![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
139 Cards in this Set
- Front
- Back

circumscribed, flat (in plane of skin) discoloration under 0.5cm |
macule |
|

elevated solid lesion under 0.5 cm |
papule |
|

circumscribed, flat discoloration over 0.5cm |
patch |
|

Circumscribed, elevated,superficial solid lesion over 0.5 cm |
plaque |
|

Circumscribed, elevated, solid lesion over 0.5 cm |
nodule |
|

Circumscribed collection of leukocytes and free fluid Varies in size |
pustule |
|

A circumscribed collection of free fluid ≤ 0.5 cm |
vesicle |
|

A circumscribed collection of free fluid > 0.5 cm(Bigvesicle) |
bullae |
|

Firm, edematous plaque resultingfrom infiltration of the dermis with fluidTransient and last hours |
wheal (hive) |
|

Excess dead epidermal cellsproduced by abnormal keratinizationand shedding |
scale |
|

A collection of dried serum & keratin debris(AKA Scab) |
crust |
|
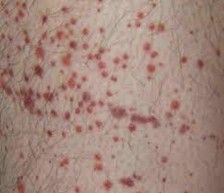
Circumscribed deposit of blood ≤ 0.5 cm |
petechiae |
|

Circumscribed depositof blood > 0.5 cm |
purpura |
|

Thickening of stratum corneum |
hyperkeratotic |
|

Dilated superficial blood vessels |
telangiectasias |
|
|
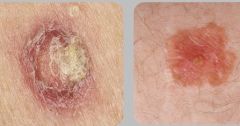
A squamous cell carcinoma (SCCA) confinedto the epidermis. Lesions are common, caused by chronic,prolonged sun exposure and increase in number with age. scaly, rough, crusty lesions |
actinic keratosis |
|
|
one treatment for actinic keratosis involves blank therapy, which uses liquid nitrogen |
cryotherapy |
|
|
topical chemotherapy agents photodynamic therapy are other treatments for blank |
actinic keratosis |
|
|
the most common form of treatment for isolated, superficial actinic keratosis legions is blank therapy |
cryotherapy (liquid nitrogen/LN2) causes separation of the epidermis and dermis causes redness, scaling, blistering for 1-2 weeks post |
|
|
actinic keratosis that is widespread (needs field treatment) is treated with blank therapy |
Photodynamic therapy (PDT) (treatment with chemical agent + blue light) |
|
|
During blank therapy, a photosensitizing agent (Levulan)applied, then exposed to a constantwavelength of light for ~15 mins |
PhotoDynamic therapy (PDT) |
|
|
does PDT scar the skin? |
no, it's nonscarring Varying degrees of discomfort, irritation and photosensitivity areexperienced for a few days post treatment |
|
|
for field therapy or for multiple lesions of actinic keratosis, blank therapy is also used (different than PDT) |
topical chemotherapy agent |
|
|
treatment of AK with topical agents can expose and eliminate blank AK lesions |
subclinical (non-visible) AK lesions |
|
|
which treatment has been shown to reduce/combat the development of new AK lesions years into the future? |
topical therapy |
|
|
5-Flurouracil (Efudex) Imiquimod (Zyclara) Picato (Ingenol) are blank types of treatment for actinic keratosis |
topical therapy All cause some degree of erythema, scaling, and crustingIntensity of reaction depends on severity of damage |
|
|
the only way to diagnose actinic keratoses is to blank |
palpate, early lesions often can only be felt not seen |
|
|
what is the difference between actinic keratosis and squamous cell carcinoma? |
Actinic Keratosis (AK) are actuallySquamous Cell Carcinomas (SCC) confined to the top layers of the epidermis. Lesionsthat extend more deeply to involve the papillary and/or reticular dermis aretermed SCC. 60% of these lesions start as AK. |
|
|
There is no way to clinicallydifferentiate between an AK and a developed SCC other than blank but….. Larger, thickened, indurated (hardened), tender, inflamed and/or oozing lesionsare probably bad |
biopsy SCCs are 65x more likely to develop in transplant patients |
|
|
years of blank are required to develop AK |
chronic UV exposure |
|

|
actinic cheilitis "farmer's lip" AK on the lip |
|

|
AK |
|
|
Begins as a pearly white or pink, dome shaped papule withtelangiectasias that frequently cause central ulceration due to friability (tendency to crumble) can bleed/have hemorrhagic crust |
basal cell carcinoma (most common form of skin cancer) |
|

|
basal cell carcinoma |
|
|
how do you confirm a diagnosis of basal cell carcinoma? |
biopsy |
|
|
what (3) factors affect treatment of basal cell carcinoma? blank type blank size location |
cell type tumor size location tx: Excision with Electrodessication & Curettage Mohs Surgery |
|
|
During blank surgery, layersof cancer-containing skin areprogressivelyremoved and examined until onlycancer-freetissue remains. |
Mohs (tx for basal cell carcinoma) |
|
|
Invasiveor large cancers Cartilaginousareas (Ears, Nose) Areaswhere underlying structures are of concern (Temple, Canthus) are indications to use which form of tx for basal cell carcinoma? |
Mohs |
|
|
what is the most common type of skin cancer and where is it found 85% of the time? |
basal cell carcinoma 85% found on head/neck |
|
|
where in the head/neck are basal cells most commonly found? |
nose (25-30%) transplant patients 10-100x greater risk BCC can occur at sites of previous skin damage |
|
|
average lifetime riisk of Caucasian developing BCC? |
30% |
|
|
what kind of UV exposure is associated with BCC? |
intermittent, intense UV exposure (3 bad sunburns increase risk by 70%) |
|
|
poor tanning ability fair skin blonde/red hair light color eyes (like blue) are risk factors for what condition? |
basal cell carcinoma |
|

|
nodular basal cell carcinoma (most common) |
|

|
superficial basal cell carcinoma |
|

|
pigmented basal cell carcinoma |
|
|
How do you differentiate between AK and SCC? |
AK is only top layer the epidermis, SCC is throughout epidermis |
|
|
a SCC limited to the epidermis is called blank |
in situ |
|
|
a SCC that has progressed from the epidermis into the dermis is said to be blank |
invasive |
|
|
when you see long term, chronic UV exposure in a hx, think blank |
squamous cell carcinoma |
|
|
nodule formation or tenderness of asuspected SCCA lesion suggests an blank component |
invasive |
|
|
anogenital (in the area of the anus/genitals) HPV lesions can involve into blank, especially in smokers |
squamous cell carcinoma immunosuppressed patients are also at increased risk of developing SCC |
|
|
an isolated patch of redness and scaling WITHOUT pruritus should always be suspected to be blank, (don't assume dermatitis) |
SCC |
|
|
squamous cell carcinoma |
|

|
SCC |
|

|
leukoplakia (premalignant SCC from tobacco use) |
|

|
leukoplakia |
|

|
Keratoacanthoma
Believedto be a variant of SCCa Originates in the pilosebaceous (hair/sebum gland) unit Excision is recommended |
|
|
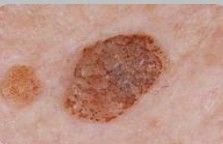
hyperpigmented, verrucous (wart-like), and hyperkeratitic (rough) stuck on lesions shows a sharply circumscribed lesion with black pearls of horn cysts onthe surface |
Seborrheic Keratosis (benign cutaneous neoplasm) not connected with viruses |
|

|
seborrheic keratosis |
|
|
do seborrheic keratoses have malignant potential? |
no most people will develop at least one in their life time |
|
|
Seborrheic keratoses are common on the extremities, face, and trunk (hair bearing areas). they are never found where (3)? |
seborrheic keratoses ARE NEVER found on lips palms soles nonhair areas |
|
|
how can you distinguish between seborrheic keratosis and melanoma? |
seborrheic keratosis has horn cysts (round intralesional cysts of loose keratin) melanoma does not, but do a biopsy if in doubt |
|
|
SKs are generally benign, but if one is inflamed in a sun-exposed area, what is a possible concern |
underlying skin cancer like SCC |
|
|
eruptivesudden increase in size and number of seborrheic keratoses that are intensely pruritic may be a sign of internal malignancy this is called the blank sign (french name) |
Leser-Trelat Sign |
|

|
SeborrheicKeratosis |
|
|
SeborrheicKeratosis |
|

|
SeborrheicKeratosis |
|

|
Stucco Keratoses Type of SK most common on the lower legsof the elderly |
|
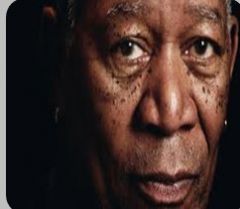
Typeof SK that develops on sun-exposed areas of African Americans |
DermatosisPapulosa Nigra |
|
|
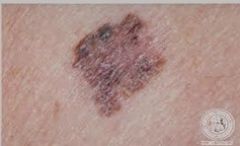
A large, hyperpigmented, asymetric macular lesionis noted to the right upper back Closer examination reveals Asymetric irregular Borders with heterogenous Colorvariations and Diameter of ~6mm. |

malignant melanoma (Asymmetry, borders, color variations, diameter) |
|
|
Clarks Level and Breslow Depth are tests used to blank melanoma?> |
stage melanoma |
|
|
Melanoma is treated by excising the lesion with blank margins? |
5 mm margins (wide and deep excision) close follow up: Generalexams including evaluation for lymphadenopathy andorganomegaly Q3months x 2 years and Q6 months x 3 years |
|
|
non-melanoma skin cancer dysplastic nevus 1st degree relative with melanoma are risk factors for blank |
malignant melanoma |
|
|
>50 nevi on the body or >11 nevi on one arm is a risk factor for |
malignant melanoma |
|
|
chronic tanning repeated blistering sun burns immunosuppression Fair skin, red/blond hair, freckling, inability to tan are risk factors for |
malignant melanoma |
|
|
which gender is more likely to get malignant melanoma |
males (median age of diagnosis is 57) |
|
|
Which race is mostly likely to get malignant melanoma? |
caucasians 10fold greater risk |
|
|
what area is most common for women to develop melanoma? |
legs |
|
|
what area is most common for men to develop melanoma? |
trunk |
|
Flat,non-palpable Haphazardcombination of colors which type of melanoma? |
superficial spreading melanoma (SSM) |
|

¤Dome-shapedor pedunculated ¤Darkred brown-black which type of melanoma? |
nodular melanoma (NM) |
|

¤MC onface in 6-7th decade ¤Colormore uniform than SSM which type of melanoma? |
lentigo maligna (LM) |
|

¤Palms,soles, terminal phalanges and mucous membranes ¤MC inAA and Asians ¤Elevatedlesions are associated with deeper invasion |
acral-lentiginous (ALM) acral (peripheral body parts) |
|
|
the blank level describes the level of anatomical invasion of a cancer |
clark's level Level I:confined to the epidermis (in situ) Level II:invasion of the papillary (upper) dermis Level III:filling of the papillary dermis, but no extension in to the reticular (lower)dermis Level IV:invasion of the reticular dermis Level V:invasion of the deep, subcutaneous tissue |
|
|
the total vertical height of an melanoma is described by the blank depth |
Breslow depth |
|
|
unusual,benign moles which resemble melanoma and indicate an increased risk of melanoma |
dysplastic nevi (DN) a percentage of dysplastic nevi will growmelanoma.Complete removal of dysplastic nevus eliminates this risk inthat mole only. DNsare graded: ¤Mild¤Moderate¤SevereSevere DNs show a level of dysplasia that is bordering evolution into MM |
|
|
hair loss clumps falling out over 1-2 months mild itching/burning annular loss smooth white skin no redness/scaling "exclamation hairs" around periphery |
alopecia areata |
|
|
Common, asymptomatic disease characterized by rapid onset of total hairloss in a sharp, usually round, area. |
alopecia areata any hair bearing surface can be affected cause is unknown, suspected to autoimmune |
|
|
Is there a treatment for alopecia areata? |
TREATMENT ONLY CONTROLS, DOES NOTCURE Mostoften, reassurance and observation areall that is necessary. Few,localized areas of hair loss have an excellent prognosis for re-growthWhen the above fails:intralesional corticosteroids are considered 1st line therapy |
|
|
What endocrine gland should you check if someone has alopecia areata? |
thyroid (8-12% of AA patients have thyroid issues) |
|
|
AA is not common, but can run in families. When does hair regrowth occur if it is going to? |
1-3 months ( Newhair is usually the same color and texture but may grow back white ) |
|
|
total hair loss of the scalp is alopecia blank |
alopecia totalis |
|
|
total hair loss of the body is alopecia blank |
alopecia universalis |
|
|
a hair loss condition due to androgens in genetically predisposed men and women |
androgenic alopecia |
|
|
androgens cause progressive shortening of successive blank cycles |
anagen cycles |
|
|
what is the anagen phase of hair growth |
active growth phase |
|
|
what is the catagen phase of hair growth? |
signals end of hair growth (stop) |
|
|
what is the telogen phase of hair growth? |
resting phase (rest) |
|
|
where are androgen-sensitive hair follicles located? |
top of the scalp (sides and back of scalp are not androgen sensitive) |
|
|
Testosterone + 5α-reductase TypeII =Dihydrotestosterone Dihydrotestosterone acts on theandrogen-sensitive hair follicles, making them smaller and causingfaster/shorter anagen phases |
Testosterone + 5α-reductase Type II = Dihydrotestosterone Dihydrotestosterone acts on the androgen-sensitive hair follicles, making them smaller and causing faster/shorter anagen phases |
|
|
originally developed to treathypertension Directvasodilator, that in turn, may increase duration of anagen phase which medication for androgenic alopecia? |
minoxidil (Rogaine) |
|
|
finasteride (propecia) is a treatment for androgenic alopecia, because it blocks blank? |
Blocks5α-reductase Type II Results in 3 months ~20-30% of men do not respond Child-bearing women CANNOT TAKE OR TOUCH¤Canimpair virilization ofmale fetus |
|
|
Adistinct pattern of central scalp alopecia that is caused by increased levels of serum adrenal androgen dehydroepiandosterone sulfate (DHEA-S) is seen in which gender? |
females adrenal androgenic female pattern alopecia (treated with minoxidil/rogaine) |
|
|
alopecia second to physical traction (heavy braids) is called blank |
traction alopecia treatment is to stop wearing your hair that way |
|
|
Diseaseof the pilosebaceous unit ↑ sebum production ↑ P. acnes proliferation abnormal desquamation ofepithelial cells plugging with debris |
acne vulgaris increased sebum production is cardinal feature for acne |
|
|
earliest type of acne, develops during early teen years due to build up of sebum and keratin |
comedonal acne "Non-inflammatory type" |
|
|
closed comedone is a blank head open comedone is a blank head |
closed comedone is a white head open comedone is a black head (keratin is oxidized) |
|

|
comedonal acne |
|
|
Inflammatory response to keratin plugging and P. acnes infection which type of acne? |
papulopustular acne "inflammatory type" |
|

|
papulopustular acne "inflammatory type" |
|

Severe inflammatory response to P. acnes infection |
NodulocycticAcne“ScarringType” Oftenexcessive sebum production Treatmentrequires Isotretinoin therapy |
|

|
acne keloidalis (tx with isoretinoin followed by excision of keloid) |
|
|
Benignenlargement ofthe sebaceous glandsWhite-yellowor skin colored papules withcentral umbilication |
sebaceous hyperplasia |
|

|
sebaceous hyperplasia |
|
|
What is the line of tx for acne? |
topicals
Tretinoin 0.025 – 0.1% QHS Verydrying, may need to ↓ dose or use QOD Clindamycin 0.1% lotion AND BenzoylPeroxide (OTC) |
|
|
If topicals fail, blank can be added? |
oral antibiotics if these both fail, refer to dermatology |
|
|
Severe recalcitrant cystic,nodular, or inflammatory acne Scarring acne (any type) Moderate acne unresponsive to oral& topical tx Acne (any severity) that is causingdepressive symptoms Excessive oiliness Sebaceous hyperplasia indications to use which medication? |
isotretinion (oral retinoid) |
|
|
Chronic suppurative (pus producing) disease of numerous recurrent abscesses found in the groin, axilla, below the breasts, and under the pannus. |
hidradenitis supperativa hallmark: double comedone obesity and smoking are risk factors |
|
|
weightloss stop smoking topical/oral antibiotics isoretinoin dapsone are treatments for? |
hidradenitis supperativa |
|
|
which drug is the only FDA approved drug for hidradenitis supperativa? |
humira |
|
|
chronic inflammatory condition of unknown origin that is most common in young adults of Celtic heritage |
rosacea |
|
|
Erythema & flushing Telangectasias Papular & pustular presentation of blank disease? |
rosacea can also come in an inflammatory version that has stinging/burning sensations and permanent telangectasias |
|
|
weather changes emotional changes foods are all blank for rosacea |
triggers |
|

|
rosacea |
|
|
What is the feature the differentiates acne from rosacea? |
comedones (acne) |
|
|
Granulomatous hypertrophy of the nose from severe,long standing, untreated rosacea |
rhinophyma |
|
|
Watery/bloodshot appearance Foreign body sensation Burning or stinging may be rosacea of the blank |
eye ocular rosacea |
|
|
What two classes of drugs are used to treat rosacea? |
topical or oral antibiotics/retinoids |
|
|
Peri-oral erythematous papules and/or papulopustules on an erythematous base sparing the vermillion border (not on lips) |
perioral dermatitis patients may report burning and tightness |
|
|
inflammation of the hair follicle as aresult of infection, follicular trauma, or occlusion (superficial) |
folliculitis |
|
|
deeperinflammation of the hair follicle, secondary to infection (deep) |
furuncle |
|
|
groupingof follicles with deep inflammation, secondary to infection (deep) |
carbuncle |
|
|
StaphFolliculitis¤Staphaureus Pseudomonal Folliculitis¤pseudomonas Pityrosporum Folliculitis¤Pityrosporum ovale types of? |
folliculitis |
|
|
Acuteonset of papules and pustules with pruritisor mild discomfort describes blank folliculitis? |
superficial |
|
|
Painfullesions with suppurative drainage, which can result in scarring and permanenthair loss describes blank folliculitis |
deep |
|

|
staph folliculitis Any hair bearing area but most common: Face,scalp, thighs, axilla,inguinal MCorganism is staphaureus |
|

key: pinpoint pustules with perifollicular flare |
pseudomonal folliculitis Hair bearing areas exposed tocontaminated water (hot tubs, swimming pools, pedicure tubs, etc.) |
|

|
pityrosporum folliculitis Back, chest & shoulders in young –middle age adults MCC is high heat, humidity and occlusion |