![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
33 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What is the normal cardiac axis? |
Waves of depolarisation generally spreadthrough the heart from 11 o’clock to 5 o’clock. Thisdirection of spread of the signal is known as the cardiac axis. Itcreates apositive R wave in lead II (and I and III) It can be estimated using leads I-III or calculated to the nearest 30 degrees |
|
|
|
How do you calculate the axis in degrees? |
1) Find equipolar lead on ECG 2) The axis is at right angles to the equipolar lead. Find the + and - lines at 90 degreee angle 3) Which of these angles/lines is present on your ECG as a lead? 4)On your ECG, is the QRS + or -? 5) This is accurate to 30 degrees |
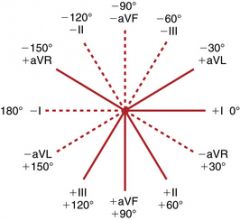
All augmented leads are perpendicular to numbered lead I p aVF II p aVL III p aVR |
|
|
What is the range for a normal axis? |
+90 to -30 degrees |
|
|
|
What are the ranges for the different deviations on the axis? |

|
|
|
|
Why do we look for the equiphasic/equipolar lead? |
Remember, if a lead is equiphasic/polar, then we know that the direction of conduction is exactly perpendicular to the direction of that lead. |
|
|
|
What does an equipolar lead look like? |

|
|
|
|
Which lead does each line represent in the hexaxial diagram |
|
|
|
|
What are the causes of LAD? |
L anterior Hemioblock Myocardial Infarction (Nice to know: WPW with R pathway, VT, Pacing, Hyperkalaemia, Emphysema) |
|
|
|
What are the causes of RAD? |
Normal for tall thin adults RVH with chronic lUng disease Ant-Lat MI (Nice to know: L post hemiblock, pulm embolis, WPW with L pathyway) |
|
|
|
What causes axis to be in No Man's Land? |
Emphysema Hyperkalaemia Pacing Lead Transposition |
|
|
|
How do we diagnose LA hemiblock (fascicular block)? |
-45 degree axis small Q wave with tall R wave (qR complexes in left sided leads) in Lead I and and small r with tall S (rS complexes in inferior leads) in lead III. Slightly prolonged QRS |
|
|
|
Describe normal sinus rhythm |
QRScomplex is less than 0.12 s wide, preceded by a P-wave, PR interval 0.12-0.20 sec and constantwhen A-V conduction normal. P:QRS ratio 1:1. No notches. Pattern inchest leads: S decreases, R increases. Small Q waves normal, esp inL-sided leads |
|
|
|
Describe the findings in RVH |
Caused by pulm hpt R axis deviation (can fall in NML), Tall R in V1 |
|
|
|
In RAH what are the findings in P wave? |
Peaked P in II = RAH |
|
|
|
What are the findings in right ventricular strain? |
Delayed precordial transition zone with tall S in V5 and V6, Inverted T and ST suppresion in V1-3 |
|
|
|
Describe the findings in RBBB |
Tall R in V1 Notched, no right axis deviation, wide QRS if completely blocked but may be narrow if incomplete SVR |
|
|
|
What are the findings in LVH? |
Tall R in V6, Deep S in V1 |
|
|
|
What are the findings in a LBBB?
|
SVR with wide QRS Notched in V6 |
|
|
|
Describe Atrial Premature Beat |
The impulse is discharged prematurely bysome irritable focus in the atria giving rise to a distorted P wave (wide,narrow, notched, inverted or superimposed on the preceding T wave). Thefurther from the SA node the ectopic focus is, the more abnormal will be P'configuration. PR interval normal or slightly prolonged. PrematureP followed by QRS less than 0.11 sec except when very premature P is notconducted. |
|
|
|
Is the pause in APB compensatory of non-compensatory? |
The pause between APB and the next sinus beat is usually noncompensatory i.e. the RR interval between two QRS enclosing APB is less than twice the normal RR interval |
|
|
|
What are the different names given to Ventricular-Extra Systoles?
|
PVCs PVBs |
|
|
|
What is VES? |
Anirritable focus in ventricle fires prematurely, spreads to opposite ventricleproducing a bizarre pattern |
|
|
|
What does a VES that originates in the LV look like? |
Wave spreads slow to R ventricle, so PVC looks like RBBB in V1 |
|
|
|
What does a VES that originates in the RV look like? |
Wave spreads slow to L ventricle, so PVC looks like LBBB in V6 |
|
|
|
What are the other characteristics of VES? |
P-wave buried notch/ deformity T-wave opposite side of QRS Can be Unifocal or multifocal Have compensatory pause (the RR interval between two QRS enclosing APB is more than twice the normal RR interval) |
|
|
|
When are you at risk of VT/VFib with PVCs? |
More than 6 PVCs/min Multifocal Bigeminy, trigeminy Couplets Runs of VT R on T |
|
|
|
What should we remember about the shapes of PVCs? |
Different shape = different origin |
|
|
|
Why do a sinus complex, a PAC and a PJC all have similarly shaped QRS complexes? |
QRSshape often reflects where the impulse entered the ventricular conductionsystem. As far as the ventricles are concerned, pacemakers in the sinusnode, atria, and the junction (normally) all share the same path. |
|
|
|
Why can multifocal PVCs look different? |
Pacemakersin the ventricular conduction system are not limited to one location; they canoccur in a variety of places. These different places should producedifferent QRS complexes. We should assume, because of theirdissimilarity, that these PVCs each originated from a different part of theventricular conduction system. |
|
|
|
What is bigeminy and what is trigeminy? |
Bigeminy — every other beat is a PVC. Trigeminy — every third beat is a PVC. |
|
|
|
What are couplets? |
two consecutive PVCs |
|
|
|
What is a run/salvo? |
Salvo(as in barrage) is used to describe theoccurrence of multiple premature complexes in a row Should be considered more in terms of VT |
|
|
|
What is the R on T phenomenon? |
PVC occurs during the preceeding T wave, known as ‘R on T’ phenomenon. |
|