Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
99 Cards in this Set
- Front
- Back
|
Bonding describes…
|
A process of attachment (adhesion)
*Per Mrs. Fox, 2 materials become 1.* |
|
|
What will enamel bond to?
|

Sealants
Composite Resins (any class) Porcelain (inlay, onlay & veeners) |
|
|
What will dentin bond to?
|

Composite Resins (Class 1,2, 3 & 4)
Porcelain (inlay, onlay & veneers) |
|
|
Why do we not bond a class 5 restoration to dentin?
|

A class 5 is at the CEJ. We would be cutting into enamel or cementum (at root surface).
We wouldn't be going so deep as to reach the dentin. |
|
|
Describe an "inlay"
|
Doesn't include a cusp tip.
|
|
|
Describe an "onlay"
|
It does include a cusp tip.
|
|
|
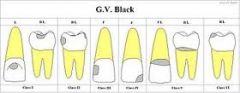
On the GV Black Classificatin of carious lesions, describe a Class I & Class II lesion
|
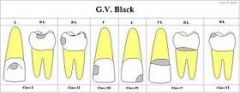
Class I: Occlusal area & buccal or lingual pits.
Class II: Posterior Interproximal |
|
|
On the GV Black Classificatin of carious lesions, describe a Class III & Class IV lesion
|
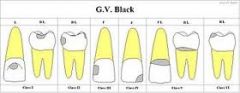
Class III: Anterior Interproximal
Class IV: Anterior Interproximal including the incisal corner |
|
|
On the GV Black Classification of Carious Lesions, describe a Class V & VI carious lesion
|
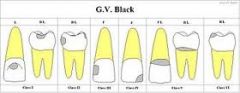
Class V: Gingival at facial or lingual
Class VI: Cups Tip |
|
|
Which materials do we most often see in bonding?
|

Amalgam to enamel
Comoposite (resin) to enamel *Remember, there is a chemical reaction happening. The attraction is between the different molecules of each surface.* |
|

What is the 2 step prep for bonding?
|
1) Remove plaque & debris
2) Etch or condition the surface w/most common acid. |
|
|
What is the most common acid used in the prep for bonding?
|
10-38% phosphoric acid
|
|
|
What is the purpose of the 10-38% phosphoric acid?
|
To demineralize (etch) the surface-->create roughness & allow for microscopic porosity.
*These two items allow for better bonding.* |
|
|
What does the term "polymerizes" refer to?
|
Curing/Hardening (baked, cooked)
|
|
|
When bonding to an etched surface, now that the surface is "porus" what does this mean for the resin or primer?
|
The etched or porus surface allows the resin/primer to flow over and into the pores. It allows for better retention.
|
|
|
What does the resin or primer do after flowing over the surface?
|
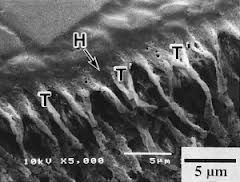
It polymerizes (hardens) and creates resin "tags" in the pores creating a mechanical bond.
|
|
|
When the material flows into the pores, what type of bond is created?
What is the material called that flows into the pores? |
Physical or Mechanical Bond
The tags |
|
|
What is it about the bonding process that is allowing for the physical or mechanical bond?
|
The resin tags, by extending into the pores and "locking" in place
|
|
|
Good wetting is an example of what type of surface energy?
|
High Surface Energy-->the product will flow!
|
|
|
If the product is "beading up" what type of surface energy do you have?
|
Low surface energy
|
|
|
How is bond strength determined?
|

By Tensile force …pulling in opposite directions
|
|
|
Bond strength is measured in MPa's (Know this for Boards!) What does MPa stand for?
|
Mega Pascals
1MPa = 150psi |
|
|
When bonding to Enamel what level of MPa is considered good?
|
30 Mpa…(4500psi)
|
|
|
Do you need more or lessing bonding when "attaching" to dentin? Why?
|
Less
Because dentin has tubules present which the product will naturally flow into and create a better bond. |
|
|
What if there is fluid in the dentinal tubules?
|
The fluid can reduce the bonding…as such we would use products that bond in the presence of fluid.
|
|
|
What factors can impact the effects of bonding? (4 items)
|
Moisture
Chewing Pressure Temperature Changes Expansion & Contraction |
|
|
If the bond eventually fails what can be the result?
(2 items) |
Sensitivity
Root Caries (both due to the loosening of the bond) |
|
|
What is the purpose of a dental dam?
|

It serves as a safet net!
|
|
|
Why is enamel etching often blue in color?
|

So you can see where its going.
It's also gelatinous so you can "control" where it goes. |
|
|
What material is actually being removed in the etching process?
|

The hydroxyapatitate of the enamel rods
|
|
|
What is the optimal Enamel etching time for permanent teeth?
|
20-30 seconds (includes both enamel & dentin)
*Can be as little as 10 seconds if etching enamel only. * |
|
|
What is the Enamel etching time for primary teeth?
|
60 seconds
|
|
|
How does the surface appear after etching?
|
"frosty"
|
|
|
What do you have to do after placing the acid for the proper amount of time?
|
Rinse it away! Avoid getting it on any soft tissue.
|
|
|
What 6 items can make up the smear layer?
|
1) cut tooth structure
2) plaque 3) bacteria 4) pellicle 5) saliva 6) blood **Can't simply be washed away with Air or Water as its very sticky.** |
|
|
What does the smear later do in relation to dentin?
|
Interferes with the bonding to dentin.
|
|
|
What has to happen to remove the smear layer?
|
You have to etch it.
*The etching happens at the same time..the enamel etch and the dentin etch. Its not two separate processes.* |
|
|
What will etching the dentin remove?
|
The smear layer!
*Think of the smear layer as "the sludge". |
|
|
What is the optimal Dentin etching time of Permanent teeth?
|
10 seconds..so if doing a deeper restoration you're etching both enamel & dentin for a total of 20-30 seconds.
|
|
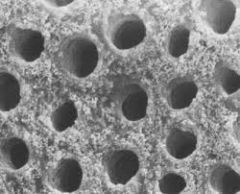
What is found inside the dentinal tubule?
|
odontoblasts!
|
|
|
Why does the dentinal tubule need to be kept partially moist?
|
It allows for a better bond.
*Think of it as a sponge..a dry sponge won't absorb anything but a damp sponge will.* |
|
|
What is usually used when bonding to enamel?
|

A curing light
|
|
|
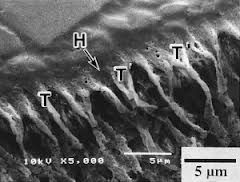
When bonding to enamel what needs to be penetrataed to ensure adhesion?
|
The material needs to penetrate enamel rods…the tags will secure the resin
|
|
|
What does a shallow or Class I composite restoration bond to?
|
Etched rods
|
|
|
What bond is greater? End etched rods or side etched rods?
|
End etched rods
|
|
|
What is a class I restoration bonding to?
|
End etched rods…coming in from the occlusal surface. A class II or III is bonding to the side etched rod as it is an interproximal restoration.
*Sometimes the Dr will carry the prep into the occlusal surface to ensure a little better bond.* |
|
|
What are some reasons there might be a failure to bond?
|
Failure to isolate the area
Surface contaminants-->saliva, blood, debris |
|
|
What has to happen if the bonding area is contaminated…like if a Pt runs their tongue over the area?
|
Must re-Etch for 10-15 seconds
|
|
|
When bonding to dentin what is used 1st? 2nd?
|
1st: primer (hydrophillic-->allows to penetrate H20)
2nd: use adhesive resin over primer |
|
|
What is this 2 step bonding process called that is currently being used?
|
Wet Dentin Bonding
|
|
|
What is the primer material for dentinal bonding?
|

Acetone
*It will evaporate so apply twice.* |
|
|
What are 3 modes of curing?
|
Self Cure--> chemical reaction between the 2 materials Light Cure-->accelerates the bond using a blue light wave range.
Dual-cure-->Combination of the two. |
|
|
Where does microleakage take place?
|

At the junction of the restoration and the tooth
|
|
|
What can cause microleakage?
|
Expansion/contration of the area.
|
|
|
What does microleakage contribute to?
|
Recurrent decay, sensitivity, and possibly the loss of the restoration
|
|
|
What is the theory behind hypersensitive teeth?
|
Hydrodynamic theory!
|
|
|
What happens if the resin is cured in increments?
|
You can ensure each layer is completely cured and thus reduce the opportunity for shrinkage-->microleakage.
|
|
|
What are some clinical applications of when bonding is utilized?
|
Porcelain
Metal Amalgam Orthodontic Brackets Endodontic Posts |
|
|
Where are composite (tooth colored) restoration used?
|

Anteriorly and now often in the posterior region as well.
|
|
|
What is added to the composite to match the tooth?
|
Pigments
|
|
|
What is mixed together to get the composite?
|
Organic resin matrix & Inorganic filler particles.
(They are joined by saline which causes the organic & inorganic elements to bond.) |
|
|
What is the most common resin matrix called?
|
Bis-GMA
|
|
|
The filler components of resin/composite restoration does what?
|
Makes the resin stronger & resistant to wear, allows for either radiolucency or radiopacity.
|
|
|
Composites will wear. The irregular surface is a result of:
|

erosion and loss of filler particles.
|
|
|
What are the 3 types of polymerization?
|
1) Chemical cure (self cure)
2) Light Cure 3) Dual Cure (combination) |
|
|
What 2 items make up the self cured composite?
|
Base + Catalyst
*Usually supplied as a paste, in jar, or syringe cartridge-->sometimes a preloaded cartridge.* |
|
|
What type of curing is most comon?
|

Light Curing
*There is no mixing involved and it gives the DH more control* |
|
|
What do you need to be cautious of when light curing?
|

That your "loops" light isn't on or any operatory light.
*Be sure to cure in 2mm increments* |
|
|
What makes up a dual cure composite?
|
2 paste system-->cure light will initiate the set reation.
*Its ideal for core buildup of endo treated teeth.* |
|
|
What is a hybrid composite?
|
A combination of Macrofilled (big parts) & Microfilled (little parts) elements.
|
|
|
What is a flowable composite?
|

A light cured, low viscosity composite resin.
*Delivered from a syringe* |
|
|
What is a packable composite?
|
A light cured, highly viscous material…"scooped" into site, doesn't spread.
|
|
|
What is a smart composite?
|
One that releases fluoride into the prep over time.
|
|
|
What is a core build up?
|

Adding material so a crown can be placed..Is used if there isn't enough tooth structure for a crown, so its "built up."
|
|
|
Provisional is another word for _________.
|
Temporary
|
|
|
What are some characterists of Macrofilled composites? (6 items)
|
Large filler particles
Hard to polish Will become rough Will stain Stronger than microfilled composites Require replacement sooner-->will breakdown Rarely used-->due to improved products. |
|
|
What did microfilled composites replace?
|
Macrofilled composites
|
|
|
What are some characterists of Microfilled composites? (4 items)
|
Smooth/shiny surface
Poor strength Not suitable for class I, II or IV restorations Used primarly for esthetic anaterior fills |
|
|
What can be said about Hybrid Composites? (4 items)
|
Best Product to date
Contains both micro & macro size fillers Provides both strength & polish Can be used in both posterior & anterior. *Do know that composites will shrink due to porosity.* |
|
|
Flowable composites can be __________________________.
|
placed directly in to the prep…they adapt well to small areas.
*Sometimes they are used as sealants.* |
|
|
When are packable composites utilized?
|
Class I & Class II restorations (Occlusal & Posterior interproximal restorations)
*They are marketed as substitues for amalgams..more for posterior occlusal surfaces.* |
|
|
In addition to fluoride, what can smart composites release?
|
calcium & hydroxyl ions…remineralizes effects of acid
|
|
|
When would core buildup composites be utilized?
|

For badly broken down teeth before placing a crown.
*Some contain pigment to contrast the color of tooth structure so its easier to place the crown…can see it better.* |
|
|
When would provisional restorative composites be utilized?
|
They are temporary fills for lab processed restorations like: Inlays, onlays, crowns & bridges.
|
|
|
What are some physical properties of composites? (8 items)
|
1) Biocompatibility
2) Strength 3) Wear 4) Polymerization Shrinkage 5) Reduced or No Thermal Conductivity 6) Elastic Modulus (Thermal expansion similar to tooth structure) 7) Water Sorption (can stain) 8) Radiopacity..look less opaque than metal. |
|
|
What are some atributes of composite resins? (6 items)
|
1) Used on all class of restoration
2) Not as durable as amalgam 3) More Costly $$ 4) Tooth Colored 5) Prep is more conservative than amalgam..don't remove as much tooth structure 6) May be temperature sensitive-->due to porosity of material. |
|
|
What can be said about choosing a shade when using composites?
|

You may have to customize the shade by mixing 2 shades together.
Can't always match Most products come with a shade guide. |
|
|
Layering of a composite is used…..
|
to design a specific color…start at cervical 1/3.
|
|
|
What are 3 clinical consideratins of composites?
|
1) Shelf life of product
2) Dispensing--reusable syringe, don't usually use entire amount so watch cross contamination 3) Cross Contamination--use barrier, wipe with disinfectant |
|
|
Glass Ionomer Cements tend to be ____________________
|
more liquid in nature.
They aren't as strong as composites! |
|
|
What is a Type I Glass Ionomer cement used for?
|

Cementation for crowns & bridges
|
|
|
What is a Type II Glass Ionomer cement used for?
|
Restorations
|
|
|
What is a Type III Glass Ionomer cement used for?
|

Liners & bases for cavity preps..helps with bonding & sensitivity
|
|
|
Feldspar, Quartz and kaolin are all names refering to…..
|

Porcelain restorations
|
|
|
PFM stands for?
|

Porcelin Fused to Metal
|
|
|
PBM stands for?
|
Porcelin Baked to Metal
|
|
|
Porcelin will ________ under stress.
|
Fracture…but it is strong enough to use in posterior teeth.
|
|
|
What are some DH considerations for porcelain?
|
No direct contact with Ultra Sonics!
Minimal hand scaling Always use a soft brush CPR prophy paste can be used for stain |
|
|
Porcelain Veneers will/will not disturb the natural tooth?
|

Will Not!
They are very thin and the incisal edge usually wraps around to the lingual area. |