Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
10 Cards in this Set
- Front
- Back
|
1. What is the role of the corpus callosum?
2. What are the strategies for testing disconnections between the hemispheres? |
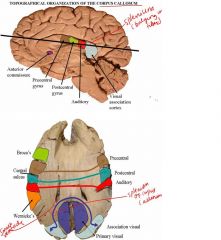
1. Various parts of the cerebral cortex are anatomically linked via the white matter. The two hemispheres are by the corpus callosum and the anterior commissure (the interhemispheric connections)
Not that much ventricle because we are too high Corpus callosum is involved in cortical interconnections Postcentral is somatosensory and somatotopically organized by dermatomes (VPL and VPM)! Primary visual has no connection by the splenium of the corpus callosum The association visual cortex are connected by the splenium! The speech cortex is Wernicke’s, most ppl have the left as the dominant area Broca is another speech area 2. Disconnections between the hemispheres is due to callosal lesions and here are 4 strategies to test for the disconnections: 1. USE LATERALIZABLE SENSATIONS AND RESPONSES Sensory: Visual (homonymous hemifields) and somatosensory Motor: Manual (palpation, pointing), speaking, writing 2. Lateralize input and output to left hemisphere (no callosal connections involved). 3. Lateralize input and output to right hemisphere (no callosal connections involved). 4. Lateralize input to one hemisphere and output to the other (callosal connections involved). NOTES: Response latralizaion, if you use the left hemisphgere and there is a pyramidal decissation Sensory decussation Motor decuissation Can we lateralize vision to one hemisphgere to the other? Yes, fibers from the 2 retinas projerct to both hemiphgers, ipsilatareally and contralaterally The nasal retinas do cross One must test with the para foveal so that stimulus from the left fallsd on the right retina and goes to tge right hemidsphgere There is a visual field method Sensory input frtom one hemisphere and a motor output to the other so we need the copus callosim for this interactiion!! Motor cortec No control for eye movements that can shift their info Tachiato ….. |
|
|
Describe HEMI-ALEXIA OF THE LEFT VISUAL FIELD?
|
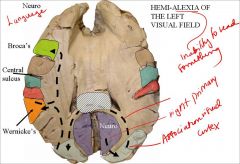
Hemi-alexia (a callosal syndrome) involving reading.
Lesion. Blockage or destruction of posterior cerebral artery causing destruction of the splenium of the corpus callosum. Symptoms. The patient cannot read in the left visual field (though there is no field defect). This is apparent only under controlled testing conditions. Mechanism. Visual input to the right hemisphere has been isolated from the left, (speech) hemisphere. NOTES: If we study portions of the c Posterior cerebral artery is the splenium of the cortpus callosum You can cut the splenium and you study only visual interconnections What did you see involved here? You see is the auditory system, I saw the word “neurio” wernicker lets you intrprete that you said neuro, so you know that the whople pthway is okay If you block this, due to lesion, the behavior is not understoold or repeated so this is You see it but you cannot intereprete it If in trhe right side, there will be no alexia Only the left visuial field is hemi alexic because |
|
|
Describe APRAXIA AND AGRAPHIA OF THE LEFT HAND?
|
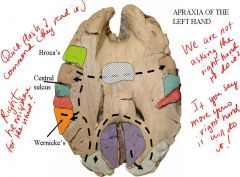
APRAXIA AND AGRAPHIA OF THE LEFT HAND
Lesion: anterior body of corpus callosum Symptoms: Patient can carry out verbal commands with the right hand but not with the left hand Mechanism: Pathway goes from Wernicke's area via arcuate and superior longitudinal fasciculus to left motor association cortex, then via corpus callosum to right motor association cortex and then to the adjacent motor cortex. Lesion disconnects verbal stimuli from gaining access to the hand area of the right motor cortex. If one assumes in the patient that the speech cortices are localized to the left hemisphere, then the verbal command "show me with your right hand how you use a hammer" travels via CN VIII to Heschl's gyri, then to the left planum temporale and on to Wernicke's for decoding of meaning to these stimuli. Wernicke's forwards this command to Broca's, which in turn activates the arm and hand area of the left precentral gyrus-the upper motor neurons which drive the right hand (CONTRALATERAL) -No no problem so far! If, instead, the verbal command is "show me with your left hand how you use a hammer", then trace out the same pathways. However, now the right precentral gyrus must be accessed to activate the left hand. Therefore, Broca's must transmit the command to the right hemisphere via callosal connections. With lesion of these callosal fibers left-right intercommunications are broken, and the right frontal lobe is thus clueless as to what is being asked. NOTES: How do you yawn or how do you use a hammer?? Can’t do this means APRAXIA!! So you are using the precentral gyrus of the right hand A phtway ..the auditory system is not lateralizatble!!!!! Cause there is bilateraty projection with the superior olives Visual command will go to the right but it needs to get to the left wernickers to be undrestood The right precentreal gyrus So lerft hsand will not show you because info dpes tnot get fro left that interpreytes and the right thast executes the command To do this has to be para foveal Show mw how to use what you see with the left hand?? == need interaction byw the 2 hemispheres |
|
|
A. Illustrate the 5 differences in the left and right hemispheric specialization?
B. Define these speech syndromes: 1. Agraphia 2. Alexia 3. Anarthria 4. Aphasia 5. Apraxia 6. Paraphasia |
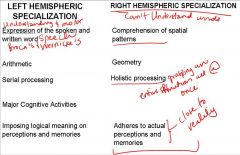
A. The 2 hemispheres are specialized
The right hand cannot draw a picture that has perspective in it The left hand can draw a perspective cause understanding of space very well Callosum lesions, the right hemisphere is good for comprehending space Arithmetic is a step by step, logical projection so it has serial not holistic so reasoning is a cognitive fxn Left fills in the spaces where they had not occurred so it makes up memories but the right hemisphere will not do this? B. 1. Agraphia = Inability to express oneself in written speech, though there is no motor paralysis or dysfunction. 2. Alexia. Inability to comprehend writing, though vision is intact. 3. Anarthria. Paralysis of the speech musculature. 4. Aphasia. Disorder in the reception or expression of languages, though sensory and motor systems are intact. 5. Apraxia. Inability to carry out motor activities following a verbal command, though motor and sensory systems are intact. 6. Paraphasia. Incorrect use of grammar ; Literal type, e.g., open the boor Semantic type e,g, the grass is blue Neologisms, e.g. new words such as "I want smurf for lunch." |
|
|
1. Describe Wernicke's receptive speech area ?
2. Describe Broca's area? |
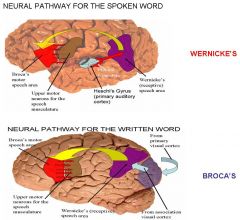
1. Wernicke's receptive speech area (see figure below) is thought to receive separate inputs from auditory (planum temporale), somatosensory and visual association areas. Discrete destruction of any of these leads to even more distinctive aphasias, as in word deafness or word blindness. The function of Wernicke's area is to decode for understanding the very complex stimuli (of the written and spoken word) sent to it from the sensory areas of the cortex for understanding. The information derived from the decoding process is forwarded to Broca's motor speech area for any language response required.
2. Broca's area, located adjacent to the part of the precentral gyrus containing the upper motor neurons of the speech musculature (lips, jaw, tongue, pharynx and larynx), programs these precentral cells in correct sequence of activation to produce meaningful speech production (speaking, writing). These upper motor neurons (i.e., corticobulbars {speaking} and corticospinals {writing}) project caudally to activate their associated motor neurons, resulting in the meaningful movements of speaking and writing). The following illustrations show the sensory to motor pathways of the brain for the processing of language stimuli. THEREFORE, Because the sensory (i.e., comprehension) aspects of language are localized in one cortical region (Wernicke's receptive speech area) and the motor (speaking, writing) aspects are localized in a second cortical region (Broca's motor speech area), discrete lesions of one or the other produce either sensory or motor aphasias. NOTES: Projection up onto the posterior parietal To wernicke's then from there by sub cortical pathway to brocas area then from brocas to the precentral gyrus because these are the upper motor neurons for the speech musculataryre cause you produce speech by talking so brocas tells all thrse neurins to produce motror function of speech! Then they projrct to the hypoglossal nucleus, nucleus ambiguus, motor nucleus of seven All the motor patyeat that innervare all the patheays of ther larynx and pharynx, buccinators…. So complete pathway for visual speech If we say write down what you saw? There will vbe axons gouing further up for the writing representation Spoken word projects to heschels that projects to planum temporale ..an auditiry assoc, cortex, then to wern’clrtts -Brocas area is ;ike a pinao player to the keys of a piano Broca is the piano player, the kets are the lower motor neurons that are produniv the motor speech so it is the programmjer of the precentral gyrus upper motor neurons |
|
|
Distinguish between:
1. ALEXIA WITHOUT AGRAPHIA (word blindness) 2. Word deafness |

1. ALEXIA WITHOUT AGRAPHIA
(word blindness) Lesion. Blockage or destruction of the left posterior cerebral artery causing destruction of the splenium of the corpus callosum and the left occupital lobe. Symptoms Right hemianopia; can understand the spoken word and can express self verbally and in writing and can write to dictation, but can't understand or repeat the written word. Mechanism. Blind in right visual field, left visual field intact but visual stimuli cannot get to dominant hemisphere for interpretation. Reading of numbers and object naming are intact because these are learned with tactile or other associations (the pathway is from right occipital cortex to the right parietal cortex then through body of corpus callosum to the left speech area). Color naming, which depends only on visual association, is lost. 2. Word Deafness Lesion. Blockage or destruction of temporal branch of left middle cerebral artery, causing destruction to the left auditory association cortex (planum temporale) and the white matter under it which carries callosal fibers from the right auditory cortex. Symptoms. Patient can read and write normally and make normal speech, but cannot understand or repeat spoken language. Mechanism. Auditory cortex has been disconnected from speech cortex. NOTES A full alexia = you cannot read anything!!! The lesion of ther left occipital lobe Its as if you were presented with a page of werneclers This is just visual, it means reading = alexia Visual goes to the right hemisphere but with corpus goes to the left side on the same level So anything on the right visual field So nothing gets to wernickes and you get alexia Agraphiac means can’t write from stored memory of words not paralysis of the muscles! So disconnection of the primary visual areas! So disconnected the visual info -Lesion of the planum temporale, disconnecting hercsls from wernickerts so this is word deafness! Block this pathway so you get word deafness! Aphasia isan inability to understant the spolken or written word through youur promary senses are inyact but its your pathways that are disconnected that cayse tge problem |
|
|
Differentiate btw:
1. Wernicke's (sensory)Aphasia 2. Broca's Motor Aphasia |
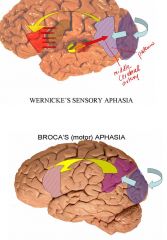
1. Wernicke's (sensory)Aphasia
Lesion. Blockage or destruction of the middle temporal branch of the left middle cerebral artery, causing destruction of posterior area 22, some adjacent inferior parietal cortex, some adjacent occipital cortex, and posterior area 20 (middle temporal gyrus). Symptoms. Fluency is normal but logorrheic and circumlocutory, while and comprehension and repetition (due to impaired comporehension) are poor. Mechanism. The area is destroyed which decoded auditory and visual patterns into meaningful language. 2. Broca's Motor Aphasia Lesion. A lesion limited to area 44, thought to be Broca's speech area, does not result in any permanent speech defects. In order to obtain the symptom picture known as Broca's aphasia, all of the cortex supplied by the upper division of the left middle cerebral artery must be destroyed. This includes frontal cortex anterior to area 44, area 44 itself, the parietal cortex posterior to area 44 (including both banks) of the central sulcus. In addition, the lesion should penetrate to the underlying white matter. Symptoms. Fluency is poor, but comprehension is normal or near normal. Repetition is poor because of poor fluency. Mechanism. Broca's area coordinates activity in the adjacent motor cortex so that the appropriate sequences of facial, oral, and respiriatory movements necessary to produce speech can be carried out. NOTES: Wern: Cut of the speech interpretation cortex so you cannot understand the written or spoken word So word blindness + word deafness It wuill be on the left side! Stroke is more on the left hemisphere and more damaging Broca In brocas, your speech is impaired which is why you cannot repear Broca is next to primary motor cortex A complete lesion gives you …you cannot speak a word |
|
|
1. Describe Conduction (repetition) Aphasia
2. Describe Global Aphasia |
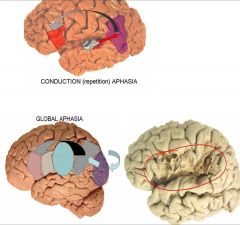
1. Conduction (repetition) Aphasia
Lesion. Blockage or destruction of the posterior and/or anterior parietal branch of the left middle cerebral artery, causing destruction of the inferior part of the supramarginal gyrus and the posterior part of the superior temporal gyrus. The lesion should extend deep into the white matter in order to sever the arcuate fasciculus. Symptoms. Fluency is normal, comprehension is normal or only moderately impaired. Repetition is very impaired, due to severance of the relay between Wernicke's and Broca's speech areas (arcuate fasciculus). Mechanism.The direct connections between Wernicke's & Broca's speech areas, by which simple verbal tasks such as repetition are carried out, are destroyed 2. Global Aphasia Lesion. Blockage or destruction of entire left middle cerebral artery, causing destruction of cortex of temporal, parietal occipital and frontal lobes. Symptoms. Total and permanent loss of language function, with complete inability to speak, write, understand speech, read repeat name, can only grunt. Mechanism All areas for understanding and producing speech have been destroyed. NOTES: Conduction: Link with broca and wrnicke so there ius destruction of the relay btw the 2 It is a short pathwat called repition They hear the word and the word has built up a nuber of associatuioins to it like the color of an apple, sound to it, oodir to it, all these associations need many sensory areas of the brain and trhids is a learning procress so when the impulses get to werniclke’s? By using these storeds images, it can slowly biuld up. In conduction you can understant the word but you cannot repat it. Global = Combination of all the aphasias |
|
|
Describe ISOLATION OF THE SPEECH AREA?
How is this related to conduction aphasia? |
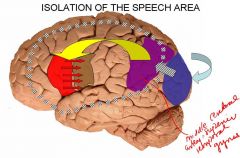
Isolation of the Speech Area
Lesion. If there is an insufficiency in all the great vessels (posterior, middle, and anterior cerebral arteries) of the left hemisphere due to severe and prolonged ischemia, hypoxia or hypoglycemia, aC-shaped infarct of the cortex which lies between the beds of the middle cerebral artery and the anterior and posterior cerebral arteries results, leaving the language area intact but isolated from the rest of the cortex. Symptoms. Patient can only repeat, echo-like, what has been spoken. There is no spontaneous speech. Mechanism. The intactness of the speech areas are necessary for speech but their presence alone is not sufficient for normal speech, which requires the rich associations that other cortical areas provide. This is related to conduction aphasia because it is the reverse of conduction aphasia and all you do is REPEAT. NOTES: Area supplied by the various cerebral artery, where they meet The peripheral vessels btw the 2 areas closed down and the cortex under them died So the whole speech apparatus is left intact but the only thing that is left in this patients is ECHOING…pathway from gersfls to planum temporale So here is the reverse of the repition aphasia = so they only REAPAT Because speech requires more than speech cortrex Requites all the associations that you have built up over many decases because you cannot draw up the asociations so you are just echoing |
|
|
Describe the role of the Corticobulbar Pattern?
|

LOOK AT PAGE 173 -BRS
NOTES Final oupt for speech is moptotr Corticobulbar projections for te speech musculature |