Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
14 Cards in this Set
- Front
- Back
|
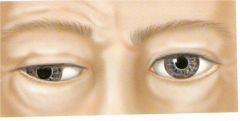
What's Horner syndrome?
Name the 4 symptoms |
Ptosis
Miosis Anhydrosis Enophthalmos --ptosis (drooping upper eyelid from loss of sympathetic innervation to the Müller or superior tarsal muscle --miosis (constricted pupil..loss of innervation to pupillary dilator muscle) --Enophthalmos (the impression that the eye is sunk in) --anhidrosis (decreased sweating) |
|
|
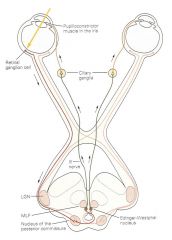
pupillary light reflex
whats the afferent and efferent? |
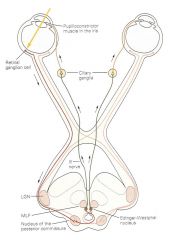
Amount of light entering eye is regulated by pupillary light reflex.
Afferent limb is optic nerve Two efferent limbs – one to each sphincter pupillae Hence, reflex is consensual. Consensual = stimulus should evoke pupillary constriction in both eyes The pupillary reflex pathway begins with retinal ganglion cells, which convey information from photoreceptors to the optic nerve (via the optic disc). The optic nerve connects to the pretectal nucleus of the upper midbrain, bypassing the lateral geniculate nucleus and the primary visual cortex. From the pretectal nucleus, axons connect to neurons in the Edinger-Westphal nucleus, whose axons run along both the left and right oculomotor nerves. Oculomotor nerve axons synapse on ciliary ganglion neurons, whose axons innervate the constrictor muscle of the iris. |
|
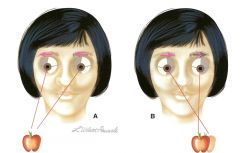
where's the lesion?
If neither pupil constricts if only one pupil constricts |
-afferent limb (CN II)
-CN III (ipsilateral to deficit) |
|
|
common causes of damage to the oculomotor nerve are:
--Aneurysm of ______ --Pressure on oculomotor nerve due to temporal herniation through tentorial incisure. Such herniation may pressage imminent death. |
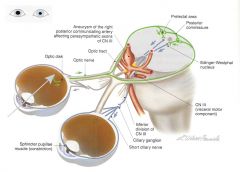
posterior communicating artery
|
|
|
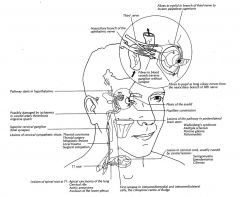
how do sympathethics get to the eye? (and innervate dilator pupillae)
|
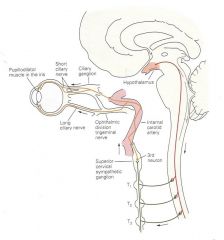
Damage to hypothalamus or pons, and some opiates, result in constricted, reactive pupils, signs of sympathetic impairment.
(reactive to light->3 is intact) |
|
what's this?
|
down and out eye
|
|
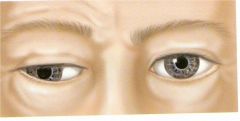
pathophys of down and out eye?
|
caused by lesion in CN III!!
“Down and out” eye caused by unopposed action of lateral rectus (VI) and superior oblique (IV). DOWN bc of SUPERIOR OBLIQUE OUT bc of LATERAL RECTUS 1) ptosis: due to inactivation of levator palpebrae superioris 2) dilated pupil: sphincter pupillae muscle inactive (parasympathetics); unopposed action of dilator pupillae: elevation of eyebrow due to contraction of frontalis to compensate. Lack of accommodation: ciliary m. inactive (parasympathetics) Strabismus (inability to direct both eyes to same object) producing diplopia; |
|
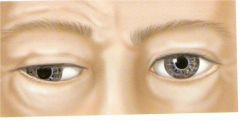
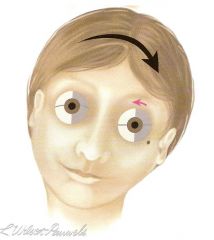
what's wrong?
|
Patient cannot abduct left eye: left abducens (VI) palsy
|
|
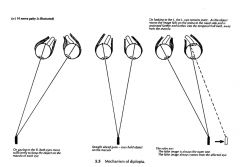
which CN is affected?
Patient has double vision when looking down (going down stairs, reading book), and when looking straight ahead, unless head tilted to left. |
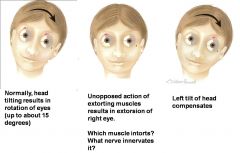
trochlear
superior oblique intorts the eye!!! if damaged, unopposed extortion |
|
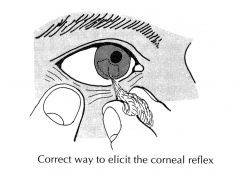
what nerve is this guy testing?
|
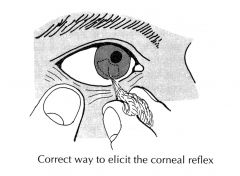
corneal reflex: 5, 7
trigeminal (afferent) facial (efferent) |
|
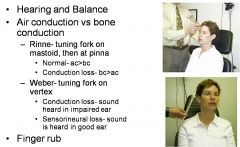
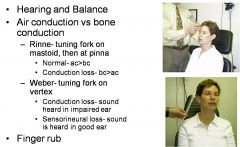
Testing CN 8
|
|
|
|
how can you test 9, 10?
|

Swallow
Dysphagia for liquids and solids Palate rise Gag Reflex (A & E) Voice exam |
|
|
what's being tested?
|

Tongue movement
Tongue deviation Deviated to the affected side Atrophy Fasciculations Upon protrusion, the tongue will deviate TOWARD the side of the lesion (i.e., same side). This is due to the unopposed action of the genioglossus muscle on the normally innervated side of the tongue (the genioglossus pulls the tongue forward). Remember, the genioglossus arises laterally in the tongue and inserts on the midline of the mandible. |
|
|
What is the connection between the cranial nerves responsible for horizontal eye movements?
|
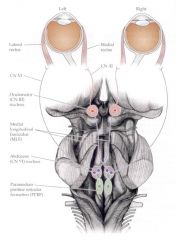
|