Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
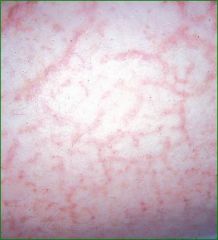
Eczema
|
pruritic inflammation of the epidermis and dermis, 2mos-2years on cheeks and extensor surfaces, eyelids and flexor surfaces for 2 and up, erythema, papules, scaling, excoriations, crusting, lichenification, keratosis pilaris, ichthyosis vulgaris, Dennie-Morgan sign, pityriasis alba
|
|
|
Keratosis pilaris
|

follicular keratosis, chicken skin, red bumps on the dorsum of the skin and the back, this is a type of eczema
|
|
|
Ichthyosis vulgaris
|

dry, scaly skin, can treat with lotion containing alpha-hydoroxy acids
|
|
|
Dennie-Morgan sign
|
extra fold or line under the eyes due to edema from atopic dermatitis(type of eczema), steroid creams, corticosteroids, antibiotics if caused by bacterial infections, sedating antihistamines to help with itching and sleep at night
|
|
|
Pityriasis alba
|
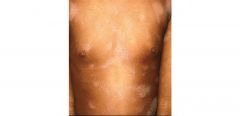
hypopigmented patches of skin secondary to inflammation due to atopic dermatitis, treat the rash and repigmentation will occur
|
|
|
Dyhidrotic eczema
|

occurs on the hands and feet with noted peeling and small tapioca pudding blisters on the palms or lateral borders of the fingers (referred to as pomphylox), Usually an associated hyperhidrosis or excess sweating, Treat with class I or II steroid and a drying agent such as 20% aluminum chloride, erythema and scale of dyshidrosis, erythema and pustules, both hands are affected which is typical in eczema
|
|
|
nummular eczema
|

coin shaped lesions usually on the dorsum of the hands and arms,seen in older patients it is often secondary to an underlying tinea infection referred to as a dermatophytid reaction, treating the underlying fungal infection(clotrimazole) will help clear the nummular eczema but quicker resolution will occur with the use of a topical steroid on the eczematoid lesions
|
|
|
asteatotic eczema
|
eczema craquele,appearance of cracked porcelain, seen in older patients,essentially excessively dry skin, treated with keratolytic agents such as 12% lactic acid, 10% or 20% urea cream or glycolic acids, emollient use, the greasier the better, H1 antihistamines help patients fall asleep but generally do not stop the itching
|
|
|
lichen simplex chronicus (still eczema)
|

secondary to rubbing or scratching, skin thickens in response to the insult, commonly seen in areas where patients have easy access(medial ankles and forearms), treated with potent topical steroids under occlusion and keratolytic agents, avoiding scratching or rubbing by use of distraction methods or cooling emollients such as those with menthol, avoiding allergic triggers and scratchy clothing such as wool, frequent emollients, topical steroids – using the lowest potency to clear the lesions, tars (however they will stain clothes, towels and porcelain tubs), the keratolytic agents such as the alpha-hydroxy acids, the immunomodulators such as tacrolimus and pimecrolimus and in extensive cases phototherapy
|
|
|
contact dermatitis
|
Caused by external agents, toxicity, or allergic reaction; pruiritis or burning of skin, irregular well demarcated patches of erythema and edema, non-umbilicated vescicles, punctuate erosions exuding serum and crusts, often linear arrangement, clinical findings and patch test, remove agent causing reaction, topical or systemic corticosteroids
|
|
|
Seborrheic dermatitis
|
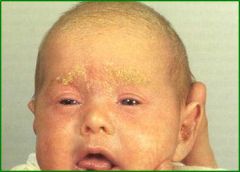
“cradle cap” in infants and dandruff in adults, Infants usually grow out of the rash by 9 months, the scalp, eyebrows, eyelashes, beard and mustache area, behind the ears the v of the chest and the groins, can also go to the forehead and in the ears, treatment for infants is to use mineral oil and a soft baby brush instead of seborrhea shampoos because of the risk of contact dermatitis, Salicylic acid, selenium sulfide, zinc pyrithrone, tar preparations, ketoconazole, topical steroids, sodium sulfacetamide with sulfur, cicloprox
|
|
|
psoriasis
|
sharply marginated papules and plaques, hereditary disorder, presents in the 20's and 50's, +auspitz sign(white scale when scraped off causes bleeding), elbows, knees, sacral area, nails, biopsy, "pepperoni" appearance, Topical steroids, Emollients, Tars, Dovonex, Phototherapy (UVB, PUVA), Anthralin, topical retinoids Methotrexate, Acitretin, Cyclosporine, Biologics
|
|
|
Pityriasis Rosea
|

maculopapular, red, scaling, eruption, herald patch(bigger than the others and erupts first), fine scaling, oval maculates w/marginal collaterette, "christmas tree" pattern, mimics syphillis so run RPR, palliative care with topical steroids and antihistamines
|
|
|
Lichen planus
|

acute or chronic inflammation of the skin and mucous membranes, pruiritic, purple, papules, planar, polygonal, wrist, lumbar area, shins, scalp, eyelids, groin, nails, 40% papules w/white reticulate lesions on the buccal mucosa, usually resolves on its own, Topical corticosteroids with occlusion (not on lids), tacrolimus, pimecrolimus, PUVA, Oral corticosteroids, Cyclosporine A in resistant cases
|
|
|
Rosacea
|
stage 1-intermittent flushing w/few talangiectasis
stage 2-persitent flushing, telangiectasis, papules, pustules, abscence of comedones stage 3-persistent erythema, numerous talangiectasis, papules, pustules, nodules, rhinophyma formation stop using the things that trigger flushing, sunscreen daily, metronidazole 0.75%, clindamycin 1%, erythromycin 2%, azelic acid cream 20%, tetracyclines, accutane 0.5-1mg/kg/day rhinophyma-dermabrasion, telangiectasias-electrocautery |
|
|
Folliculitis
|

follicular-based pustule, frequently grouped
face/legs-staph aureus due to shaving, mupriocin, dicloxicillin, macrolide antibiotics trunk-psuedomonas aeruginosa(hot tub), quinolones back-candida albicans in febrile hospitalized pts |
|
|
Perioral dermatitis
|

females age 16-45, erythematous, micropapular, fine scaling eruption, nasolabial folds, chin and upper lip, etiology unknown(maybe toothpaste?)
tetracycline/erythromycin |
|
|
Hidradenitis suppurative
|

chronic inflammatory scarring disease related to apocrine sweat glands, axilla, inguinal, perianal and inframammary areas, intralesional triamcinolone 5-10mg/ml, I&D, minocycline, ciproflaxican, cephalosporins, clindamycin, accutane 1mg/kg, surgical excision of area aprocrine glands
|
|
|
paronychia
|

red, painful area proximal/lateral to nail fold, post trauma, usually staph, I&D, penicillinase resistant antibiotics (acute)
redness, edema of nail fold of several fingers, long term dystrophy of the nail, people who work with hands in moist enviroment, class 5 steroid, miconazole, thymol, fluconazole if canididal overgrowth |
|
|
impetigo
|

transient thin roofed vesicles, then golden-yellow stuck on crusts, face, arms, legs, buttocks
mupirocin, fusidic acid, oral antibiotics w/good staph/streptococci coverage *can occasionally cause glomerulonephritis |
|
|
cellulitis
|
adults-strep and staph children- H. influenza, strep, staph
breaks in skin, ulcers, chronic dermatosis red, hot, tender,edema, sharply defined, irregular borders analgesia and oral antibiotics IV antibiotics if severe |
|
|
erysipelas
|

variant of cellulitis caused by group A streptococci, lymphatics involved, sharply demarcated from normal skin, spreads centrally, painful, face, lower legs, areas w/preexisting lymphedema, umbilical stump
analgesia and oral antibiotics IV antibiotics if severe |
|
|
diaper dermatitis
|
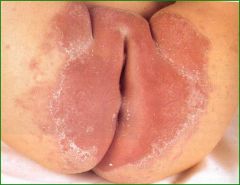
nystatin or imidazole cream bid
oral nystatin diluted Castellani's paint addition of topical steroids speed up healing |
|
|
onychomycosis
|

yellow, white hyperkeratotic ddebris, crumbly toenails, generally due to trichophyton rubrum, KOH and culture
itraconazole 200mg, 2 PO qd for one week on and 3 weeks off for 3 months terbenifine 250mg qd 3 mos ciclopirox nail lacquer as added agent surgical removal |
|
|
dermatophytes
|
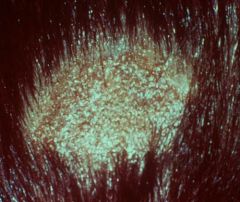
superficial infections on non-viable keratinzied tissue, caused by trichophyton, microsporum, epidermophytan, broken off hair on th scalp(black dots), kerion(exudative follicles), Wood's lamp, KOH prep, culture
terbenifine, griseofulvin, ketoconazole, itroconazole, PO or IM steroids if kerion present |
|
|
Tinea Corporis/pedis
|
sharply marginated plaque, scaling, enlarges from periphery
maceration between toes or moccasin-like scale Wood’s lamp, KOH prep, Culture Topical imidazoles, Terbenifine, Griseofulvin, Ketoconazole, Itraconazole |
|
|
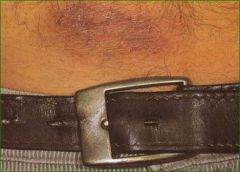
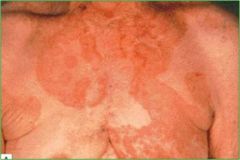
tinea versicolor
|

Malassezia furfur, sharply marginated off-white to brown “velvety” macule, fine scaling, round to oval on chest and back, occasionally pruritic, worse in hot humid weather, topical imidazoles, oral or topical ketoconazole, itraconazole, Selenium sulfide
|
|
|
Verruca Vulgaris
|

Human Papilloma Virus, school age children, decreases after 25, firm papules, hyperkeratotic, clefted surface, vegetations, site of trauma, biopsy, HPV subtyping, : Salicylic acid and/or lactic acid in collodion, curettage, surgical or laser excision, cryosurgery, electrocautery, tagamet, hyperthermia, intralesional bleomycin/interferon, Imiquimod, topical retinoids, cantharone
|
|
|
Verruca Plana
|

HPV, biopsy, HPV subtyping, mesa-like flat-topped papules, linear (self inoculation from scratching), Topical retinoids, cryosurgery, electrosurgery
|
|
|
Condyloma acuminata
|

Subtypes 6 and 11 are the most common (90% of all genital warts), however 16 & 18 are associated with 70% of cervical cancer,
Imiquimod (Aldara), 20% podophyllin, 0.5% podofilox, 5-fluorouracil, Trichloroacetic acid, Pulsed dye laser, Cryotherapy Electrocautery Gardasil, the HPV vaccine, covers subtypes 6, 11, 16, 18 |
|
|
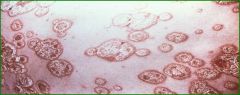
Molluscum Conatagiosum
|
caused by poxvirus
Discrete, umbilicated, dome-shaped, pearly-white, waxy papules, Adults (often STD or in HIV infected individual), Neck, trunk, anogenital area, eyelids, Children - spontaneous remission, but can use cryosurgery and curettage Adults - curettage, cryosurgery, electrocautery, Topical retinoids |
|
|
Scabies
|

intense, generalized, intractable pruritis, burrows, vesicles, nodules, excoriations, Pruritis can continue up to 2-3 weeks, Topical steroids, Antihistamines (Atarax, Benadryl), Elimite (5% Permethrin), Ivermectin, Clothes, sheets, etc. wash normally the next morning; bedspread, coats, put in plastic bag for 4-7 days
|
|
|
Pediculosis (lice)
|

Over-the-counter treatment:
topical pyrethrin with piperonyl butoxide (Rid) Prescription treatments: permethrin (5% Elimite, 1% Nix) topical sulfur lindane (Kwell) malathion (Ovide) crotamiton (Eurax) Remove nits using a special comb Sanitize clothing and bedding Examine close contacts, especially children |
|
|
Brown Recluse Bite
|

RICE, aspirin, antihistamine, tetanus prn, antibiotics, analgesics, dapsone, surgical debridement
|
|
|
black widow bite
|
Neurotoxin – muscle cramps, spasm, nausea, vomiting, hypertension, weakness, malaise, tremors, lasting days to a week
Ice, antivenin alone or in combination with IV opioids and muscle relaxants |
|
|
Bullous Pemphigoid
|

Onset >60 years of age
Pruritic skin lesions Tense blisters Oral mucous membrane lesions in 10-35% Self-limited in many cases Treatment with oral glucocorticoids alone or with azathioprine, also dapsone, tetracycline, niacinamide |
|
|
Vitiligo
|

Symmetric white macules, periorificial locations, sites of trauma, early lesions can be pink or tan
Review of systems - halo nevi, Alopecia areata H/O thyroid disease, diabetes mellitus, pernicious anemia, Addison’s disease Any age - peak 10-30 years Etiology: Autoimmune destruction of melanocytes Labs: TSH, FBS, ANA Psoralen plus UVA (PUVA), Topical corticosteroids, Minigrafting, Sunscreens, Cosmetics, Depigmenting (MBEH) |
|
|
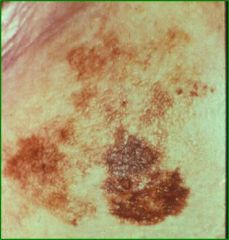
Melasma
|

Common acquired hypermelanosis
Occurs in sun-exposed areas, Worse with sun exposure, pregnancy, oral contraceptives and anti-epileptic medications Only 10% of cases reported in males Most common in the central face, may be epidermal (brown), dermal (blue-gray) or mixed (brown-gray) Treatment: sunblock (>SPF 30, Parsol 1789, Mexoryl) , bleach (2 to 4% hydroquinone, adapalene, tretinoin, +/- hydrocortisone and time (may take 2 to 6 months to see a response), also azelaic acid, chemical peels, laser Do not use MBEH because of risk of irreversible leukoderma/induction of vitiligo in distant sites Discontinue OCP’s if possible |
|
|
Acanthosis nigricans
|
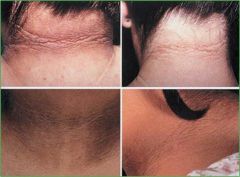
Hyperpigmentation and thickening of the skin of the neck and in body folds; appears “velvety”
Skin markings are accentuated Paraneoplastic AN can involve palms/soles and vermillion border of the lips Classification: Type 1 - hereditary, benign Type 2 - insulin resistant states Type 3 - Pseudo-AN, seen with obesity Type 4 - Drug-induced (nicotinic acid, oral contraceptives) Type 5 - Malignant - Paraneoplastic |
|
|
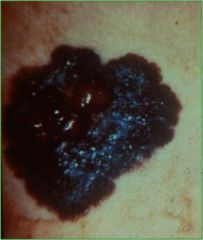
Moles
|
A - Asymmetry in shape, one half unlike the other
B - Borders are irregular with irregular, scalloped edges C - Color is mottled, with a haphazard display of colors - shades of brown, black, gray, red and white D - Diameter is usually large, greater than the tip of a pencil eraser (6.0mm) E - Enlargement (history of an increase in the size of a lesion) is perhaps one of the most important signs of malignant melanoma |
|
|
Superficial spreading melanomas
|
Account for 70% of all melanomas, 30 - 50 years, Slightly higher in females, Evolves over a period of 1 - 5 years, excisional biopsy is treatment
|
|
|
Nodular melanoma
|

Account for 16% of all melanomas, Median 50 years, Evolves over 6 - 18 months, Rarely associated with a nevus remnant, worse prognosis than superficial spreading bc of vertical growth and thickness
|
|
|
Lentigo maligna
|
Synonymous with Hutchinson’s nevus, Hutchinson’s freckle, melanoma in situ, Flat, macular, intraepidermal neoplasm and the precursor or evolving lesion of Lentigo Maligna Melanoma (LMM), median age 65, Older population with increased sun exposure
|
|
|
Lentigo maligna melanoma
|

Accounts for 5% of all melanomas,Seventh decade, predominantly occur on the head and neck, May take up to 20 years to evolve from a Lentigo Maligna
|
|
|
acral lentiginous melanoma
|

Account for 2 to 8% of all melanomas; evolves over 2.5 years, Median is 65 years, Male:Female ratio - 3:1, ALM is the principal melanoma in American and African Blacks; accounts for 50 - 70% of melanomas in Japanese population, Survival rates for the volar(on palms and soles) type are less than 50%, Subungual(under the nails) type has a 5-year survival rate of 80%
|
|
|
Acitinic Keratosis
|

Single or multiple, discrete, dry, rough, adherent, scaly lesions on habitually sun-exposed skin, Usually middle age, More common in males, skin phototypes I, II, III, Rare in IV , Almost never in V or VI, Outdoor workers, sportspersons and sun worshipers
|
|
|
Basal Cell carcinoma
|
Mole like,papule, nodules, ulcer-like, most common type of skin cancer, does not have ability to metastisize, Excision with primary closure, skin flaps or grafts, Cryosurgery, curettage and electrosurgery are options, but have higher recurrence rates, Imiquimod, For lesions in the danger zones (around eyes, in the ear canal, posterior auricular sulcus and in sclerosing BCC) Moh’s surgery is the best approach
|
|
|
Bowen's Disease
(squamous cell carcinoma in situ) |

Usually a solitary lesion on exposed skin, Slowly enlarging, erythematous macule, sharp border, little or no infiltration, usually slight scaling, some crusting, excision, Moh’s surgery in difficult sites, Cryotherapy, Efudex, Imiquimod, Mortality rate is very low
|
|
|
Invasive Squamous Cell Carcinoma
|

Fleshy, granulating, friable, crusted nodules, Has the capacity to metastasize, Any persistent nodule, plaque or ulcer, especially in areas of sun-exposure, radiation dermatitis, old burn scars or on the genitalia must be biopsied, Excision, SCC has an overall remission rate after therapy of 90%
|
|
|
Seborrheic Keratosis
|

skin colored to brown to black, discrete, raised, rough or hyperkeratotic, papules to plaques, often verrucous,
greasy “stuck on” appearance, sebaceous areas: face, back, chest, groin, Completely benign, Common, middle age-elderly, higher in whites, hereditary, liquid N2,"", curettage, treatment not necessary,R/O malignant melanoma in dark lesions |
|
|
Dermatosis Papulosis Nigra
|

2-3mm, brown to black, hyperkeratotic, pedunculated or verrucous papules, cheeks, around eyes bilaterally, Completely benign, teens to middle age, hereditary, more common in Blacks and Hispanics, Origin
equivalent to seborrheic keratosis, Liquid nitrogen – do test patch for hypopigmentation, small lesion electrocautery and curette, large lesion-anesthetize, excise, will normally recur |
|
|
Lipoma
|

soft, pillowy, SQ lesions, normal, mobile overlying skin, 1-10+cm, trunk, extremities, Benign, fast growing, consider malignant transformation, any age, more common mid 20’s, asymptomatic, may be tender if large component of blood vessels, excision, once removed, they normally do not recur
|
|
|
Erythema Nodosum
|

Acute inflammatory/immunologic reaction caused by a number of etiologies, Painful, tender nodules on the lower legs, fever, malaise, 50% with arthralgias, F:M 3:1, Infection - Group A ß-hemolytic Strep and others, Drugs - Sulfa, OCP, Sarcoidosis, Ulcerative colitis, Behçet’s, Idiopathic in 40%, Spontaneous resolution in 6 weeks depending on etiology, Bed rest, symptomatic treatment
|
|

Erythema multiforme
|
acute, self-limited skin eruption with symmetric, pruritic or painful, acral target lesions, EM Minor, No mucosal lesions, No prodromal symptoms, Tends to be recurrent,
EM Major (SJS/TEN), At least one mucosal surface involved, Acral and facial lesions early, Trunk is frequently spared, Often see prodrome of fever, headache, myalgias, cough, Infection - HSV infections are the most common cause, preceding the EM outbreak by 10-14 days, bacterial, mycotic, viral, e.g. influenza, EBV, Mycoplasma pneumoniae, Drugs - Antibiotics - PCN, tetracycline, sulfa, Anticonvulsants - hydantoins, carbamazepine, barbiturates, Other - antihypertensives, NSAID’s, allopurinol; Stop medication, Resolution of virus, Topical or systemic steroids |
|
|
Stevens-Johnson Syndrome
|

1-6 week duration, Usually symmetric distribution, fixed
> 7 days, Severe mucosal involvement in 2 or more areas, Prodrome of fever, malaise, sore throat, headache, cough, Secondary infection, Fluid and electrolyte loss, Sloughing of upper and lower respiratory tract, Blindness due to corneal lesions, Death Attempt to identify underlying infection or drug source Specific treatment or removal of offending drug, Systemic corticosteroids *,IViG *, Support measures, Burn unit support, Fluid/electrolyte & nutrition support, Treat secondary infection specifically, Care of skin |