![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
182 Cards in this Set
- Front
- Back
|
Parts of the Axial Skeleton |
Vertebral Column, Skull, Ribs, Sternum |
|
|
Regions of Vertebral Column |
Cervical (7), Thoracic (12), Lumbar (5), Sacral (5 Fused), Coccyx (4 Fused) 33 Total |
|
|
Pairs of Spinal Nerves in Vertebral Column Regions |
Cervical (8), Thoracic (12), Lumbar (5), Sacral (5), Coccyx (1) 31 Total Pairs |
|
|
Functions of Vertebral Column |
- Protect Spinal Column and Nerves - Posture, supports body weight - Movement- Extension, Flexion, Lateral Flexion, Rotation -Provides flexible axis for neck and torso |
|
|
Primary Curvatures |
- Thoracic and sacral - Anteriorly Concave - Develop early in womb |
|
|
Secondary Curvatures |
- Cervical and Lumbar - Concave Posteriorly - Develop in infancy - Cervical- develops when an infant starts to lift their head - Lumbar- develops due to bipedal nature, crawling, walking, standing |
|
|
Thoracic Kyphosis |
Exaggerated thoracic curvature, "Humpback" deformity |
|
|
Lumbar Lordosis |
Exaggerated Lumbar curvature, "swayback" deformity |
|
|
Scoliosis |
Lateral deviation of column often coupled with a rotational component - Forward Bend Test: Uneven shoulders and waist, appears to be leaning |
|
|
Body of vertebrae |
Anteriorly Moving inferiorly, bodies get larger to support more body weight Articulate with intervertebral discs |
|
|
Vertebral Arch |
"Neural Arch" Posterior to body Formed by pedicles and laminae |
|
|
Pedicles |
Components of vertebral arch attach to body |
|
|
Laminae |
Attached to pedicles Flattened or arched parts of vertebral arch Form roof of spinal canal |
|
|
Transverse Processes |
Lateral at the junction of the pedicle and laminae |
|
|
Spinous Process |
posterior process where the 2 laminae fuse together |
|
|
Superior Articular Processes |
Smooth surfaces that articulate with the Inferior articular processes |
|
|
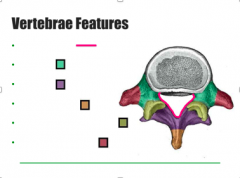
Green- Pedicles Purple- Laminae Orange- spinous process Yellow- Sup articular processes Red- Transverse Processes Pink- Vertebral Arch |
|
|
Vertebral Foramen/Spinal Canal |
Formed by vertebral arch and posterior surface of body Contains Spinal Cord |
|
|
Facet Joints (basics) |
Synovial Joints articulation of superior and inferior articular processes Different orientations of the regions allow for different movements |
|
|
Intervertebral Foramen |
Formed by superior and inferior vertebral notches allow passage of blood vessels and spinal nerves |
|
|
Cervical Vertebrae |
Small bodies Transverse Foramina (not found in any other vertebrae) allow passage of vertebral vessels that supply blood to the brain |
|
|
C7 |
Vertebral Prominens Most prominent cervical spinous process Flexion of the neck allows for easy palpation |
|
|
C1 |
Atlas no vertebral body or spinous process Superior Articular Processes articulate with occipital condyles of skull forms the atlanto-occipital joint, allows anterior flexion and posterior extension |
|
|
C2 |
Axis Dens Process- portion of the C1 body that incorporates into the C2 during development Atlanta-axial joint (C1-C2) allows for rotation |
|
|
Thoracic Vertebrae |
Articulate with the 12 pairs of ribs Long, slender spinous processes slant inferiorly |
|
|
Thoracic Articulation with Ribs |
head of ribs Superior articular facet articulates with the body of the superior thoracic vertebrae Inferior articular facet articulates with the body of the same numerical thoracic vertebrae Tubercle of rib articulates with the transverse process of the same numerical T vertebrae |
|
|
Lumbar Vertebrae |
Very large bodies Robust spinous processes projecting posteriorly |
|
|
Lumbar Puncture/Spinal Tap |
Gaps b/w adjacent lumbar spinous processes allow especially in flexion Allows access to the spinal cord contents typically b/w L3-L4 Lumbar anestesia b/w L4-L5 |
|
|
Lumbosacral Angle |
L5-S1 bodies |
|
|
Sacrum |
5 fused no intervertebral foramen 4 pairs of Ant and Post Foramina allow transmission of ventral and dorsal rami of sacral spinal nerves |
|
|
Sacral Canal |
continuation of vertebral canal ends at sacral hiatus, bound by cornua which allow for easy palpation, covered by sacrococcygeal ligament |
|
|
Coccyx |
4 fused small focal point for muscle and ligament attachment in perineal area which help stabilize the pelvic diaphragm |
|
|
Intervertebral Discs |
b/w bodies of vertebrae distribute force and weight Provide flexibility to column named by the two vertebrae they articulate |
|
|
Thoracic discs |
thin, uniform shape |
|
|
Cervical and Lumbar discs |
thicker anteriorly, contributing to secondary curvatures more susceptible to herniation |
|
|
Components of IV Discs |
Annulus Fibrosus-outer fiber cartilaginous ring that serves as structural support Nucleus Pulposus- Gel central mass, shock absorber, high water content that decreases throughout the day and as you age |
|
|
Cervical Facet Joints |
Face superiorly and inferiorly allow flexion and extension some lateral flexion very limited rotation |
|
|
Thoracic Facet Joints |
Ant and Post orientation Restrict flexion and extension permit rotation some lateral flexion but the ribs inhibit it |
|
|
Lumbar Facet Joints |
Medial and lateral orientation restricts rotation allows flexion, extension, lateral flexion |
|
|
Palpable Surfaces of Back |
C7- vertebral prominens T1- at inferior angle of scapula Acromium process of scapula spine of scapula superior angle of scapula medial border of scapula Iliac Crest- L4 |
|
|
2 main types of back muscles |
Extrinsic (superficial) and Intrinsic (deep) |
|
|
Extrinsic Muscles |
innervated by ventral rami (except trapezius is cranial nerve 11) Trapezius, Latissimus Dorsi, Levator Scapulae, Rhomboid Major and Minor Serratus Posterior Superior & Serratus Posterior Inferior are involved in respiration because they're attached to ribs (deep to Rhomboids and Lats respectively) |
|
|
Triangle of Auscultation |
Small region free of overlying muscle b/w trapezius, Lats, and medial border of scapula allows for optimal use of stethoscope to hear sounds of thoracic cavity |
|
|
Intrinsic Muscles of the Back |
Innervated by dorsal rami often injured (pain and limited mobility) T and L region enclosed by Thoracolumbar Fascia Primarily extend column secondary role in lateral flexion and rotation divided into superficial, intermediate, and deep |
|
|
Superficial Intrinsic Muscles |
Splenius Capitis and Splenius Cervicis Contracted bilaterally, extend the neck contracted unilaterally, ipsilateral lateral flexion and rotation |
|
|
Intermediate Intrinsic Muscles |
Erector Spinae divided into Medial, intermediate, and lateral Contracted bilaterally, extend column Contracted unilaterally, ipsilateral lateral flexion and rotation |
|
|
Medial Erector Spinae |
Spinalis (Thoracis, Cervicis, Capitis) Origin: Iliac Crest, Sacrum, Lumbar and Sacral spinous processes Insertion: Spinous Processes |
|
|
Intermediate Erector Spinae |
Longissimus (Thoracis, Cervicis, Capitis) Origin: Iliac Crest, Sacrum, Lumbar and Sacral spinous processes Insertion: Transverse Processes and Mastoid Processes |
|
|
Lateral Erector Spinae |
Iliocostalis (Lumborum, Thoracis, Cervicis) Origin: Iliac Crest, Sacrum, Lumbar and Sacral spinous processes Insertion: Ribs and Transverse Processes |
|
|
Deep Intrinsic Muscles |
Transversospinalis divided into superficial, intermediate, and deep Located in the gutter of transverse and spinous processes span entire column but prominent in different areas Bilateral contraction, extend and stabilize column Unilateral contraction, Contralateral Rotation |
|
|
Superficial Transversospinalis |
Semispinalis Prominent in Cervical Region |
|
|
Intermediate Transversospinalis |
Multifidus Prominent in Lumbar Region |
|
|
Deep Transversospinalis |
Rotatores Prominent in Thoracic Region, high amount of rotation in this region |
|
|
Pelvis |
Ilium, Pubis, Ischium |
|
|
Palpable surfaces of Ilium |
Iliac Crest, Anterior Superior Iliac Spine |
|
|
Palpable surfaces of Pubis |
Pubic Symphysis, Pubic Tubercle |
|
|
Vertebral level of the umbilicus |
L4- in fit people Can vary in people who are unfit |
|
|
Median plane of the abdomen |
splits the ab. into equal left and right sections From xiphoid process down to pubic symphysis |
|
|
Transumbilical plane of the abdomen |
Horizontal plan along the L4 level (umbilicus) Is also the level of the Iliac Crest |
|
|
4 quadrants of the abdomen |
RUQ, LUQ, RLQ, LLQ |
|
|
Transpyloric Plane of the Abdomen |
Passes through the L1 lvl, through the pyloris of the stomach |
|
|
Abdominal Fascia Layers |
Skin Camper's Fascia- fatty, subcutaneous tissue Scarpa Fascia- Membraneous layer Ext. Oblique Int. Oblique Transverse Abdominus (Investing deep fascia separates muscle layers) Transversalis Fascia Extra peritoneal fat parietal peritoneum |
|
|
Scarpa Fascia |
Helps to prevent the spread of infection from ab. to lower limbs Attaches to iliac crest, inguinal ligament, pubic symph. |
|
|
Abdominal Muscle functions |
Maintain posture movements of the torso protect organs also recruited during strenuous exertion increase intra-abdominal pressure for digestive and waste release and childbirth |
|
|
Abdominal Muscle names and pattern of fibers |
(Superficial -> Deep) Ext. Oblique- runs diagonally down from post to ant Rectus Abdominus- run longitudinally Int. Oblique- runs _|_ to ext. oblique Transverse Abdominus- run horizontally *Alternating fibers allows for extra support |
|
|
External Oblique origin and insertion |
O: Ribs 5-12 I: Iliac Crest, Pubic Tubercles, Linea Alba |
|
|
Rectus Abdominus appearance |
Belly of muscle is interrupted by tendonis intersections for the 6 pack look |
|
|
Internal Oblique origin and insertion |
O: Inguinal ligament, iliac crest, thoracolumbar fascia I: Linea alba, conjoint tendon of pubic crest, ribs 10-12 |
|
|
Transverse Abdominus origin and insertion |
O: Iliac crest, inguinal ligament, thoracolumbar fascia, costal cartilage of ribs 7-12 I: Xiphoid process, lines alba, pubic crest, conjoint tendon of the pubic crest |
|
|
Rectus Sheath |
Aponeurosis of the EO, IO, TA that surround and cover the RA. Anterior: all of EO and 1/2 of IO Posterior: 1/2 IO and all of TA |
|
|
Linea Alba |
Runs vertically along midline formed by fibers of the rectus sheath fusing at the midline |
|
|
Arcuate Line |
1/3 the distance from umbilicus to pubic bone formed from the rectus sheath -all aponeurosis run anteriorly to RA leaving only the transversalis fascia deep to the RA - Lack of fascia leads to herniations |
|
|
Nerves of the Abdominal muscles and skin |
Ventral Rami of the intercostal nerves of T7-T11 Subcostal nerve of T12 L1 iliohypogastric and Ilioinguinal nerves |
|
|
Pattern of abdominal innervation |
Innervation occurs in segments damage to one nerve/segment will not paralyze whole muscles weakness of a segment allows protrusion of abdominal contents (herniation) |
|
|
Location of abdominal dermatomes |
Superior to umbilicus: T7-T9 dermatomes @ umbilicus: T10 inferior to umbilicus: T11, T12, L1 These are important for spinal nerve testing and referred pain |
|
|
Posterior intercostal/subcostal arteries |
Branch from 10th and 11th intercostal arteries supply the lateral portion of the ab. wall |
|
|
Superior epigastric artery |
Within the rectus sheath deep to RA Branch from the Internal Epigastric artery Collaborates with the Inf. Epi. Artery via Anastomosis |
|
|
Inferior epigastric artery |
within the rectus sheath deep to RA Branch from Ext. Iliac Arteries Collaborates with the sup. epi. artery via anastomosis |
|
|
Superficial Epigastric artery |
Branches from the femoral artery *Located in superficial fascia* (not like the other arteries) Course directly towards the umbilicus |
|
|
Superior Epigastric Vein |
Sup. to umbilicus drains to superior VC |
|
|
Inferior epigastric vein |
Inferior to umbilicus drains to Inferior VC |
|
|
Relationship of Superior and Inferior Epigastric Veins |
Often form venous plexi and collaborate via anastomosis Caval-Caval Anast. |
|
|
Caval- Caval Anastomosis |
When one route is blocked, blood takes an alternate route back to heart Blockage causes back flow and increased blood volume in veins causing distension of veins Example: If inferior epigastric blockage 1.Reroute to common iliacs 2.To superficial epigastric veins 3.To lateral Thoracic veins 4.Subclavians 5. Superior VC to heart |
|
|
Portal- caval Anastomosis |
Paraumbilical veins (drain mortally) and Superficial epigastric veins (drain to Inf. VC) -Blockage in Liver causes back flow through the paraumbilical veins, towards umbilicus, through the superficial epigastric veins, to the Inf. VC -Portal Blockage causes distension in veins radiating from umbilicus (caput medusae) |
|
|
Superficial lymphatic drainage of the Ant. Ab. Wall |
-Contains NO lymph from organs -Superior of transumbilical plane (L4) drains to Axillary Nodes -Inferior of transumbilical plane drains to Superficial Inguinal Nodes -If infection in one of these areas, the associated Nodes will swell (though other lymph does flow to these Nodes) |
|
|
Groin Region |
Marked by the inguinal ligament (Inferior to ligament) |
|
|
Inguinal Ligament |
-Most inferior portion of Ext. Ob. aponeurosis -spans from Ant. Sup. Iliac Spines to Pubic tubercles -Superior to Ligament is the Inguinal Canal |
|
|
Inguinal canal |
Superior to the midpoint of the Inguinal ligament Consists of Internal and External Rings |
|
|
Deep Internal Ring |
-Entrance to the canal -Superior to the midpoint of the Ing. Lig. -Lateral to Inferior epigastric vessels |
|
|
Superficial External Ring |
-Exit of ing. canal -slit-like opening within the ext. obl. aponeurosis -superiolateral to pubic tubercle -Site of weakness of Ant. Ab. Wall -Increases in intra-abd. pressure will close canal |
|
|
Male Inguinal canal |
-Testes develop in Post. Abd. wall -must drop to scrotum through the ing. canal -gubermaculum lig. attaches testes to scrotum -over 9 mos. the lig. pulls the testes down, pulling vessels, nerves, lymphatics, vas deferens, forming the spermatic cord -Testes take on fascial coverings of abd. wall (from int. to ext. = transversalis->TA->Int. Obl.->Ext. Obl.) |
|
|
Female Inguinal Canal |
Ovaries form in post. abd. wall -gubermaculum pulls them down (connects ovaries with uterus and labium majora) - B/w ovaries and uterus as adult = Ovarian ligament -B/w uterus and labium major as adult = Round Lig. only part that passes through the canal *Canal is much narrower than males, less herniations* |
|
|
Inguinal Canal Nerve Contents |
-ilioinguinal nerve Branches from L1 spinal nerve Provides sensory from the inguinal region & labium majora & scrotum -Genital branch of the genitofemoral nerve Branches from L1, L2 Sensory info from ing. region, labium majora, scrotum Motor Inn. to the cremaster muscle (covers the spermatic cord and testes) |
|
|
Inguinal Hernias |
Other internal structures that pass through/into the canal that shouldn't Protrusion of abd. viscera through the abd. wall Occurs more in males Direct and Indirect |
|
|
Indirect (congenital) Hernias |
Most Common Mass enters the DEEP RING, LATERAL to the inf. epigastric vessels Passes through the canal becoming enclosed in fascia May exit the superficial ring and enter the scrotum or labium majora |
|
|
Direct (acquired) Hernias |
Involve area of weakness called Hesselback's triangle Mass (possibly intestine) pushes into peritoneum and transversalis fascia MEDIAL to inf. epigastric vessels Enters Ing. canal through post. abd. wall |
|
|
Indirect vs. Direct Hernias |
Indirect = Lateral to inf. epi. vessels, and through the deep ring Direct = Medial to inf. epi. vessels, does not enter deep ring |
|
|
Abdominal Cavity |
Continuous with pelvic cavity separated from thoracic by diaphragm Lined with peritoneum - Serous membrane that lines cavity and organ walls, helps hold organs in place |
|
|
Parietal Peritoneum |
Lines internal aspect of Abd-pelvic cavity Receives somato-sensory info from the nerves in the walls Pain, Temp, touch pain is usually acute and localized adhesions from surgery can be very painful |
|
|
Visceral Peritoneum |
Lines outer surfaces of organs Innervated by visceral innervation Sensitive to stretch and ischemia Lacks Somato-sensory inn. (no pain, temp, touch) |
|
|
Peritoneal Cavity |
Lies between the parietal and visceral peritoneum Called "peritoneum space" though there isn't really any open space It contains a thin layer of fluid that keeps surfaces moist and lubricated- aids in movement |
|
|
Peritoneal Effusion (Ascites) |
Fluid accumulation in peritoneal space caused by infections, metastasis of cancer cells, perforations of GI tract Fluid can compress organs, preventing proper function |
|
|
Retroperitoneal Space |
B/w Parietal Peritoneum and Muscles of Post Abd. Wall Contains fat, Abd. Aorta, Inf. VC, and organs (kidneys) Organs are deep to parietal peritoneum (retroperitoneal) |
|
|
Gut Tube Development |
Abd. organs develop from embryonic gut tube Become inviscerated in the parietal Peritoneum Intra- vs Retroperitoneal |
|
|
Intraperitoneal Organs |
Have Mesentery Suspend an organ from the peritoneal wall or another organ *Are Mobile* |
|
|
Mesentery |
Double layer of visceral peritoneum Nerves and vessels travel through to the organs Acts as protection for nerves and vessels |
|
|
Retroperitoneal Organs |
Lack Mesentery Primary vs Secondary Retroperitoneal Not Mobile |
|
|
Primary Retroperitoneal |
Develop within the retroperitoneal space and stay there Only covered anteriorly with peritoneum Not Mobile |
|
|
Secondary Retroperitoneal |
Completely covered with visceral peritoneum early in development but become pushed up against the Post. peritoneal wall, losing mobility. Anchored |
|
|
Intra- and Retroperitoneal Orientation in Adb. Cavity |
Usually alternate moving Superiorly and Inferiorly so that theres areas of mobility and areas of anchoring |
|
|
Omenta |
Mesentery associated with the stomach Greater and lesser |
|
|
Greater Omenta |
Associated with the Greater (Inferior) Curvature of the stomach, extending down like an apron covering the intestines -Can form Mental Adhesions to wall off any inflamed organs, protecting the rest of the organs |
|
|
Less Omenta |
Associated with the Lesser (Superior) Curvature of the stomach |
|
|
Divisions of the Gut Tube |
Foregut, Midgut, Hindgut Organs of divisions share a common blood supply, venous and lymphatic drainage, and innervation |
|
|
Foregut derivatives |
esophagus, stomach, proximal duodenum, Liver, pancreas, gallbladder |
|
|
Foregut Blood supply |
Celiac Trunk from Abd. Aorta |
|
|
Foregut Venous Return |
Gastric and Splenic Veins |
|
|
Foregut Lymphatic Drainage |
To Celiac Nodes surrounding the Celiac trunk |
|
|
Esophagus of Abd. |
1-1.5 cm. long Passes through the Esophageal Hiatus of Diaphragm @ T10 Diaphragm acts as sphincter Intraperitoneal |
|
|
Hiatal Hernia |
When esophagus or part of the stomach gets pushed superiorly through the esophageal hiatus. No symptoms usually sometimes heart burn and chest pain that resembles MI Same referred pain pattern as heart (why its confused with MI) |
|
|
Stomach Location and Classification |
Foregut LUQ Intraperitoneal |
|
|
Curvatures of Stomach |
Greater and Lesser |
|
|
Stomach Regions/Features |
Cardia- Narrow Proximal Opening Fundus- Superior, dome-shaped, Inferior to Left dome of Dia. Body- Largest area, b/w Fundus and Pylorus Pylorus- Distal part has pyloric sphincter Rugae- Folds of gastric mucosa present when stomach is empty |
|
|
Pyloric Sphincter |
L1 level (Transpyloric Plane) Circular Smooth muscle controls release of content into the duodenum Powerful associated with infant projectile vomitting |
|
|
Gallbladder Location and Classification |
Foregut RUQ Inferior aspect of Right lobe of liver Intraperitoneal |
|
|
Gallbladder Functions |
Stores bile produced by liver After meals empty/before meals full Squeezes bile into small intestine via ducts Bile helps digest fats Can be removed -nonessential, usually no effect, some diarrhea and lack of fat absorption |
|
|
X-ray of stomach |
Fundus is distinguishable because of gas bubble |
|
|
Referred Pain of Stomach |
Anterior- just below sternum by xiphoid process Posterior- Midline of thoracic vert. b/w scapula |
|
|
Proximal Duodenum Location |
Foregut RUQ |
|
|
4 parts of the Duodenum |
Foregut: -Superior (1st)- Intra, heptoduodeneal ligament Along transpyloric plane @ L1 -Descending (2nd)- Sec. Retro., no mesentery Curves around head of pancreas Midgut: -Horizontal (3rd) -Ascending (4th) |
|
|
Pancreas Location and Classification |
Foregut RUQ&LUQ Secondary Retro. Posterior to stomach Duodenum on Right, Spleen on Left Has Head, Body, and Tail |
|
|
Pancreas Referred Pain |
Similar to stomach (Just below sternum) Only Anteriorly May indicate injury or pancreatitis |
|
|
Liver Location and Classification |
Foregut RUQ- Mainly, LUQ- partially Deep to ribs 7-11 Intraperitoneal- covered in visceral peritoneum except the part adjacent to diaphragm |
|
|
Falciform Ligament |
Attaches Liver to Ant. Abd. Wall Divides the liver into the large right lobe and small left lobe |
|
|
Liver and Gallbladder Refered Pain |
Liver Inflammation irrates Diaphragm, Pain from Dia. is sent up to the Right shoulder Anterior- Right shoulder Posterior- Right shoulder, flanks the side of Abd. GB can have its own referred pain -Anterior Mid-region of Abd. along Costal Region |
|
|
Spleen Location and Classification |
Foregut LUQ Deep to Ribs 9-11 Intraperitoneal |
|
|
Spleen Functions |
Filters Blood Recycles old RBCs Stores Platelets and WBCs Fights bacterias (Meningitis, pneumonia) |
|
|
Spleen Appearance |
usually shape and size of adult fist (4in.) Purple Can't usually palpate unless enlarged Splenomegaly-Due to disease, palpable inferior to L costal margin |
|
|
Midgut Derivatives |
Distal Duodenum, Jejunum, Ileum, Cecum, Appendix, Ascending Colon, Proximal 2/3 of Transverse Colon |
|
|
Midgut Blood Supply |
Superior Mesenteric Artery (SMA) |
|
|
Midgut Venous Return |
Superior Mesenteric Vein (SMV) |
|
|
Midgut Lymphatic Drainage |
Superior Mesenteric Nodes clustered around the Superior Mesenteric Root from Abd. Aorta |
|
|
Distal Duodenum Location and Classification |
Horizontal (3rd) -Superior Mesenteric Vessels emerge just superiorly, pass anteriorly -Secondary Retro Ascending (4th) -Forms acute angle called Duodenal-Jejunal Flexure (Transition point) -Secondary Retro. |
|
|
Small Intestine Parts |
Made of duodenum, jejunum, and ileum |
|
|
Jejunum and Ileum Location and Classification |
All Quadrants, Central Abd. Intraperitoneal- robust mesenteries |
|
|
Jejunum Internal Structure |
Prominent Circular Folds- Plicae Circulares -Cause spotty barium swallow |
|
|
Ileum Internal Structure |
Sparse Plicae Circulares, disappear moving down -smooth barium swallow Reyes's Patches- Lymphoid Nodules |
|
|
Referred Pain of Small Intestines |
Anterior Only Midline, epigastric region (in all 4 quads) |
|
|
Large Intestine of Midgut |
2/3 proximal transverse colon (right side) Amending Colon, Cecum, Appendix |
|
|
Hindgut Derivatives |
Distal 1/3 Transverse Colon, Descending Colon, Sigmoid Colon, Rectum |
|
|
Hindgut Blood Supply |
Inferior Mesenteric Artery (IMA) |
|
|
Hindgut Venous Return |
Inferior Mesenteric Vein (IMV) |
|
|
Hindgut Lymphatic Drainage |
Inferior Mesenteric Nodes (@IMA root of Abd. Aorta) Lumbar Nodes |
|
|
Iliocecum Junction |
Where the Ileum terminates and merges with the medial Cecum |
|
|
Cecum Location and Classification |
Beginning of Large intestine Right side Intraperitoneal |
|
|
Appendix Location and Classification |
Attached to Cecum Intraperitoneal- attached to mesoappendix |
|
|
Ascending Colon Location and Classification |
Extends Superiorly up the right side to the right Colic Flexure or Hepatic Flexure In most - Secondary Retroperitoneal- anchored to the post. abd. wall in 25%- has mesentery and thus Intraperitoneal |
|
|
Transverse Colon Location and Classification |
Horizontal b/w hepatic and splenic flexures Intraperitoneal- transverse mesocolon |
|
|
Descending Colon Location and Classification |
Descends Inferiorly on the left side from Splenic Flexure to Sigmoid colon Secondary Retroperitoneal 33% have mesentery- Intraperitoneal |
|
|
Sigmoid Colon |
Inferior Left side Intraperitoneal- sigmoid mesocolon |
|
|
Rectum Location and Classification |
Inferior Medial of Sigmoid Colon Primary Retroperitoneal |
|
|
Referred Pain of Large Intestine |
Along midline, slightly lower than Small intestine |
|
|
Appendicitis Location |
McBurney's Point- Root of App. 1/3 of the way b/w Ant. Sup. Iliac Spine and Umbilicus Location can vary because its Intraperitoneal |
|
|
Referred Pain of Appendicitis |
Starts in region of colon- inferior midline, diffused periumbilical pain at T10 Dermatome As the parietal peritoneum becomes inflamed, somatic innervation localizes pain to the App. region in RLQ near McBurney's Point |
|
|
Abdominal Aorta Location and Trunks |
Passes through aortic hiatus of diaphragm at T12, runs down to L4 (Transumbilical Plane) where it splits into Common Iliac Arteries Paired- supply retroperitoneal organs Unpaired- Supply Abdominal Organs -Celiac, SMA, IMA |
|
|
Celiac Trunk of Abd. Aorta |
T12 lvl Foregut derivatives Splits into Left Gastric, Splenic, Common Hepatic Arteries |
|
|
Superior Mesenteric Artery |
L1 lvl Midgut Derivatives splits into -Jejunal and Ileal Arteries (Anastomosing Pattern) -Middle Colic Art. (Right Transverse Colon -Right Colic Art. (Ascending Colon) -Ileocolic Art. (Ascending colon, cecum, appendicular artery) |
|
|
Marginal Artery |
Formed by the middle and right colic arteries, and ileocolic artery Connects SMA to IMA |
|
|
Inferior Mesenteric Artery |
L3 lvl Hindgut derivatives Splits into: -Left Colic Artery (Splenic Flexure, Sup. Desc. Colon) -Sigmoid Artery (2 to 4 of them, Desc. Colon and Sigmoid) -Rectal Artery (Superior Rectum) |
|
|
Inferior Vena Cava |
Forms from L & R Common Iliac Veins @L5 Passes through Caval opening in Diaphragm @T8 Returns blood from Retroperitoneal Space and from unpaired Arteries of the adb. |
|
|
Portal System Overview |
Venous drainage of Fore &Midgut derivatives Drained to the liver for detox Processed blood enters Inf. VC via hepatic veins Anastomosis occurs due to blockage leading to Liver- causes Distension of veins |
|
|
Distal Esophagus Anastomosis |
Azygos veins (Caval) interact with Esophageal tributaries of the Left Gastric Vein (Portal) Can cause Esophageal varices (deadly) |
|
|
Rectum & Anus Anastomosis |
Superior Rectal Vein (Portal) interact with Middle and inferior Rectal Veins (Caval) |
|
|
Umbilicus Anastomosis |
Paraumbilical Veins (Portal) interact with Superficial veins of the Ant. Abd. Wall (Caval) |
|
|
Colon Anastomosis |
Arteries of the Posterior Abd. Wall (Caval) interact with Colonic Veins (Portal) |
|
|
Foregut and Midgut Parasympathetics |
Stimulate Peristalsis and Excretion -Pregang Cell Bodies- In brain -Pregang Fibers- Vagus Nerves -Postgang Cell Bodies & Fibers- In organ walls |
|
|
Foregut Sympathetics |
Inhibits peristalsis and constricts blood vessels -Pregang Cell Bodies- Lat. Horn of spinal cord -Pregang Fibers- Ventral root, to spinal nerve, to white ramus, to sympathetic trunk. -@Sym. Trunk, they turn into Greater Thoracic Splanchnic Nerves that branch from T5-T9 -Postgang Cell Bodies-Celiac Ganglion -Postgang Fibers- Follow arterial branches to organs |
|
|
Midgut Sympathetics |
Inhibit Peristalsis and Constricts blood vessels -Pregang Cell Bodies-Lat. Horn of spinal cord -Pregang Fibers-Ventral root, to spinal nerve, to white ramus, to sympathetic trunk. -@Sym. Trunk, they turn into Greater Thoracic Splanchnic Nerves that branch from T5-T9 -Postgang Cell Bodies- Celiac or Sup. Mesenteric Ganglion -Postgang Fibers- Follow arterial branches to organs |
|
|
Hindgut Parasympathetics |
-Pregang Cell Bodies- Intermediate Gray matter of S2-S4 spinal lvls -Pregang Fibers- Out ventral root, to ventral ramus, to Pelvic Splanchnic Nerves -Postgang Cell Bodies and Fibers- Walls of organs |
|
|
Hindgut Sympathetics |
-Pregang Cell Bodies- Lateral Horn of Lumbar spinal cord -Pregang Fibers- Ventral root, to spinal nerve, to white ramus, to sympathetic trunk, to Lumbar Splanchnic Nerves -Postgang Cell Bodies- Inferior Mesenteric Ganglion -Postgang Fibers- Follow arterial branches to organs |
|
|
Foregut Referred Pain |
Follow Sympathetic pathways back to spinal cord -Organ, to Celiac Ganglion, to Grey Ramus, to Spinal Nerve, to Dorsal Root Ganglion, to Dorsal Root, to Lateral Horn |
|
|
Hindgut Referred Pain |
Can follow Sympathetic or Parasympathetic pathways back to spinal cord |