![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
A ______ individual is sleepy but easily aroused with stimulation. ______ describes someone who is excessively sleepy and requires vigorous stimulation but shows normal cognition once aroused. ______ refers to an individual who in addition to severe lethargy shows cognitive dysfunction. ______ refers to severe obtundation and is distinguished from coma only because the eyes open briefly. In ______, the eyes fail to open to the most vigorous stimulation. ______ usually refers to a disoriented, confused patient who fluctuates between lethargy and agitation. |
A lethargic individual is sleepy but easily aroused with stimulation. Hypersomnia describes someone who is excessively sleepy and requires vigorous stimulation but shows normal cognition once aroused. Obtundation refers to an individual who in addition to severe lethargy shows cognitive dysfunction. Stupor refers to severe obtundation and is distinguished from coma only because the eyes open briefly. In coma, the eyes fail to open to the most vigorous stimulation. Delirium usually refers to a disoriented, confused patient who fluctuates between lethargy and agitation. |
|
|
Patients in coma generally develop eye-opening and sleep-wake cycles after 2 to 4 weeks regardless of the cause of coma. A number of terms have been used to describe these patients. A patient is _____ when he has his eyes open but demonstrates no spontaneous interaction with the environment. One sees this after severe bifrontal lobe damage (lobotomy at its worst), but with vigorous stimulation, these patients answer questions correctly. If no evidence of mental activity can be elicited with vigorous stimulation, the patient may be said to show “_____ _____” or be in a “vegetative state.” The term “______” refers to the so-called “vegetative functions” of the brainstem that include maintaining sleep-wake cycles, respirations, heart rate, blood pressure and visceral autonomic regulation. A patient who appears vegetative but then shows fragments of awareness and meaningful interaction with the environment is said to be in “___ ___ ___” or MCS. Such patients may reach for objects, grunt or gesture in response to a command, visually fixate and track but are unable to do much more. It is important to realize that these conditions may not be static but can undergo transitions over time. That is typically the case when the news media reports on individuals awakening after many years spent in “coma.” |
Patients in coma generally develop eye-opening and sleep-wake cycles after 2 to 4 weeks regardless of the cause of coma. A number of terms have been used to describe these patients. A patient is abulic when he has his eyes open but demonstrates no spontaneous interaction with the environment. One sees this after severe bifrontal lobe damage (lobotomy at its worst), but with vigorous stimulation, these patients answer questions correctly. If no evidence of mental activity can be elicited with vigorous stimulation, the patient may be said to show “akinetic mutism” or be in a “vegetative state.” The term “vegetative” refers to the so-called “vegetative functions” of the brainstem that include maintaining sleep-wake cycles, respirations, heart rate, blood pressure and visceral autonomic regulation. A patient who appears vegetative but then shows fragments of awareness and meaningful interaction with the environment is said to be in “minimally conscious state” or MCS. Such patients may reach for objects, grunt or gesture in response to a command, visually fixate and track but are unable to do much more. It is important to realize that these conditions may not be static but can undergo transitions over time. That is typically the case when the news media reports on individuals awakening after many years spent in “coma.” |
|
|
One useful way to address what constitutes consciousness is to recognize that there are actually two components to consciousness. One is _____ or wakefulness and the other is the ______ of consciousness. Wakefulness is achieved by neural circuits that mediate sleep-wake cycles and involves a specific area of the upper brainstem commonly referred to as the “___ ___ system” but more accurately named the “___ ___ system.” Disruption of this system causes stupor and coma and is the primary focus of this presentation. The second component involves the content of consciousness. This refers to the cerebral activity responsible for self-awareness, cognition and purposeful interactions with the environment. These behaviors are _____ and not reflex in nature. The neural networks in the _____ drive this brain activity. Disease affecting the content of consciousness causes _____. It should be obvious that a person must be in an awake state in order to engage in any cognitive task. While the role of the cortex in maintaining consciousness seems obvious, what do we know about the brain’s arousal systems? |
One useful way to address what constitutes consciousness is to recognize that there are actually two components to consciousness. One is arousal or wakefulness and the other is the content of consciousness. Wakefulness is achieved by neural circuits that mediate sleep-wake cycles and involves a specific area of the upper brainstem commonly referred to as the “reticular activating system” but more accurately named the “ascending arousal system.” Disruption of this system causes stupor and coma and is the primary focus of this presentation. The second component involves the content of consciousness. This refers to the cerebral activity responsible for self-awareness, cognition and purposeful interactions with the environment. These behaviors are premeditated and not reflex in nature. The neural networks in the cortex drive this brain activity. Disease affecting the content of consciousness causes dementia. It should be obvious that a person must be in an awake state in order to engage in any cognitive task. While the role of the cortex in maintaining consciousness seems obvious, what do we know about the brain’s arousal systems? |
|
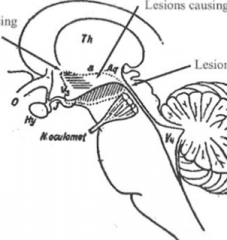
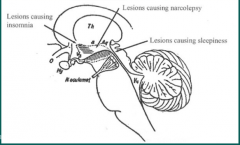
Identify lesions causing insomnia, lesions causing narcolepsy, and lesions causing sleepiness:
|
|
|
|
In the last century, the anatomy of consciousness became better defined through the work of Baron Constantine von Economo. In 1916, von Economo noticed cases of a new and not previously described typeofencephalitisthatcauseda“sleeping sickness”he termed ________. This disease became a world-wide epidemic that did not subside until a decade later. This epidemic should not be confused with the huge influenza pandemic of 1918 that killed millions and whose recombinantprogenyH1N1hasrecentlythreatenedtheworld. TheviruscausingVonEconomo's encephalitis lethargica has never been identified. What did the sleeping sickness look like? Individuals slept for 20 hours a day, awakening only to eat or go to the toilet. Some patients died, and von Economo's post-mortem studies revealed lesions in the_________ and __________. Some patients with encephalitis would sleep at most only a few hours a day and had lesions in the rostral hypothalamus. Among the survivors, there was a recovery phase several months after the acute encephalitis when some patients developed sleep attacks and cataplexy. ________ referstothesuddeninvoluntarylossofmuscletoneduringemotional excitement,suchasintenselaughter,causingtheindividualtofalldown. Thesepatientshadwhatwe now call “__________.” These patients died later from other causes and were found to have lesions in the posterior lateral hypothalamus lying between a sleep promoting area in the rostral hypothalamus and a wakefulness promoting area in the upper midbrain. Further research has identified the sleep promoting area as the _____________, whose destruction causes profound insomnia. Narcolepsy is caused by a loss of neurons that can be histochemically stained with antibodies against the neuro-peptide neurotransmitter “_______”. The upper brainstem area promoting arousal consists of multiple nuclei and pathways that will be described later. Many of the long term survivors of von Economo's encephalitis went onto develop a post-encephalitic Parkinsonism syndrome to which von Economo's name has been linked. But we will not be discussing that. |
In the last century, the anatomy of consciousness became better defined through the work of Baron Constantine von Economo. In 1916, von Economo noticed cases of a new and not previously described typeofencephalitisthatcauseda“sleepingsickness”hetermedencephalitislethargica. This disease became a world-wide epidemic that did not subside until a decade later. This epidemic should not be confused with the huge influenza pandemic of 1918 that killed millions and whose recombinantprogenyH1N1hasrecentlythreatenedtheworld. TheviruscausingVonEconomo's encephalitis lethargica has never been identified. What did the sleeping sickness look like? Individuals slept for 20 hours a day, awakening only to eat or go to the toilet. Some patients died, and von Economo's post-mortem studies revealed lesions in the rostral periaqueductal grey matter and posterior 3rd ventricle. Some patients with encephalitis would sleep at most only a few hours a day and had lesions in the rostral hypothalamus. Among the survivors, there was a recovery phase several months after the acute encephalitis when some patients developed sleep attacks and cataplexy. Cataplexyreferstothesuddeninvoluntarylossofmuscletoneduringemotional excitement,suchasintenselaughter,causingtheindividualtofalldown. Thesepatientshadwhatwe now call “narcolepsy.” These patients died later from other causes and were found to have lesions in the posterior lateral hypothalamus lying between a sleep promoting area in the rostral hypothalamus and a wakefulness promoting area in the upper midbrain. Further research has identified the sleep promoting area as the ventrolateral preoptic nucleus, whose destruction causes profound insomnia. Narcolepsy is caused by a loss of neurons that can be histochemically stained with antibodies against the neuro-peptide neurotransmitter “orexin”. The upper brainstem area promoting arousal consists of multiple nuclei and pathways that will be described later. Many of the long term survivors of von Economo's encephalitis went onto develop a post-encephalitic Parkinsonism syndrome to which von Economo's name has been linked. But we will not be discussing that. |
|
|
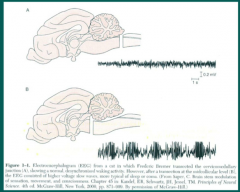
a brainstem transection at the level of the cervical medulla caused _____ and respiratory arrest requiring mechanical ventilation. While these motionless animals appeared unconsciousness, the EEG showed a “_______” brain wave pattern characteristic for the awake state. Successive lesions marching upwards (rostrally) toward the midbrain produced the same effect until a cut was made at the level of the ______ (quadrigeminal plate). At this level, the EEG became “synchronized” showing high voltage slow waves typical of thepatternseeninsleepandinsomepatientswithcoma. Inotherwords, lesions of the brainstem did not affect wakefulness, as defined by the EEG pattern, until the lesion reached the upper pontine and midbrain level. This supported von Economo’s contention that an arousal center in the midbrain had been damaged by “encephalitis lethargica.” |
a brainstem transection at the level of the cervical medulla caused quadriplegia and respiratory arrest requiring mechanical ventilation. While these motionless animals appeared unconsciousness, the EEG showed a “desynchronized” brain wave pattern characteristic for the awake state. Successive lesions marching upwards (rostrally) toward the midbrain produced the same effect until a cut was made at the level of the posterior colliculi (quadrigeminal plate). At this level, the EEG became “synchronized” showing high voltage slow waves typical of thepatternseeninsleepandinsomepatientswithcoma. Inotherwords, lesions of the brainstem did not affect wakefulness, as defined by the EEG pattern, until the lesion reached the upper pontine and midbrain level. This supported von Economo’s contention that an arousal center in the midbrain had been damaged by “encephalitis lethargica.” |
|
|
|
|
|
Where some some primary lesions that cause coma located? |
|
|
|
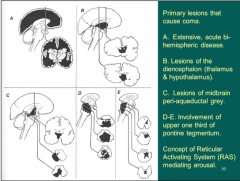
Since the 1930s, a number of neuropathological patterns have been associated with coma. The first, represented by A, involves severe sudden bilateral hemispheric disease. It is unusual, however, to have such an extensive global insult without affecting the upper brainstem as well. The other pictures, B through E, are notable for involving some region of the upper brainstem but always including “_______” whether found in the thalamus, hypothalamus, mid-brain peri-aqueductal grey or upper third of the pons. What is not shown is that often, the damage to these regions are often secondary to a ______ syndrome affecting one or both cerebral hemispheres. You will hear more about that shortly. In any event, people noticed that the reticular grey formation was affected and that led to the concept of the “_______” as mediating arousal. |
Since the 1930s, a number of neuropathological patterns have been associated with coma. The first, represented by A, involves severe sudden bilateral hemispheric disease. It is unusual, however, to have such an extensive global insult without affecting the upper brainstem as well. The other pictures, B through E, are notable for involving some region of the upper brainstem but always including “reticular grey formation” whether found in the thalamus, hypothalamus, mid-brain peri-aqueductal grey or upper third of the pons. What is not shown is that often, the damage to these regions are often secondary to a herniation syndrome affecting one or both cerebral hemispheres. You will hear more about that shortly. In any event, people noticed that the reticular grey formation was affected and that led to the concept of the “reticular activating system” as mediating arousal. |
|
|
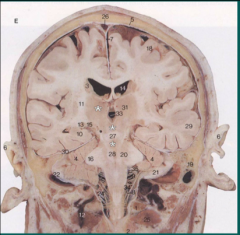
What is the “reticular grey formation”? Among the _____ nerve nuclei and other clearly demarcated cell groups in the brainstem, anatomists had found diffuse aggregations of neurons of different types and sizes, separated by a wealth of fibers traveling in all directions. When stained to visualize the neuronal processes, a net-like or _____ pattern emerged as shown in this photomicrograph of a section stained to show fibers (____) and cell bodies. The term “reticular formation” was born. What does it do? It was known that sensory pathways on their way to the thalamus would often send a collateral axon to synapse in the reticular formation. It seemed reasonable that sudden major sensory changes might well benefit from a heightened alertness before the sensory information ever got processed by the parietal cortex. A startle response to a sudden noise behind you, or a movement in a nearby brush, or an unexpected nudge to your side, whatever, might mean thedifferencebetweenlifeanddeathinevolutionaryterms. Itturnsout, however, that the reticular formation does much more, and furthermore, it is not a diffuse, undifferentiated structure but quite the contrary. Cytoarchitectonic differences exist between different areas of the reticular formation and the various cell groups have highly specific connections. |
What is the “reticular grey formation”? Among the cranial nerve nuclei and other clearly demarcated cell groups in the brainstem, anatomists had found diffuse aggregations of neurons of different types and sizes, separated by a wealth of fibers traveling in all directions. When stained to visualize the neuronal processes, a net-like or reticular pattern emerged as shown in this photomicrograph of a section stained to show fibers (myelin) and cell bodies. The term “reticular formation” was born. What does it do? It was known that sensory pathways on their way to the thalamus would often send a collateral axon to synapse in the reticular formation. It seemed reasonable that sudden major sensory changes might well benefit from a heightened alertness before the sensory information ever got processed by the parietal cortex. A startle response to a sudden noise behind you, or a movement in a nearby brush, or an unexpected nudge to your side, whatever, might mean thedifferencebetweenlifeanddeathinevolutionaryterms. Itturnsout, however, that the reticular formation does much more, and furthermore, it is not a diffuse, undifferentiated structure but quite the contrary. Cytoarchitectonic differences exist between different areas of the reticular formation and the various cell groups have highly specific connections. |
|
|
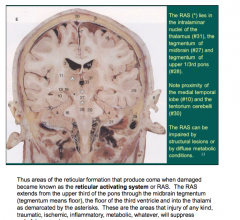
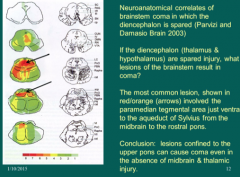
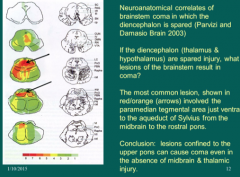
What is the minimal amount of reticular formation that can be damaged in the upper brainstem and still produce coma? Working at the Mayo Clinic, Parvizi and Damasio performed a combined MRI neuropathological study of comatose individuals with brainstem injury in whom the _____ (that is the thalamus and hypothalamus) and most of the midbrain were spared. In other words they excluded patients with so-called “top of the basilar” stroke. Among 9 patients, the most common lesion site is shown in red and orange. It is the_____ area just ventral to the aqueduct of Sylvius from the midbrain to the rostral pons. This study suggests that lesions confined to the _____ can cause coma in the absence of midbrain and thalamic injury. This explains why some patients with pontine hemorrhage are comatose. Lesions below the rostral pons disrupt the_____ and corticobulbar tracts bilaterally to leave a patient quadriplegic with a paralyzed lower face, unable to speak, swallow or breathe on his own, yet the patient is conscious, aware, can see and hear, and usually retain some control over vertical eye movements and blinking through which he can communicatewiththeoutsideworld. Thusotherpatientswithslightlymore _____ pontine hemorrhage appear to be in coma but are actually awake and “locked-in”. From a humane aspect, it is essential to make a correct diagnosis and to treat locked-in patients at the bedside as fully conscious and mentally competent individuals. |
What is the minimal amount of reticular formation that can be damaged in the upper brainstem and still produce coma? Working at the Mayo Clinic, Parvizi and Damasio performed a combined MRI neuropathological study of comatose individuals with brainstem injury in whom the diencephalon (that is the thalamus and hypothalamus) and most of the midbrain were spared. In other words they excluded patients with so-called “top of the basilar” stroke. Among 9 patients, the most common lesion site is shown in red and orange. It is the paramedian tegmental area just ventral to the aqueduct of Sylvius from the midbrain to the rostral pons. This study suggests that lesions confined to the upper pons can cause coma in the absence of midbrain and thalamic injury. This explains why some patients with pontine hemorrhage are comatose. Lesions below the rostral pons disrupt the corticospinal and corticobulbar tracts bilaterally to leave a patient quadriplegic with a paralyzed lower face, unable to speak, swallow or breathe on his own, yet the patient is conscious, aware, can see and hear, and usually retain some control over vertical eye movements and blinking through which he can communicatewiththeoutsideworld. Thusotherpatientswithslightlymorecaudal pontine hemorrhage appear to be in coma but are actually awake and “locked-in”. From a humane aspect, it is essential to make a correct diagnosis and to treat locked-in patients at the bedside as fully conscious and mentally competent individuals. |
|
Identify RAS |
|
|
|
|
|
|
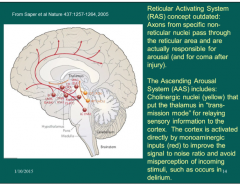
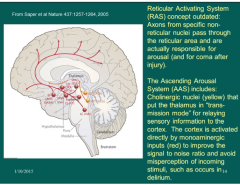
The concept of the reticular activating system or RAS underlying arousal is ingrained in medical jargon. Work by Cliff Saper and others, however, has shown that reticular nuclei are not the source of arousal. Damage to these areas destroys axons from specific nearby nuclei that pass through the RAS territory. The nuclei shown in red and yellow are the ones actually responsible for arousal and are more accurately identified as the ______. In yellow, two cholinergic nuclei project to the thalamic relay nuclei and inhibit their firing. This inhibition increases wakefulness and places the thalamus “in transmission” mode for filtering and relaying sensory information to the cortex. Without this inhibition, the thalamic relay neurons spontaneously continue their periodic electrical “bursting” and with their widespread connections to the cortex, these thalamic relay neurons synchronize cortical electrical activity and induce sleep. The monoaminergic systems shown in red also have widespread connections to the cortex, both direct and indirect Their role is to improve the signal to noise ratio for messages from the thalamus and thereby prevent any misperception of incoming sensory stimuli. When this system fails, sensory hallucinations and confusion result, causing delirium. Note that different neurotransmitters are responsible for the normal maintenance of consciousness and perturbations in any of them can lead to delirium. Knowledge of these transmitters also offers potential therapeutic targets in the treatment of delirium. |
The concept of the reticular activating system or RAS underlying arousal is ingrained in medical jargon. Work by Cliff Saper and others, however, has shown that reticular nuclei are not the source of arousal. Damage to these areas destroys axons from specific nearby nuclei that pass through the RAS territory. The nuclei shown in red and yellow are the ones actually responsible for arousal and are more accurately identified as the ascending arousal system. In yellow, two cholinergic nuclei project to the thalamic relay nuclei and inhibit their firing. This inhibition increases wakefulness and places the thalamus “in transmission” mode for filtering and relaying sensory information to the cortex. Without this inhibition, the thalamic relay neurons spontaneously continue their periodic electrical “bursting” and with their widespread connections to the cortex, these thalamic relay neurons synchronize cortical electrical activity and induce sleep. The monoaminergic systems shown in red also have widespread connections to the cortex, both direct and indirect Their role is to improve the signal to noise ratio for messages from the thalamus and thereby prevent any misperception of incoming sensory stimuli. When this system fails, sensory hallucinations and confusion result, causing delirium. Note that different neurotransmitters are responsible for the normal maintenance of consciousness and perturbations in any of them can lead to delirium. Knowledge of these transmitters also offers potential therapeutic targets in the treatment of delirium. |
|
|
|
|
|
|
|
|
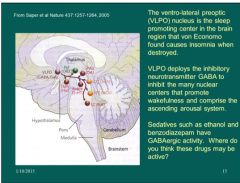
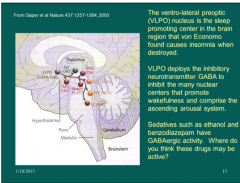
The _______ or VLPO is the sleep promoting center that von Economo found causes insomnia when destroyed. VLPO uses the inhibitory neurotransmitter _____ and an inhibitory neuropeptide, galanin, to inhibit the many centers that promote wakefulness in the ascending arousal system. Ethanol, benzodiazepines and other drugs that have GABA-like properties in the brain induce sedation in part by promoting the inhibitory effects of the VLPO on the _______ system. Notice that one nucleus, the VLPO, singlehandedly counterbalances the influence of multiple arousal nuclei to promote sleep. |
The ventro-lateral preoptic nucleus or VLPO is the sleep promoting center that von Economo found causes insomnia when destroyed. VLPO uses the inhibitory neurotransmitter gamma amino butyric acid or GABA and an inhibitory neuropeptide, galanin, to inhibit the many centers that promote wakefulness in the ascending arousal system. Ethanol, benzodiazepines and other drugs that have GABA-like properties in the brain induce sedation in part by promoting the inhibitory effects of the VLPO on the ascending arousal system. Notice that one nucleus, the VLPO, singlehandedly counterbalances the influence of multiple arousal nuclei to promote sleep. |
|
|
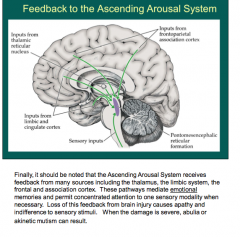
Where does the ascending arousal system receive feedback from?
What do these pathways mediate?
What does loss of this feedback cause? |
|
|
|
What are two major causes of coma? What are components of each one of the major causes?
What should you always rule out first? |

|
|
|
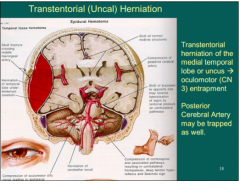
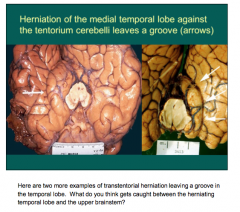
What does a transtentorial herniation of the medial temporal lobe lead to? What vessel may be trapped as well? |
|
|
|
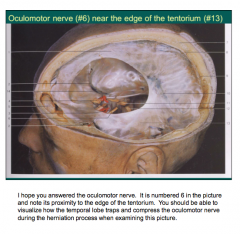
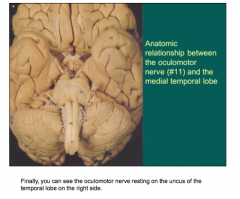
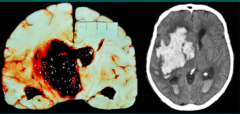
A 30 year old man is assaulted and struck on the right head with a bat. Theresultingskullfracturelaceratesthemiddlemeningealarterywhichproducesan epidural hematoma as shown in the picture. The mass effect pushes the right temporal lobe medially and down across the tentorium cerebelli. This is called transtentorial herniation of the medial temporal lobe or the uncus of the temporal lobe. Another term is uncal herniation. The terminology is less important than the key anatomical teaching point, namely that the oculomotor nerve lies between the herniating uncus and the midbrain and diencephalon. It is therefore compressed first, before pressure on the midbrain and diencephalon produce ischemia and cause increasing lethargy, stupor and coma. Infactthenervefasciclemediatingpupillaryconstrictionliessuperficiallyandmaybe thefirstpartoftheoculomotornervetobecompressed. Atthebedside,therightpupil becomes widened and slower to react to direct and indirect light compared to the left side. This pupillary abnormality may precede the ptosis and weakness of ocular movement causedbyocularmotornerveparesis. Itoftenprecedestheincreasedlethargyandthe developmentofcontralateralhemiparesisandacontralateralBabinskisign. Whileitisnot shown well here, the posterior cerebral artery can be trapped against the cerebellar tentorium as well to cause ipsilateral ischemia and stroke in the occipital lobe. This is a structural and neurosurgical emergency, and the key teaching point is that an early loss of pupil reactivity to light should signal the possibility of imminent herniation, of raised intracranial pressure and impending catastrophe if emergency steps to reduce intracranial pressure are not taken immediately and surgery is not performed in a timely fashion. |
A 30 year old man is assaulted and struck on the right head with a bat. Theresultingskullfracturelaceratesthemiddlemeningealarterywhichproducesan epidural hematoma as shown in the picture. The mass effect pushes the right temporal lobe medially and down across the tentorium cerebelli. This is called transtentorial herniation of the medial temporal lobe or the uncus of the temporal lobe. Another term is uncal herniation. The terminology is less important than the key anatomical teaching point, namely that the oculomotor nerve lies between the herniating uncus and the midbrain and diencephalon. It is therefore compressed first, before pressure on the midbrain and diencephalon produce ischemia and cause increasing lethargy, stupor and coma. Infactthenervefasciclemediatingpupillaryconstrictionliessuperficiallyandmaybe thefirstpartoftheoculomotornervetobecompressed. Atthebedside,therightpupil becomes widened and slower to react to direct and indirect light compared to the left side. This pupillary abnormality may precede the ptosis and weakness of ocular movement causedbyocularmotornerveparesis. Itoftenprecedestheincreasedlethargyandthe developmentofcontralateralhemiparesisandacontralateralBabinskisign. Whileitisnot shown well here, the posterior cerebral artery can be trapped against the cerebellar tentorium as well to cause ipsilateral ischemia and stroke in the occipital lobe. This is a structural and neurosurgical emergency, and the key teaching point is that an early loss of pupil reactivity to light should signal the possibility of imminent herniation, of raised intracranial pressure and impending catastrophe if emergency steps to reduce intracranial pressure are not taken immediately and surgery is not performed in a timely fashion. |
|

What is causing the herniation?
|

|
|
What caused the groove here? |
|
|
|
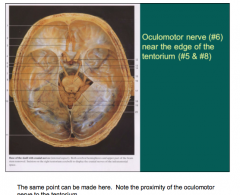
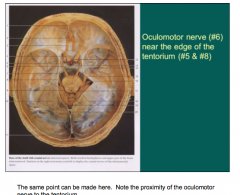
What nerve has close proximity to the edge of the tentorium? |
|
|
|
|
|
|
What is the relationship between the oculomotor nerve and the medial temporal lobe? |
|
|
|
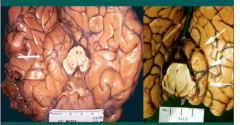
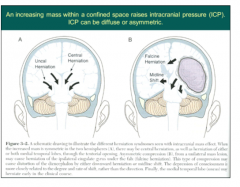
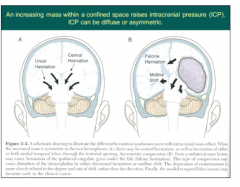
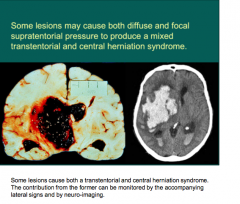
This slide shows an uncal herniation that is unilateral. It also shows that the herniation can involve both hemispheres. The latter can occur when trauma produces bilateral _____hematomas or the hemispheres are severely and irreversibly damaged by certain metabolic insults such as ____ or the cerebral edema that accompanies fulminant liver failure or hydrocephalus. Under such circumstances, there is diffuse and symmetric pressure on the brain both medial and downward to produce _____ herniation. Another type of herniation involves a mass effect that pushes the brain under the falx cerebri. This _____ herniation sometimes traps and compresses one or both anterior cerebral arteries against the falx to cause ischemic stroke in the parasagittal cortex on one or both sides. |
This slide shows an uncal herniation that is unilateral. It also shows that the herniation can involve both hemispheres. The latter can occur when trauma produces bilateral subdural hematomas or the hemispheres are severely and irreversibly damaged by certain metabolic insults such as hypoxia or the cerebral edema that accompanies fulminant liver failure or hydrocephalus. Under such circumstances, there is diffuse and symmetric pressure on the brain both medial and downward to produce central herniation. Another type of herniation involves a mass effect that pushes the brain under the falx cerebri. This falcine herniation sometimes traps and compresses one or both anterior cerebral arteries against the falx to cause ischemic stroke in the parasagittal cortex on one or both sides. |
|
|
|
|
What does this describe? |
Central herniation |
|
|
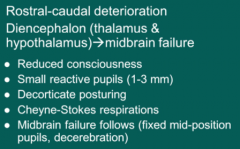
How does one recognize central herniation at the bedside? There is a steady progressive failure of the brainstem in a rostral to caudal direction. It starts with increasing lethargy due to early pressure on the reticular grey in both thalami. The hypothalamus comes under pressure and the central sympathetic tracts originating in the hypothalamus are compromised leading to small but still reactive pupils. They are small due to the unopposed cholinergic activity mediated by the Edinger-Westphal nuclei. Later, when the pressure extends to the midbrain, the Edinger-Westphal nuclei fail. Constrictive pupillary tone is lost and the pupils become fixed in mid- position. Decorticate or flexor posturing is followed by _____ or extensor posturing and is a late sign of herniation. This posturing will be described and explained later. _____ respirations, characterized by apneic spells interspersed with hyperventilation periods, also provide an early warning of herniation. |
How does one recognize central herniation at the bedside? There is a steady progressive failure of the brainstem in a rostral to caudal direction. It starts with increasing lethargy due to early pressure on the reticular grey in both thalami. The hypothalamus comes under pressure and the central sympathetic tracts originating in the hypothalamus are compromised leading to small but still reactive pupils. They are small due to the unopposed cholinergic activity mediated by the Edinger-Westphal nuclei. Later, when the pressure extends to the midbrain, the Edinger-Westphal nuclei fail. Constrictive pupillary tone is lost and the pupils become fixed in mid- position. Decorticate or flexor posturing is followed by decerebrate or extensor posturing and is a late sign of herniation. This posturing will be described and explained later. Cheyne-Stokes respirations, characterized by apneic spells interspersed with hyperventilation periods, also provide an early warning of herniation. |
|
What is happening here? |
|
|
|
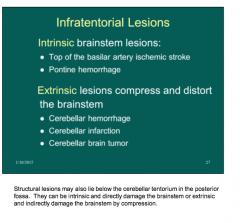
Two causes of intrinsic brainstem lesions: Three causes of extrinsic lesions? |
|
|
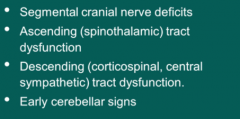
How do you clinically identify a lesion lying in the brainstem? |
|
|
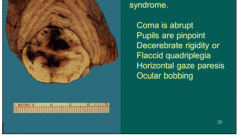
A 45 year old crack cocaine user suddenly becomes unconscious and displays a flaccid quadriplegia. The eyes show 1 mm pinpoint pupils that do react to bright light when observed with a magnifying glass. There is complete paralysis of horizontal gaze. The eyes can move in the vertical plane and at times show bobbing up and down movements. This is a classic example of a pontine hemorrhage that caused coma because the upper one- third pontine tegmentum was disrupted. The vertical gaze center in the midbrain, along with cranial nerves 3 and 4 are intact and permit eye movements in the vertical plane. When this patient awakens, he is at risk for what syndrome? |
Pontine hemorrhage:
Locked-in syndrome |
|
|
What may non-cerebral disease interfere with metabolism of?
What are toxins in uremia and hepatic failure? Toxins in drug overdose poisons and sepsis?
|
|
|
|
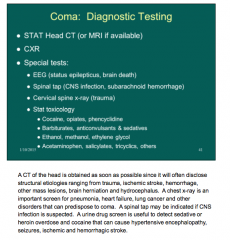
Metabolic encephalopathy: How does neuro-exam present? Head CT? |
Read notes on page |
|
What are all of these causes of? |
Metabolic encephalopathy * = common in elderly |
|
|
What is dextrose 50 always preceded by? |
|
|
|
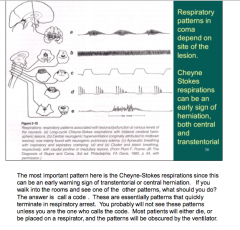
What do you see here? What is it an early sign of? |
|
|
|
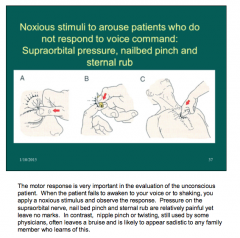
What do you do to arouse patients who do not respond to voice command? |
|
|
|
What was developed for prognosis in head trauma? What is the flexor response due to? How does the extensor response arise? |
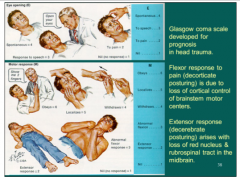
Read notes on page |
|
|
What is an excellent GCS? What is a very poor GCS? |

|
|
|
What do you do STAT if suspicion of coma?
|
|
|
What are all of these? |
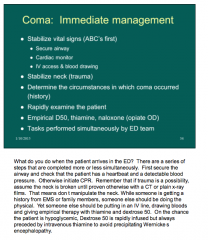
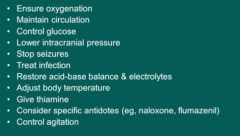
Treatment for coma |
|
|
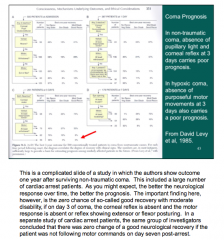
What carries a poor prognosis in non-traumatic coma? In hypoxic coma? |
|
|
|
Read through cases in presentation. |
Read through cases. |