Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
51 Cards in this Set
- Front
- Back
|
What is the first basic principle of dysrhythmias
|
to identify and treat precipitating factors
|
|
|
What are the 4 causes of Dysrhythmias
|
-automaticity
-excitability -refractoriness -conduction |
|
|
What are different manifestations of cardiac dysrhythmias
|
-ectopic pacemakers
-heart block -re-entry (tachy dysrhythmias) -any combination of the above |
|
|
defined as the ability to spontaneously generate an action potential and the speed that action potentials are generated
|
automaticity
|
|
|
What 3 things "enhance automaticity": brings the RMP closer to the TP
This will do what to HR? |
-Increased slope of phase 4
-Depolarize the RMP -Hyperpolarize the TP * Increases HR |
|
|
What 3 things "depress automaticity": makes the RMP and TP further apart
This will do what to HR? |
-decrease in slope of phase 4
-Hyperpolarize the RMP -Depolarize the TP * Decreases HR |
|
|
Defined as "any area of the myocardium that generates an AP other than the SA node
|
Ectopic Pacemakers
|
|
|
Defined as the ability of the cardiac cell to respond to stimulation by depolarization
|
Excitability
|
|
|
Defined as the period of time when the myocardial cell will not respond to an action potential b/c the Na or Ca inactivation gate remains closed
|
Refractory Period
|
|
|
rebuff
|
reject (someone or something) in an abrupt or ungracious manner
|
|
|
Defined as the ability to cause an adjoining cell to depolarize and the speed by which the adjoining cell is depolarized
|
conduction
|
|
|
What part of the refractory period occurs on the downstroke of T
|
Relative
|
|
|
**bold**
defined as re-excitation of the cardiac tissue from the "SAME" cardiac impulse using a circuitous pathway. |
Re-entry or circus movements
|
|
|
What are the two requirements for Re-entry
|
-imbalance between conduction and refractoriness
-Unidirectional block |
|
|
What are some causes of Re-entry?
|
-Elongation of the conduction pathway...i.e Afib
-Decreased velocity of conduction of the cardiac impulse (like after an MI) -shortened refractory period |
|
|
**If you have a hyperpolarized RMP; would it increase or decrease HR?
|
decrease HR
|
|
|
**If you have a Hyperpolarized TP; would it increase or decrease HR?
|
Increase HR
|
|
|
What do you think 1st if you see a wide QRS?
|
BBB
|
|
|
If QRS is < 0.12 secs the complex is ___________
|
supraventricular
|
|
|
What leads are P waves normally upright in?
|
I, II, aVF, and V4-6
|
|
|
During anesthesia, p wave morphology is commonly seen in which lead?
|
II
|
|
|
If S-A dysrhythmia is associated with physiologic events it is called
|
phasic sinus rhythm
|
|
|
What is the Rx for Sick Sinus Syndrome?
|
permanent pacer and antidysrhythmics
|
|
|
**What is the difference between a junctional rhythm and a accelerated junctional rhythm?
|
Accelerated just means rate is over 60
|
|
|
**What drugs would you "NOT" use in Wolff-Parkinson-White Syndrome?
|
-verapamil
-diltiazem -digoxin These drugs may put pt in V-tac |
|
|
Review fig 4-1 pg 20
|
..
|
|
|
What type of heart block:
-every P wave produces a QRS complex -amt of time required to produce the QRS complex is prolonged ( exceeds_____sec) |
1st degree
> 0,20 secs |
|
|
What type of Heart block:
the relationship between P waves and QRS complexes is altered in that some P waves conduct, and some do not |
second degree HB
|
|
|
In this type of Heart Block "there will never be fixed P-R intervals
|
3rd degree HB
|
|
|
Type of rhythms where the "p waves are inverted" Rate is typically 40-60 bpm, but can be less
|
classic junctional rhythm
|
|
|
Type of rhythm where the "p waves are inverted" Rate is > 60 bpm
|
junctional tachycardia
|
|
|
What is very helpful in treating PVC's (stabilizes membrane)
|
Magnesium
|
|
|
**This rhythm is always associated with prolonged QT interval
|
Torsades
|
|
|
* What is the most common cause of PEA in Anesthesia
|
Hypovolemia
|
|
|
*In what leads would you see a RBBB
|
v1-2
|
|
|
*In what leads would you see a LBBB
|
V5-6
|
|
|
**________ makes the diagnosis of an old anterior MI impossible
|
LBBB
|
|
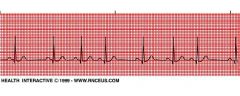
What Rhythm is this?
|
Sinus Arrhythmia
Key Characteristic: irregular rhythm! everything else normal |
|
|
What rhythm?
|
"Sinus Arrest"
Causes: -Obstruction of RCA -Acute MI -Dig toxicity -Repeat dose of Succinylcho |
|
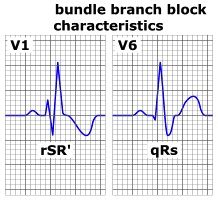
what type of block
|
right bundle branch block
"triphasic pattern" rSR in V1-2 Wide S wave in V5-V6 |
|
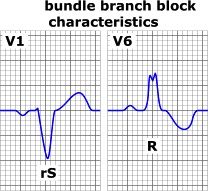
What type of block
|
left bundle branch:
Bisphasic rS in V1-2 Bisphasic rR in V5-6 |
|
|
What rhythms are extremely common under anesthesia
|
atrial and nodal rhythms
|
|
|
What is the criteria for diagnosis of 1st degree A-V Block
|
Fixed PR intervals
PR interval > 0.2 secs |
|
|
What is the criteria for diagnosis of Mobitz II
|
Not all P waves have QRS complexes, P to P interval is regular
|
|
|
What is the criteria for diagnosis of 3rd Degree A-V Block
|
* No fixed PR intervals
P to P interval is regular R to R interval is regular |
|
|
What is the most prevalent aspect in regards to a strip that shows Torsades de Pointes
|
Always associated with a prolonged QT interval
|
|
|
If the ECG show BBB with a QRS 0.10-0.11, this is known as?
|
incomplete BBB
|
|
|
if the ECG shows BBB with a QRS >= 0.12, this is known as?
|
Complete BBB
|
|
|
The following diseases are common causes of which type of BBB
-PE -Pulmonary HTN -WPW |
Right BBB
|
|
|
What type of block is usually an indication of organic heart disease?
|
L BBB
|
|
|
Pt's with acute MI who develop LBBB are at high risk for?
|
complete heart block and temporary pacing is indicated
|