorly and proceeds in a posterior direction. (establishment of mesenchymal continuity). |
|
|
Pharyngeal pouches Pharyngeal grooves |
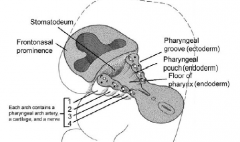
Valleys in between pharyngeal arches.
Pouches are inside (lined with endoderm). Grooves are outside (lined with ectoderm). |
|
|
What is the fate of the first pharyngeal groove and the ectoderm at the bottom of this groove? |
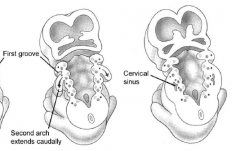
- 1st groove deepens ---> external auditory meatus - the ectoderm at the bottom of the groove becomes the external surface of tympanic membrane |
|
|
What is a cyst found on the medial/anterior border of the sternocleidomastoid is probably a remanent of?
|
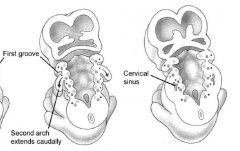
The cervical sinus (created by the second pharyngeal arch) |
|
|
What happens to the pharyngeal grooves (Except for the first groove)? |
The second arch grows caudally and covers the other arches. A cervical sinus is created. Ectoderm-lined. This sinus can later become a cyst on the sternocleidomastoid. |
|
|
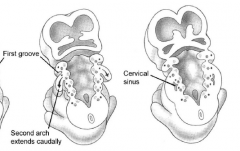
What happens to the first pharyngeal pouch? What does the 2nd pouch form? |
- deepens and meets floor of 1st pharyngeal groove
- forms middle ear and auditory tube - 2nd pouch ---> tonsillar fossa (the depression between the palatoglossal and palatopharyngeal arches occupied by the palatine tonsil) |
|
|
The ear drum separating the middle ear and the external auditory meatus is derived from? |
The endoderm of the first pharyngealpouch and the ectoderm of the first pharyngeal groove. |
|
|
What happens to the 3rd pharyngeal pouch? What does the 4th pouch form? |
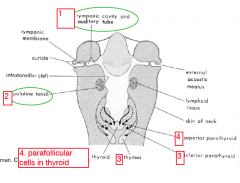
Third pouch – The cells in the ventral part of each pouch cells migrate into theanterior mediastinum to form the thymus. Cells from the dorsal part of each pouchmigrate into the neck forming the inferior parathyroid glands Fourth pouch – cells from the dorsal part migrate into the neck to form thesuperior parathyroids and cells in the ventral part invade the thyroid gland to formthe parafollicular (thyrocalcitonin - secreting) cells. |
|
|
What cartilages do the 4 pharyngeal arches form? |
First arch (Meckle's cartilage) – the mandible, sphenomandibular ligament,malleus and incus Second arch (Reichert's cartilage) – the stapes, styloid process of temporal bone,lesser horn and part of the body of the hyoid Third arch – the greater horn and part of the body of the hyoid Remaining arches – laryngeal cartilages |
|
|
What muscles do the 4 pharyngeal arches form? |
First arch – muscles of mastication, mylohyoid, anterior belly of digastric, tensortympani and tensor palati (innervated by V)
Second arch – muscles of facial expression, posterior belly of the digastric,stylohyoid and stapedius (innervated by VII). Third arch – stylopharyngeus (innervated by IX) Remaining arches – levator palati, muscles of the pharynx and the larynx(innervated by X). |
|
|
1. Truncus arteriosus 2. Aortic sac |
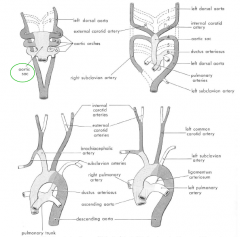
1. Gives rise to - pulmonary trunk artery - Ascending aorta 2. Connects the Truncus arterosus with the aortic arches, which develop into the arteries in the chest and neck. |
|
|
How does the thyroid gland develop? |
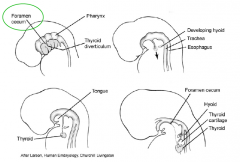
Finger like invagintion at foramen cecum between 1st and 2nd arch, thyroglossal duct, grows down. The distal part expands to form lobes of the thyroid. Proximal part disappears. - If they do not disappear then remnants like the pyramidal lobes of thyroid can be found. |
|
|
Thyroglossal duct cyst |
Ectopic thyroid tissue can sometimes enlarge. |
|
|
How does the pituitary gland (adenohypophysis) develop? |
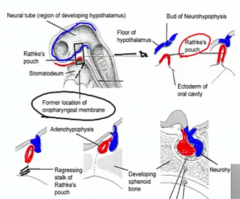
- from the ectoderm of the roof of the stomatodeum. - The neurohypophysis (posterior lobe) develops as a downgrowth neuroectoderm (blue) of the neuraltube in the region of the developing hypothalalmus. |
|
|
Describe the development of the tongue |

Lateral lingual swellings ---> Anterior 2/3 from 1st arch – trigeminal nerve - VII will contribute taste to anterior 2/3 Posterior 1/3 from 3rd and 4th arches (glossopharyngeal and vagus) Skeletal muscle migrates in from the occipital somites (Hypoglossal) |
|
|
From the venous (caudal) pole to the arterial (cranial) pole what are the primitive chambers and what do they develop? |
‐ Primitive atrium (will give rise to both left and right atria) ‐ Primitive ventricle (will give rise to LV) ‐ Bulbus cordis (will give rise to RV) ‐ Truncus (the main outflow, which will split into aorta and pulmonary artery) |