Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
|
What is Compartment Syndrome?
|
- elevated tissue pressure within a closed fascial space
- reduces tissue perfusion- ischemia - Results in cell death (necrosis A TRUE ORTHOPEDIC EMERGENCY |
|
|
What causes Compartment Syndrome?
|
- Decreasing compartment size (tight bandage, lying on limb)
- Increasing Compartment Content (bleeding, capillary permeability) - Fractures - Temp vascular occlusion - Burns - Exertional states - Hemophiliac - Intraosseous IV - Snake bite - Arterial Injury |
|
|
What is the most common cause of Compartment Syndrome?
|
- Fracture
- risk is proportional to degree of injury - most common in a comminuted grade III |
|
|
What is the 2nd most common cause of compartment syndrome?
|
Blunt Trauma
|
|
|
What is the muscle tissue survival rate in Compartment syndrome?
|
- Reversible at 3 to 4 hours
- Variable Damage at 6 hours - Irreversible at 8 hours |
|
|
What is the survival rate of nerves in Compartment Syndrome?
|
- Loose nerve conduction at 2 hours
- Neuropraxia at 4 hours - Irreversible changes at 8 hours |
|
|
What are the symptoms for compartment syndrome?
|
- PAIN OUT OF PROPORTION
- palpable tense compartment - pain with passive stretch - Paresthesia (later) - Paralysis (later) - Pulselessness (later) |
|
|
How is Compartment Syndrome Diagnosed?
|
- Pain and aggravation of pain by passive stretching of muscles in the compartment and palpation
- PAIN - Pressure measurement with STRYKER NEEDLE MANOMETER in all compartments (in most law suits the compartments were never measured) |
|
|
What are the differential diagnosis for compartment syndrome?
|
- Arterial occlusion
- Peripheral Nerve Injury - Muscle Rupture |
|
|
What are the 4 compartments of the lower leg?
|
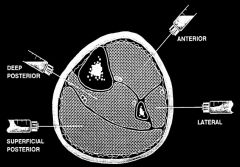
Anterior
- EHL, EDC, Tibialis Anterior, Peroneus Tertius Lateral - Peroneus longus and brevis Deep Posterior - Tibialis Posterior, FHL, FDL Superficial Posterior - Gastrocnemius, Soleus *Anterior and posterior have higher pressures |
|
|
What are the criteria for a Fasciotomy?
|
- within 30 mm Hg pressure in compartment
- Greater than 30 mm Hg do more exams first |
|
|
What is the medical management for Compartment Syndrome?
|
- Make sure patient isn't hypotensive
- Supplemental Oxygen - Remove circumferential bandages and cast (85 to 95% reduction) - Place at level of heart - Alert or Anesthesia - FASCIOTOMY - Stabilize fracture |
|
|
What is a Fasciotomy?
|
- prophylactic release of pressure before permanent damage occurs. Will not reverse damage
- safe, reliable, effective - The ONLY treatment for compartment syndrome when performed in time |
|
|
What to do in a lower leg fasciotomy?
|
Double incision
- one incision over anterior and lateral compartments - one incision behind posteromedial aspect of tibia |
|
|
What to do in a forearm Fasciotomy?
|
- Protect median nerve, brachial artery, and tendons after release
- Consider dorsal release |
|
|
What to do in a Foot Fasciotomy?
|
- Dorsal incision to release the interosseous and adductor
- Medial incision- to release the medial, superficial lateral and calcaneal compartments |
|
|
What to do in a Hand Fasciotomy?
|
- nonspecific aching of the hand with fracture or crush
- disproportionate pain - loss of MP extension and PIP flexion - Can't measure tissue pressure - 10 separate Osteofascial compartments - Dorsal Interossei (4) Palmar Interossei (3) Thenar and hypothenar (2) Adductor Pollicis (1) |
|
|
What to do in a Thigh Fasciotomy?
|
- Lateral incision to release anterior and posterior compartments
- May need Medial incision for adductor compartment |
|
|
Wound management after a Fasciotomy
|
- Bulky compression dressing and a splint
- Vacuum Assisted Closure - Foot should be placed in neutral to prevent contracture - Incision can be closed after 3 to 5 days (simple absorbent dressing and semipermeable skinlike membrane in the interim) - May need skin graft - Get complete coverage in 7 to 10 days |
|
|
Complications related to Compartment Syndrome
|
- Volkmann's Contracture
- Weak dorsiflexors - Claw toes - Sensory loss - Chronic pain - Amputation |