![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
49 Cards in this Set
- Front
- Back
|
Precancerous skin lesions: Actinic keratoses |

- Sun exposed areas - Small, rough, scaly lesions d/t prolonged sun exposure - Common in fair skinned people, typically on face biopsy to exclude squamous cell carcinoma tx: 5-FU topical, 5% imiquimod cream, topical diclofenac gel or photodynamic therapy |
|
|
Basal cell carcinoma |
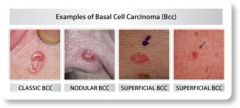
- Most common skin cancer* - Risk: sun exposure, fair skinned, most common on nose PE: Classic appearance pearly, smooth papule w/ roles edges & surface telangiectases (3 p's: pearly, pink, papule) *Metastasis is rare, but can be locally destructive Tx: surgery |
|
|
Squamous cell carcinoma |

- Less common than SCC - Risks: sun exposure, actinic keratoses, chronic skin damage, immunosuppressive therapy PE: crusting, ulcerated nodule or erosion, red conical hard lesions *Metastasis is higher than BCC, lower than melanoma *90% cause = HPV Tx: excision |
|
|
Melanoma |
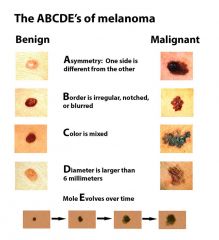
- Most aggressive form of skin cancer & #1 cause of death d/t skin cancer Risks: fair complexion, inability to tan, easily sunburned, red hair &/or freckles, numerous moles |
|
|
Steven-Johnson Syndrome (Erythema multiforme) |

- Target like, "bulls eye", multiple lesions - Abrupt eruption - Hives, blisters, petechiae, purpura & hemorrhagic that are painful - Mucosal surface involvement (eyes, nose, mouth, esophagus) - Fever or flu-like sx before rash Causes: medicines (PCN, sulfa, barbs, phenytoin), infections, malignancies Tx: Supportive *HIV pts @ inc risk |
|
|
Skin clinical findings: Benign |
Seborrheic keratoses: senile wart, raised pink, d/t aging, tx: ammonium lactate Xanthelasma: raised plaque around eye -- sign of hyperlipidemia Melasma: mask of preg or birth control, brown/tan stains upper cheeks & forehead, permanent, lighten over time Vitiligo: hypopigmented patches of skin Cherry angioma: benign small red papules, inc w/ age Lipoma: painless cystic tumors on subq layer of skin (neck, trunk, legs, arms) Nevi (moles): round macules to papules Xerosis: inherited, extremely dry skin Acanthosis nigricans: thickening of skin (neck & axilla). a/w DM, metabolic syndrome, obesity, GI cancer Dermatofibroma: legs most common, slow growing round firm nodule -- fitzpatrick's sign (retracts when squeeze) Lentigines: small brown patches on elderly |
|
|
Psoriasis |
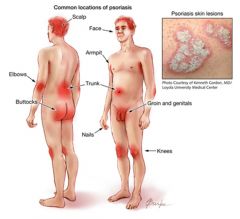
- Inherited, chronic skin disorder - Pruritic erythematous plaques w/ fine silvery white scales, symmetrical (scalp, elbows, knees, sacrum, intergluteal folds) - May also c/o swollen joints (a/w arthritis) Tx: topical corticosteroid or retinoids *alcohol can trigger a lesion |
|
|
Atopic dermatitis (eczema) |

- Chronic inherited skin disorders, extremely pruritic rashes (hands, flexural folds, neck) - Small vesicles that rupture leaving bright red weepy lesions - Exacerbated by stress, winter, etc. - A/w asthma, allergic rhinitis, multiple allergies Tx: 1st line = topical steroids - Mild = hydrocortisone 1-2.5% - Medium = triamcinolone - Benadryl - Skin lubricants (eucerin) - Hydrating baths followed by immediate application of eucerin *Avoid drying skin - no hot baths, harsh soaps |
|
|
Contact dermatitis |

- Inflammatory skin rxn d/t contact w/ irritating external substance (i.e. poison ivy, nickel) - Can be single lesion or generalized rash occurring w/in minutes to several hours - Multiple, bright red, pruritic lesions evolve into bullous or vesicular lesions, easily rupture Tx: Calamine lotion, topical steroids (i.e. triamcinolone) ointment over cream - Severe (>20% affected, or involving face, hands, genitals prescribe a systemic corticosteroid) = oral prednisone x 12-14 days |
|
|
Bacterial |
Impetigo Cellulitis Follicular: folliculitis, furuncle, carbuncle, hidradenitis suppurative |
|
|
Impetigo |

BACTERIAL - Acute superficial skin infection (S. pyrogenes or S. aureus) - Very contagious, pruritic, common warm & humid weather - 2 types: bullous & nonbullous forms Nonbullous - Erythematic macule rapidly evolves into vesicles or pustule, ruptures, contents dry, leaves crusted honey colored exudate - Can use just topical abx Bullous - Bulla contains clear, yellow fluid that turns cloudily/dark yellow - Rupture easily (1-3 days) leaving rim of scale around red, moist base - Requires systemic abx - Children & teens, itchy pink to red lesions that become bullous, then crusty & maculopapular -- after rupture lesions are covered w/ honey colored crusts (dried serous fluid) Tx: Cephalexin x 10 days (allergy: z-pak), & bacitracin |
|
|
Acute cellulitis |
BACTERIAL
- Acute skin infection of the deep dermis & underlying tissue - Usually caused by Gram (+) bacteria (staph) - 2 forms: purulent & non-purulent - Diffused pink to red colored skin, poorly demarcated margin that grows larger, lesion is hot, may be abscesses or draining of purulent green d/c
Tx: PO Clinda, Cephalexin, Doxycycline
*Erysipelas is superficial stage - Caused by S. progenies - Amox, z-pak |
|
|
Furuncle |

BACTERIAL - Infected hair follicle that fills w/ pus - Red bump, hot to touch *small abscess Tx: I&D, warm compress, no abx unless comorb/immuno/accomp by cellulitis) |
|
|
Carbuncle |

BACTERIAL - Several furuncles that coalesce to form a large boil/abscess - Hot, tender to touch - C&S - Purulent drainage Tx: - Non-MRSA, nonpurulent: dicloxacillin x 10 days (cephalexin or clinda) - PCN allergy: macrolids, 2nd gen cephalosporins, clinda - Suspect MRSA: bactrim DS x 10 days (or doxy or clinda) - Td booster Follow-up: w/in 48hrs Refer if: systemic sx (fever, toxic), worsening, not responding w/in 48hrs of tx, spreading, pt immunocompromised Complications: osteomyelitis, septic arthritis, sepsis |
|
|
Hidradenitis suppurative |

BACTERIAL aka acne inversa - Chronic follicular occlusion disorder - Intertriginous skins (folds-axilla) -- apocrine glands - Prevalent in women Tx: Intralesional kenalog (corticosteroid), I&D, sometimes surgery |
|
|
Purulent (abscess/carbuncle/furuncle) |
Mild - I&D, warm compress Moderate - I&D, C&S - Systemic abx: bactrim, doxycycline - Therapy by C&S results: MRSA --> bactrim, MSSA --> dicloxacillin, or cephalexin |
|
|
Nonpurulent (cellulitis/erysipelas/impetigo) |
Mild - Systemic abx: PCN, Cephalexin, Dicloxacillin, Clinda- Topical therapy indicated (impetigo only) --> mupirocin Moderate - IV abx: PCN, Ceftriaxone, Cefazolin, Clinda |
|
|
Paronychia |

- Acute local BACTERIAL skin infection of proximal or lateral nail folds that resolves after abscess drains - Chronic cases a/w on onychomycosis Tx: soak warm water (20min, 3x/day), apply topical abx, abscess I&D |
|
|
Scarlet fever |

BACTERIAL - "sandpaper" rash on face, neck, trunk, arms, legs - strep throat, pharyngitis - strawberry tongue Tx: PCN |
|
|
Bites: human & animal |
Human: dirtiest bites Animals: cat bites highest rate infxn - Need C&S - Do not suture if high risk for infxn, or >12hrs old - Tetanus Tx: augmentin x 10 days (PCN allergy: clinda plus fluroquinolone) Follow-up: 24-48hrs
Rabies: bats, raccoons, skunks, foxes, coyotes, cats --> rabies immune globulin plus rabies vaccine |
|
|
Acne vulgaris |
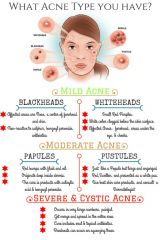
- Pustular disorder Mild acne: <20 comedones, or <15 inflamm lesions - tx: TOPICAL only - benzoyl peroxide (antibacterial) OR - topical retinoid Moderate acne: 20-100 comedones, or 15-20 inflamm - tx: topical PLUS abx - topical combo (benzoyl + retinoid) OR retinoid + benzoyl + abx Severe acne: >5 nodules, or inflamm >50 - combo of PO abx + topical retinoid + benzoyl (consider isotretinoin (accutane)) |
|
|
Scabies |

- Communicable skin dz skin to skin contact - Place items in plastic bags for 1wk (mites don't live >3-4 days) - Common to see over waistband area Tx: permethrin lotion left on for 8-14hrs |
|
|
Lyme |

- infection caused by b. burgdorferi, tick - must feed on human host >24hrs to transmit spirochete Stages: 1. Early localized dz: mild flulike sx, single annular lesion w/ central clearing (erythema migrans), resolve 3-4wks w/o tx 2. Early disseminated infxn: months later, classic rash reappear w/ multiple lesions, usually accompanied by arthralgias, myalgia, HA, fatigue 3. Last persistent infxn: 1yr after initial infxn, MSK sx persist (joint pain, arthritis), neuropsychiatric sx (memorial probe, depression, neuropathy) Dx: serum testing Western blot assay for IgM antibodies Tx: antimicrobials (doxy, ceftin, amoxicillin, macrolides) 14-21 days w/ earlier dx; up to 28 days more adv dz |
|
|
Burns |
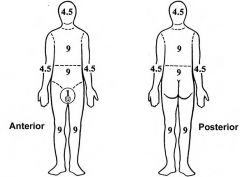
*Thermal, chemical, electrical, radiation 1st degree: skin blanches with ease, dry (i.e. sunburn) 2nd degree: blisters, moist (i.e. chemical) 3rd degree: pain minimal, white & leathery, dry, areas surrounded by painful 1st & 2nd degree burns (i.e. flame) --> REFER Tx: prevention of infection by topical abx (i.e. silvadene) *Refer if involve high function areas (hands, feet, face, genitalia) |
|
|
Sun safety |
<6mo do NOT apply sunscreen >6mo apply minimum SPF 15 q2hrs |
|
|
Viral |
Herpes Molluscum contagiosum HPV Pityriasis rosea Herpetic whitlow |
|
|
Varicella |
VIRAL Nonclustered lesions at variety of stages tx: antiviral meds (acyclovir) 24-48hrs of eruption vaccine: varivax @ 4 & 6yo |
|
|
Herpes zoster |
VIRAL typically >50yo, possible any age with hx chickenpox vesicles in unilateral dermatomal pattern, slowly resolving w/ crusting complications: postherpetic neuralgia, ophthalmologic involvement, superimposed bacterial infxn tx: antivirals w/in 72hrs of eruption *Involve EYES --> Refer! vaccine: zostavax 1 dose @ >60yo |
|
|
Molluscum contagiosum |

VIRAL - Smooth, skin colored dome-shaped, pearly papules w/ umbilicated centers - Cause: pox virus, skin to skin, sex - Contagious until ALL lesions disappear Tx: q2-3wks for 6mo, curette, cryo (liquid nitrogen), imiquimod |
|
|
HPV |
VIRAL Verruca vulgaris (common warts) - OTC: salicylic acid - Face: tretinoin - Genital: imiquimod Verruca plantaris (plantar warts) Verruca planae (flat warts, HPV3) - Children, young adults - Forehead, cheeks, nose, perioral - Common cause: shaving - Tx: imiquinod topical Condyloma acuminata (genital warts) - Rough on surface, worse during preg |
|
|
Pityriasis rosea |
VIRAL - Common children & 15-40yo - Self limiting viral exantham - Sometimes a/w URI - HAROLD PATCH start on trunk --> develops smaller lesions on body, 50% pruritus, lasts 5-8wks Tx: symptomatic, calamine lotion, antihistamin, topical/oral steroids |
|
|
Herpetic whitlow |

VIRAL - skin infection of finger(s) caused by herpes I or 2 - direct contact Tx: self-limiting |
|
|
Measles |

VIRAL aka rubeola - fever, malaise, 3 c's: coryza, cough, conjunctivitis - Koplik's spots: small, white round spots on base of buccal mucosa - Sx: don't appear until 10-14 days after exposure: cough, runny nose, inflamed eyes, sore throat, fever, & a red, blotchy skin rash Tx: none |
|
|
Fifth's disease |
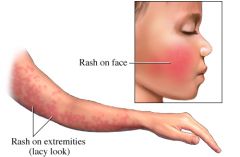
Parvovirus 19 - 5-15yo - URI sx 1st RASH 1. slapped cheeks 2. maculopapular rash on extremities 3. rash subsides, painful/swollen joints |
|
|
Coxsackie virus |
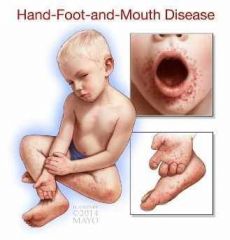
VIRAL
aka hand, foot, mouth dz - Enterovirus - sore throat, rash, blisters - fever, oral vesicles on buccal mucosa & tongue - lesions on palms, plantar surface of feet, buttocks |
|
|
Fungal |
Tinea capitus Tinea corporis Tinea cruris Tinea pedis Tinea/pityriasis versicolor Intertrigo Onychomycosis |
|
|
Tinea capitus
|

FUNGAL aka ringworm of the scalp Sx: - Scalp, broken hair shafts - versus alopecia (has NO black dots, hair shafts) - pruritic - a/w scalp injury, moist hair, poor hygiene - Kerion: swollen, boggy, fever, pain, lymph, pus --> steroids Dx: KOH --> hyphae Tx: Griseofulvin PO, antifungal shampoo, topical Rx ineffective as monotherapy! |
|
|
Tinea corporis
|

FUNGAL aka ringworm - body - pruritic, circular, red, scaly patch - CENTRAL CLEARING - well demarcated - Common: adults caring peds w/ T. captius, athletes skin-skin, immunosupp. Tx: topical antifungal imidazole (if immunosupp PO lamisil (monitor liver) |
|
|
Tinea cruris |

"jock itch" groin - small, red patch w/ crust & scaling --> spreads peripherally w/ curved well defined edges Tx: topical antifungal (lotrimin, lamisil), zeazorb powder, PO 2wks if severe |
|
|
Tinea pedis |

FUNGAL "feet" - moisture, poor vent in shoes - can cause t. cruris - may be a/w onychomycosis - macerated hyperkeratotic plaques in interdigital webs OR dull redness w/ scaling on plantar Tx: topical econazole, severe: oral, KEEP DRY! |
|
|
Tinea/pityriasis versicolor |
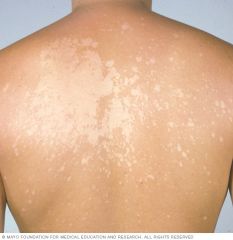
YEAST - chronic, asx, warm climates, fine scaly guttate OR nummular patches, yellow-brown macules - hypopigmented on dark skin - NEVER on face or legs Tx: PO ketoconazole, selenium sulfide OR ketoconazole shampoo, topical |
|
|
Superficial candidiasis |
- Superficial skin infection from yeast - Inc w/ warmth/humidity, friction, dec immunity - Infects skin (candidal intertrigo), mucous membranes (thrush, vaginitis), and systemically Sx: - External: bright red & shiny lesions, itch, burn, can be under breast, may have satellite lesions (small red rashes around the main rash) - Oral thrush: severe sore throat w/ white adherent plaques w/ red base --> give oral nystatin Tx: Nystatin powder &/or cream in skin folds *HIV esophageal candida infxns treated w/ systemic antifungals |
|
|
Intertrigo |

CANDIDA - mucosal surfaces &/or skin folds - Rxs: obese, DM, recent abx, or steroids, immunosupp, chronic moisture - erythema erosions, tissues, itchy, burn Tx: topical antifungal, nystatin or imidazole ointment, zeazorb powder |
|
|
Onychomycosis |
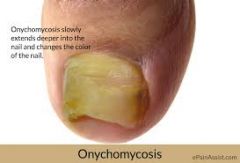
FUNGAL - aka dermatophytosis of the nail - chronic disfiguring disorder of the nail - nails are dull, thickened, lusterless Dx: hyphae of nail scrapings mixed with KOH Tx: antifungals (diflucan, lamisil) |
|
|
Kawasaki disease |
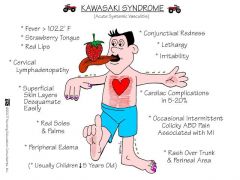
Unknown origin Sx: - Early stages: rash & fever, peeling skin on palms & bottom of feet - Late stages: inflamm of medium size blood vessels (vasculitis). It also affects lymph nodes, skin, & mucous membranes, such as inside the mouth Tx: symptomatic |
|
|
Infant derm |
Hemangioma - benign tumor of endothelium - often NOT present @ birth - rapid growth from day 1-6mo - tx: po propranolol or systemic corticosteroids to slow growth; watchful waiting Port wine lesion - present @ birth - blanch able red to dark pink - will darken as child grows, does NOT regress! Mongolian spots - blue-black macular flat lesions usually buttocks - most common: asians, AA, NA - lightens over time, NO tx Milia - raised white bumps on nose or cheeks - No tx, resolve few weeks on own Erythema toxic neonatorum - occasionally present @ birth, usually appear 1st 48hrs of life (resolves 5-7 days) - erythematous papules progress or pustular lesions - No tx, resolves on own Acne neonatorum - androgens from mother or infant - face, lesions start 1st mo, lasts 1-2mo, self-limiting Atopic dermatitis/eczema - present @ birth to 2yo - hydrate w/ daily ointment Seborrheic dermatitis (cradle cap) - scalp, face, groin, underarms - erythematous plaque/scales, common 3wks-12mo - apply emollient overnight, can remove w/ soft brush in AM Keratosis pilaris - genetic, acne like tiny bumps on skin, common outer aspect of upper arm - rough skin texture, asx or itch - NO cure, use mild soapless cleansers to prevent dryness - childhood & adolescence: improves w/ age, periods of remission & exacerb, worse in cold/dry weather |
|
|
Acanthosis nigricans |

- hyper pigmented velvety plaque on skin fold areas (neck, axilla) - d/t insulin resistance or inherited, DM |
|
|
Ointment |
Do NOT use ointment in intertriginous areas or perineum |
|
|
Cafe au lait spots |
>5 should be concerned, can indicate neurofibromatosis type I |