Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
98 Cards in this Set
- Front
- Back
|
Here is the overview of development
|
learn it, live it, love it
|
|
Here is the overview of development
|

learn it, live it, love it
|
|
|
Congenital absence of the vagina. It is caused by RKH aka Rokitansky-Kuster Hauser syndrome
|

What is this is?
What disease caused this? |
|
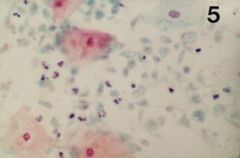
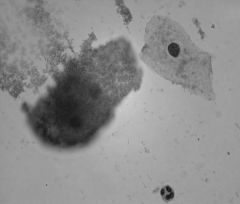
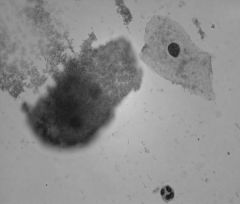
What is this patient infected with?
|
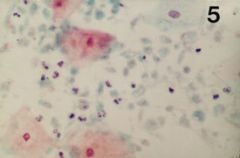
Trichomonas
|
|
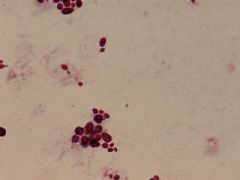
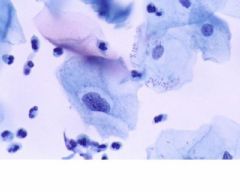
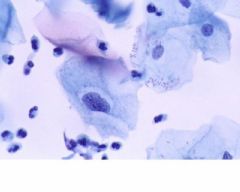
What organism is this patient infected with
|
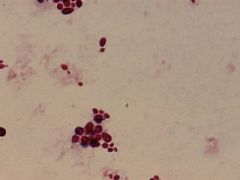
She is infected with Candida
|
|
You lowered her sheet to get a clue. You went on her, up her, and down her for a tagallant, royal time.
What kind of cells are these? |
Clue Cells
That was the mnemonic for rail of the fore mast & main mast on USCGC Barque Eagle |
|
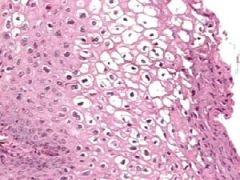
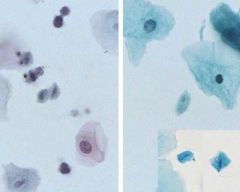
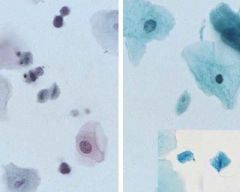
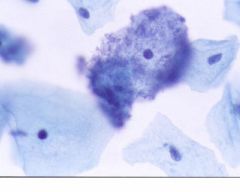
What does this pap smear indicate?
|
HPV condyloma
|
|
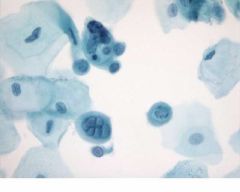
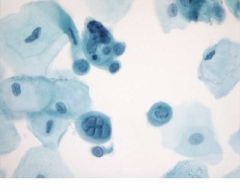
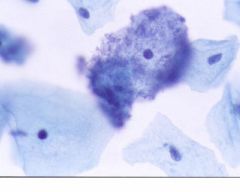
What is this?
|
HPV Condyloma
|
|
|
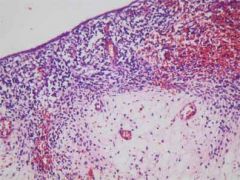
Toxic Shock syndrome
|
What disease is this slide associated with
|
|
What disease is this slide associated with?
|
Atrophic vaginitis
|
|
What is this?
|
EID
|
|
|
Endometriosis
|
What is this?
|
|
What is this?
|
Endometriosis
|
|
What is this?
|
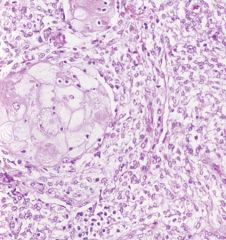
Benign mixed tumor of the vagina.
|
|
|
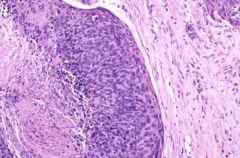
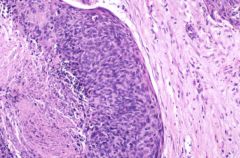
ERMS
|

What is this? (besides nasty looking)
|
|
What is this?
|
ERMS
|
|
|
ERMS
Thank you Dr. Netter |
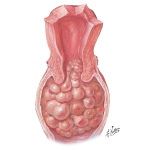
What is this?
Who made this image. |
|
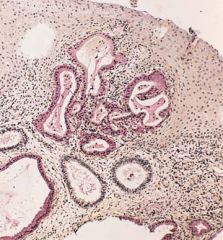
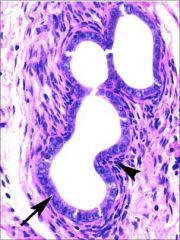
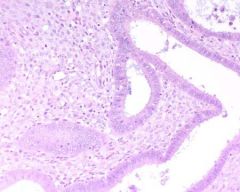
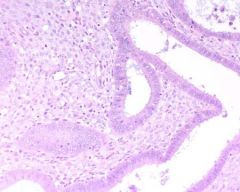
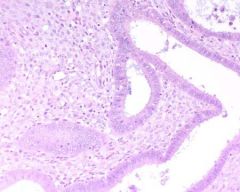
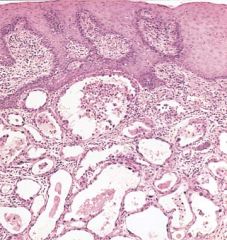
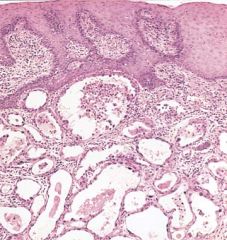
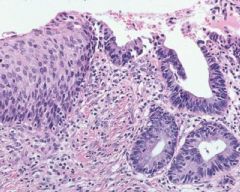
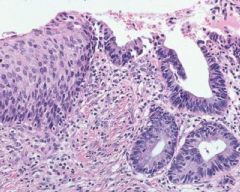
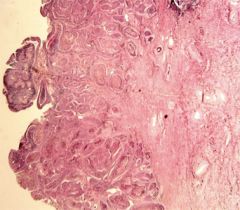
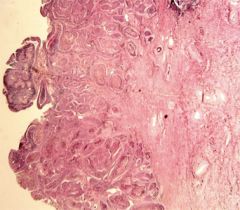
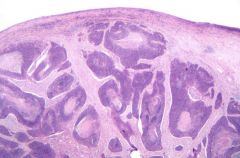
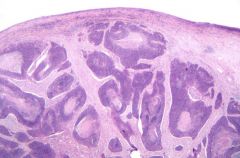
What is this?
|
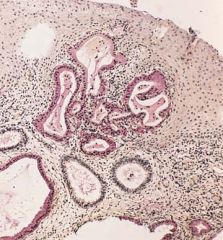
Vaginal adenosis. Mucosa of the exocervix and adjacent vagina contains
mucinous glands in place of normal squamous epithelium. Mucus is PAS-positive (red). |
|
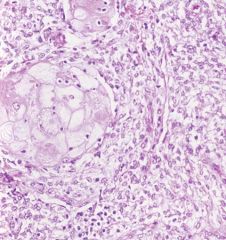
What does this patient have?
|
Clear cell
adenocarcinoma |
|
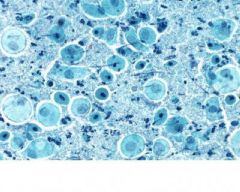
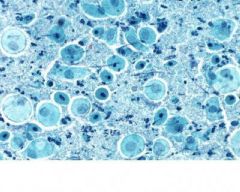
What is this?
|
Trichomonas vaginalis
|
|
What is this?
|
HSV
Herpes Simplex Virus |
|
What does this shift of flora suggest?
|
Bacterial vaginosis
|
|
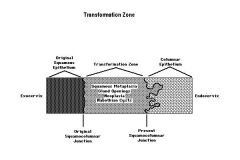
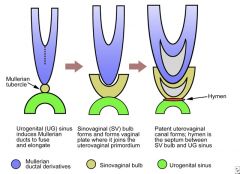
This cartoon should help explain the transformation zone
|
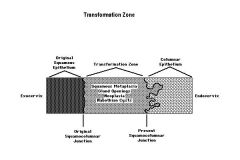
It is clear like mud right?
|
|
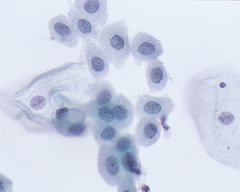
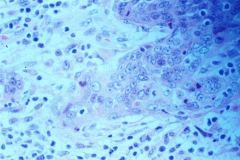
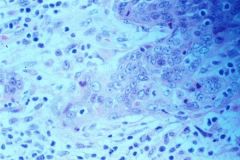
What is this image?
|
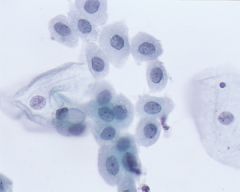
Squamous metaplasia
|
|
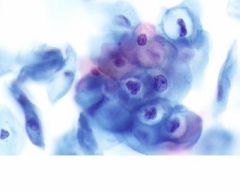
What is this image?
|
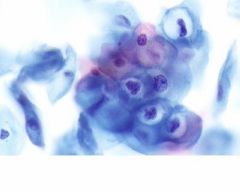
LGSIL or Condyloma
|
|
What is this image?
|
ASCUS
|
|
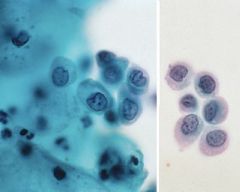
What are these cells?
|
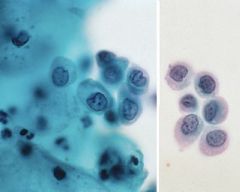
HGSIL
|
|
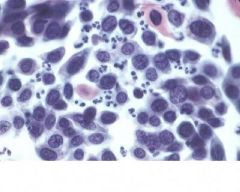
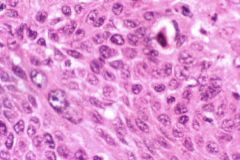
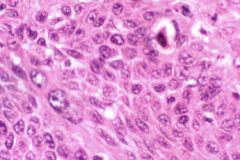
What are these cells?
|
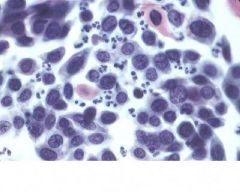
SCC Nonkeratizing
|
|
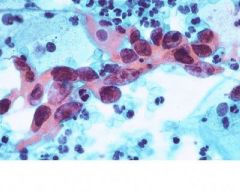
What are these cells (red) ?
|
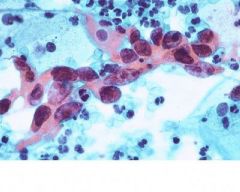
SCC Keratinizing
|
|
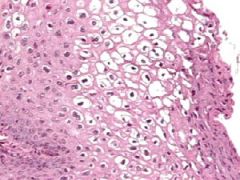
What is this image?
|
Endocervical adenocarcinoma in situ (AIS) /HSIL
|
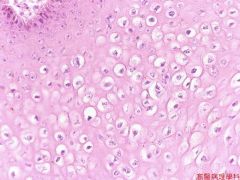
|
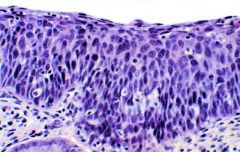
What is this image?
|
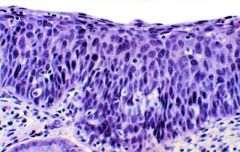
Carcinoma in situ (CIS or CIN III)
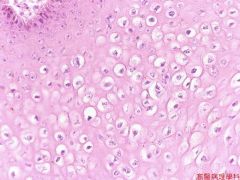
|
|
What is this image?
|
Microinvasive carcinoma (Stage la)
|
|
What is this image?
|
Keratinzing squamous
cell carcinoma of cervix |
|

What is this image?
|

Keratinzing squamous
cell carcinoma of cervix |
|
What is this image?
|
Squamous Cell Carcinoma of the cervix (SCC)
|
|
What is this image?
|
Squamous Cell Carcinoma of Cervix (SCC)
|
|
What is this image?
|
Squamous Cell Carcinoma of the cervix (SCC)
|
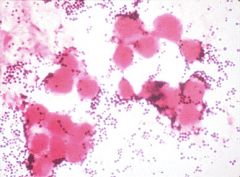
|
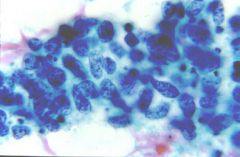
What is this image
|
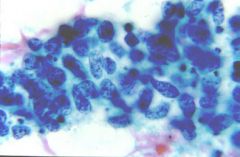
Cervix smear: small cell ca
|
|
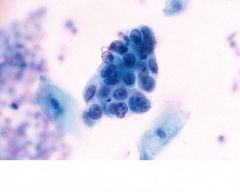
What is this image?
|

Adenocarcinoma
|
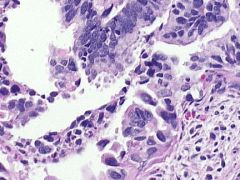
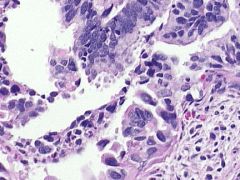
|

What is this image
|

Pap smear squamous cell carcinoma
|
|
This is a test
|
Do you know do you know do you know...
|
|
|
Name vaginal anomalies
|
vaginal agenesis,
obstruction, duplication, and fusion |
|
|
What are the features of urogenital sinus anomalies?
|
urinary and genital tracts open into
a common channel. |
|
|
What is the feature of cloacal anomalies?
|
urinary, genital, and anorectal tracts open into a common
channel. |
|
|
How often do imperforate hymens occur?
|
1 in 1000 births
|
|
|
When can imperforate hymen, atresia of the vagina or transverse vaginal septum present?
|
In the newborn or at puberty
|
|
|
What is duplication due to?
|
Incomplete fusion of Mullerian tracts.
|
|
|
How does one diagnose congenital anomalies?
|
Physical examination,
ultrasonography, & retrograde contrast studies. |
|
|
Do duplication & fusions anomalies require treatment?
|
They may not.
|
|
|
What is the second most common cause of primary amenorrhea?
|
Rokitansky-Kuster-Hauser syndrome (RKH)
|
|
|
What is Rokitansky-Kuster-Hauser (RKH)?
|
Absence of the upper vagina & uterus. The mullerian duct system stops developing at gestational days 44-48.
|
|
|
What is chromosomal analysis to exclude?
|
It is essential to exclude karyotypic abnormalites of the X chromosome (e.g. Turner syndrome, the most common cause of primary amenorrhea).
|
|
|
What are the acquired vaginal disorders?
|
Infections/inflammations
Cysts Endometriosis Neoplasms In Utero DES Exposure Pelvic Relaxation |
|
|
What are common infections and/or disorders inflammation of the vagina?
|
Trichomonas vaginalis
Candida albicans Garnerella vaginalis Condyloma acuminatum (HPV) Toxic Shock Syndrome (Staph Aureus) Atrophic vaginitis |
|
|
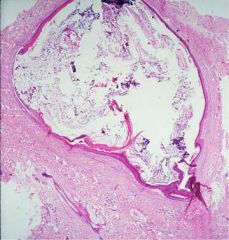
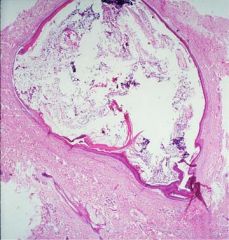
What are the most common type of vaginal cysts?
|
Vaginal inclusion cysts are the most common. These can form as a result of trauma or following an obgyn procedure.
|
|
|
What is relatively common type of cyst?
|
Gartner's duct cysts.
A portion of the Wolffian duct remains in the lateral vaginal wall. This duct is active during fetal development but ordinarily disappears after birth in the female of the homo sapiens species. |
|
|
Where has endometriosis been found (commonly)?
|
Endometriosis is commonly found in episiotomy sites.
|
|
|
How long has there been a controversy over the origin of endometriosis? (and this is relevant clinically how?)
|
There has been a 100-year controversy over the origin of this lesion; developmental or acquired.
|
|
|
What has been observed regarding traumatically removed endometrium?
|
It appears that traumatically removed endometrium can implant in scars.
|
|
|
When can menstrual endometrium implant in the peritoneum?
|
Retrograde expulsion
|
|
|
Does endometriosis respond to the cycle? How do they respond to it?
|
Yes, it responds to the cycle & but not like a 12 yo girl to 90s boy band in sync, it is often out of phase with the endometrial cavity.
|
|
|
How will an endometriosis lesion respond to pregnancy or hormonal manipulations?
|
The lesion will involute.
|
|
|
Why is the risk of Toxic Shock syndrome greater in young people?
|
Older people are more likely to have the necesary antibodies to the toxin that causes TSS.
|
|
|
What are more than half the reported cases of TSS associated with?
|
Women using tampons.
|
|
|
What do the other half result from?
|
Localized infections following burns, boils, insect bites, or surgeries.
|
|
|
What is significant about a benign mixed tumor of the vagina?
|
It is a rare tumor that may be confused with sarcoma.
|
|
|
What is the median age of occurance of benign mixed tumor?
|
young women (median age 30 yrs)
|
|
|
Where does the benign mixed tumor typically occur?
|
In or just above the hymenal ring.
|
|
|
Histologically what size & composition of the benign mixed tumor?
|
Small (1 to 5 cm in diameter)
Composed of bland spindle-shaped stromal elements admixed with epithelial origin. |
|
|
What is the origin of spindle-shaped cells & epithelial cells?
|
Epithelial origin (so says Zaman)
|
|
|
What is the most common type of malignant tumors in the vulva disorders.
|
Squamous cell carcinoma from cervix with local extenstion. Other sites include vulva, bladder, & rectum.
|
|
|
What are the risk factors for squamous cell carcinoma?
|
- HPV type 16
- Smoking cigarettes -Immunodeficiency |
|
|
Where do squamous cell carcinoma first metastasize to?
|
Inguinal nodes.
|
|
|
What is sarcoma botryoides (embryonal rhabdomyosarcoma)?
|
It is a tumor of children, usually younger than 6-years-old, it gets its name from the grape-like clusters it froms.
|
|
|
What is synonym of squamous cell?
|
epidermoid (Zaman might use the term)
|
|
|
What else is sarcoma botryoides?
|
submucous rhabdomyosarcoma.
|
|
|
Can a similar tumor to sarcoma botryoides be found in the oral cavity?
|
Yes.
|
|
|
Adenosis (benign & common)
Adenocarcinoma (clear cell adenocarcinoma) - fortanately rare. What is implicated |
Diethylstilbestrol (DES) exposure.
|
|
|
When were diethylstilbestrol (DES) and related drugs (dienestrol & hexestirenol) given ?
|
To prevent threatened abortions or women with histories of obstetrical difficulties in the mid 1940s.
|
|
|
How many women were exposed to diethylstilbestrol (DES) and related drugs (dienestrol & hexestirenol) ?
|
It is estimated that over 2 million women were exposed to these drugs.
|
|
|
How much of the exposure can be verified?
|
Only about 50%.
|
|
|
What happened in the early 1970s?
|
Vaginal & cervical abnormalities including the rather rare vaginal clear cell adenocarcinoma. This was more frequent in the offspring of mothers who had taken DES during pregnancy.
|
|
|
When is the critical interval of intrauterine DES exposure?
|
The first eighteen weeks of pregnancy.
|
|
|
What does DES inhibit?
|
DES inhibits mullerian differentiation of the tubes, uterus, & cervix
|
|
|
What are the most common changes of in utero DES exposure?
|
vaginal adenosis, cervical &/or vaginal ridges such as vaginal nood, pseudopolypoid/incompetent cervix, and cervical erosion.
|
|
|
What frequency of the common changes due to in utero DES exposure has reported to occur?
|
40 - 90 % of exposed women
|
|
|
Have upper genital tract changes been documented?
|
Yes upper genital tract changes (uterus) have been documented by hysterosalpingograms)
|
|
|
Menstrual _________ are more common in DES exposed women.
|
irregularites
|
|
|
What is the most ominous & least common change in DES exposed women?
|
The development of clear cell carcinoma.
|
|
|
What is the most common changes of DES exposure called?
|
Adenosis
|
|
|
What is adenosis defined as?
|
It is defined as the presence of columnar mucin-secreting epithelium in the vagina. It is often contiguous with glands lying in the lamina propria of the vagina.
|
|
|
With advancing age is metaplasia involved with the involution of vaginal adenosis?
|
Yes.
|
|
|
Have DES-changes in males been discovered?
|
Yes, DES-related changes are now being discovered.
|
|
|
What are the DES-changes?
|
Epididymal cyst, hypotrophic testes, examples of microphallus, sperm abnormalities are more common in DES-exposed males than in controls.
|
|
|
What is pelvic relaxation associated with?
|
A Number of conditions associated with traumatic childbirth, poor obstectrical care, & large number of births.
|
|
|
What are the results of pelvic relaxation?
|
Weakening of pelvic musculature & prolapse of various structures.
|
|
|
What are the structures that prolapse as a result of pelvic relaxation.
|
Uterine prolapse
cystocele urethacele enterocele, & rectocele |
|
|
How do pelvic relaxation conditions present?
|
Urinary incontinence. Detected on pelvic exam during a valsava manuever.
|