Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
116 Cards in this Set
- Front
- Back
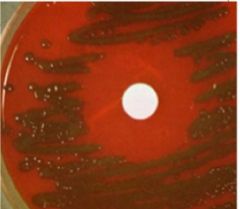
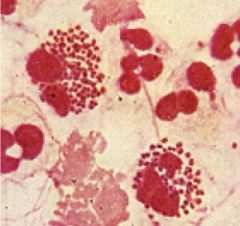
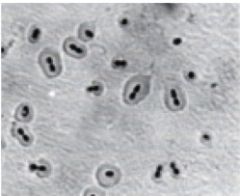
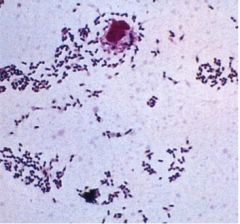
What bug that causes meningitis is pictured? What media is shown and what type of growth is seen?
|
Streptococcus Pneumoniae
G(+) cocci in pairs or chains α-hemolytic on blood agar optochin sensitive (circle in middle) bacitracin resistant |
|
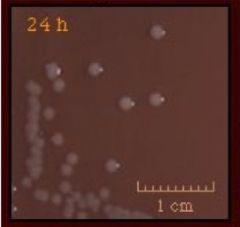
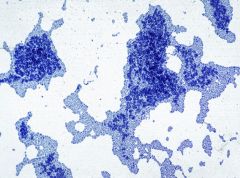
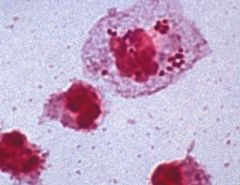
What bug that causes meningitis is pictured? What media is shown and what type of growth is seen?
|
Neisseria meningitidis
G(-) diplococci (grows w/in PMNs) • Growth on blood agar • Thayer-Martin agar (modified/selective chocolate agar) • Optimal growth with 5% CO2 |
|
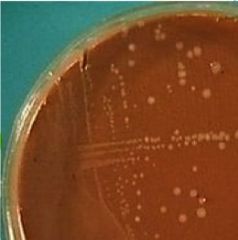
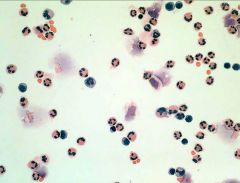
What bug that causes meningitis is pictured? What media is shown and what type of growth is seen?
|
Haemophilus influenzae type b
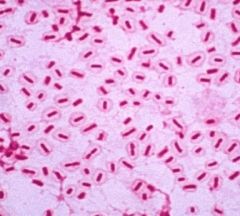
WBC + G(-) coccobacilli or rods Growth on chocolate agar - provides both X & V factors |
|
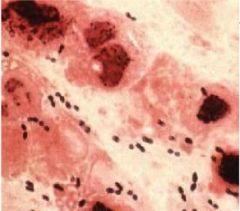
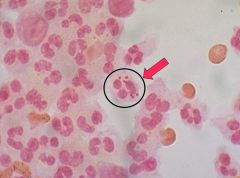
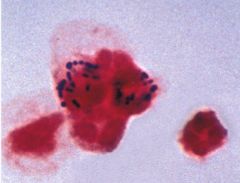
What bug that causes meningitis is shown? (as G(+) cocci in pairs?)
|
Streptococcus pneumoniae
|
|
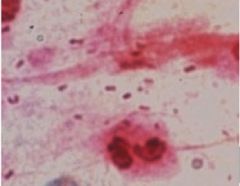
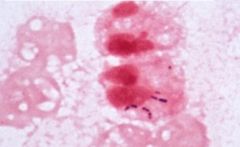
What G(-) diplococci that causes meningitis is shown growing w/in PMNs?
|
Neisseria meningitdis
|
|
What G(+) coccobacilli or rods that cause meningitis are shown growing in WBCs?
|
Haemophilus influenzae type-B
|
|
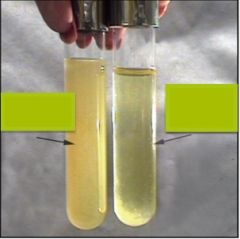
What lab test is shown? Which meningitis bug will test (+)? Which tube would that be?
|
Bile solubility test.
Streptococcus pneumoniae Tube on the right (clearer tube shows that S. pneumoniae is bile soluble) |
|
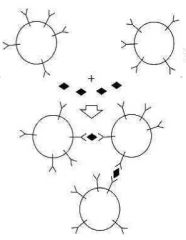
What test is shown? What is it used for?
|
Latex particle agglutination test
• Used to identify capsular antigens in the CSF |
|
What reaction is being shown? How can it be used?
|
The Quellung reaction is a biochemical reaction in which antibodies bind to the Bacterial capsule of Streptococcus pneumoniae, Klebsiella pneumoniae, Neisseria meningitidis and Haemophilus influenzae and thus allow them to be visualized under a microscope. If the reaction is positive, the capsule becomes opaque and appears to enlarge.
It can be used for identifying pneumococcal polysaccharide capsule antigens t has been used to identify the 90 known capsular serotypes of Streptococcus pneumoniae |
|
What is shown?
|
Bacteria in the CSF in purulent meningitis
|
|
What is shown?
|
CSF in Acute bacterial meningitis
|
|
What is shown?
|
G(-) intracellular diplococci
(in otherwords, Neisseria meningitidis) |
|

What is shown in 1? What cells in what space? What disease process?
|
• Vessel
• PMNs in perivascular Virchow-Robin space • Acute supportative meningitis |
|
What is shown? What is the causative agent?
|
Meningiitis
• Klebsiella pneumniae • G(-) large rods with thick mucoid capsule |
|
What is shown?
|
Listeria monocytogenes
• G(+) rods • Cause transplacental infxn in the neonate • Bugs are phagocytosed by PMNs |
|
What is shown? What bug?
|
Stretococcus agalactiae
• Causes neonatal meningitis • G(+) cocci in normal vaginal flora • Phagocytosed by PMNs |
|
What is shown?
|
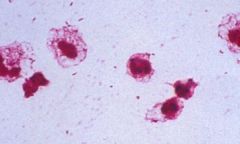
Haemophilus influenzae
• causes neonatal meningitis • G(-) short rods • Mostly extracellularly located |
|
What is shown?
|
Streptococcus pneumoniae
• Causes fulminant meningitis • G(+) cocci (in pairs or chains) • Mostly extracellular |
|
What it shown?
|
Neisseria Meningitidis
• G(-) dipplococcus • Causes fulminant meningitis • Intracellularly located |
|
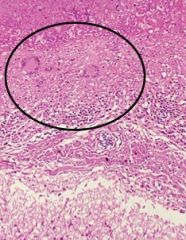
What is shown? What kind of necrosis? What specific cells?
|
TB Meningitis
• Caseous necrosis • Epitheliod cells & Langerhands Type Giant cells |
|
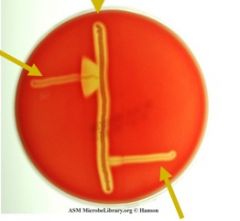
What test is shown? What is unique about this test?
What strain is shown at 9 o'clock? 12? 4 o'clock? |
CAMP test
• GBS produces a diffusible heat-stable protein (CAMP factor) that enhances B-hemolysis of staphylococcus aureus • 9: Streptococcus agalactiae • 12: Staphylococcus aureus • 4: Stapylococcus pyogenes |
|
|
Front
|
Back of Flashcard (Answer)
|
|
|
What are the most common causes of bacterial meningitis in neonates? Children/young adults? Adults?
|
• Neonates: 1. Group B strep 2. Escherichia coli
• Children & young adults: 1. Neisseria meningitidis 2. Streptococcus pneumoniae 3. Group B streptococus 4. Haemophilus influenzae (consider if not vaccinated) • Adults: 1. Streptococcus pneumoniae 2. Neisseria meningitidis 3. Haemophilus influenzae *Consider listeria monocytogenes in all populations* |
|
|
This meningitis-causing bug is gram (+) cocci & lancet shaped. What population does it prefernetially affect?
|
Streptococcus pneumoniae.
Most common in adults (second most common cause in young adults) |
|
|
Streptococcus pneumonia appears in which formation and will appear as __ on blood agar. What is its main virulence factor?
|
• Appears in chains or as diplococci and is α-hemolytic on blood agar.
• Main virulence factor is polysaccharide capsule. |
|
|
This meningitis-causing bug is gram (-) diplococci. What population does it preferentially affect?
|
Neisseria meningitidis
Most common in children and young adults (2nd in adults) |
|
|
What is the main virulence facotr of neisseria meningitidis? How does it appear on gram stain?
|
• Polysaccharide capsule is the main virulence factor of neisseria meningitidis
• G(-) dipploccci |
|
|
This meningitis-causing bug is gram (-) coccoabacilli. What population does it preferentially affect?
|
Haemophilus influenzae type-B
Affects people who have not had their Hib vaccines |
|
|
What are the main virulence factors of Haemophilus influenzae type-B? How does it appear on gram stain?
|
• Capsule serovar b (Hib), pili, IgA protease (mucosal colonization), endotoxin (LPS)
•G(-) coccobacilli |
|
|
What are the virulence factors associated with streptococcus pneumonia meningitis? What is the disease progression?
|
• Polysaccharide capsule (antiphagocytic)
• IgA protease (facillitaets colonization) • Pneumolysin (pore-forming toxin) • Teichoic acid (peptidoglycan fragment --> inflammation) • Colonization of nasopharynx --> lung/eustacian tube infxn --> pneumonia/otitis media --> bacteremia/meningitis |
|
|
What pathogen causes meningitis by an initial URI, attachment to receptors on non-ciliated cells of the nasopharynx via pili, colonization w/ IgA protease, kills host cells by repicating & migrating to the subepithelial spaces, invasion into the blood stream and then into the brain. What prevents phagocytosis of this bug?
|
• Neisseria meningitidis (meningococcal meningitis) prevents phagocytosis via polysaccharide capsule
|
|
|
What is a complication of neisseria meningitidis infxn? How is it mediated?
|
Diffuse vascular damage/ DIC caused by endotoxins (LPS and LOS (lipooligosaccharides)
Can appear as petechiae or purpura |
|
|
Where is meningococcal menigitis often seen?
|
• University dorms, military barracks (crowded conditions)
• Endemic in the meningitis belt across sub-sahara Africa |
|
|
What pathogen causes meningitis by initial colonization of the nasopharynx --> invasion into deeper tissues (goes between epithelial cells) --> bacteremia --> spread to the CNS?
|
Haemophilus influenzae type-B
Affects people who have not had their Hib vaccines |
|
|
What meningitis causing pathogen has the following virulence factors: polysaccharide capsule (poly-ribitol-phosphate), pili, IgA protease (mucosal colonization), endotoxin (LPS)
|
Haemophilus influenzae type-B (type-B is after the type of polysaccharide capsule)
|
|
|
What meningitis causing pathogen is bile soluble and can be identified using the Quellung reaction?
|
Streptococcus pneumoniae.
G(+) cocci in pair Most common in adults (second most common cause in young adults) |
|
|
What type of meningitis will present like this:
• Gradual onset over a few weeks • Starts with malaise, apathy, and anorexia • Then photophobia, neck stiffness, impairment of consciousness • Serious complications & sequelae (including brain abscesses) |
Tuberculous meningitis
|
|
|
To prevent bacterial meningitis from this bug there is a 7-valent conjugate vaccine (for infants and children) and a 23 valent polysaccaharide vaccine
|
Pneumococcal meningitis
Streptococcus pneumoniae |
|
|
To prevent bacterial meningitis from this bug there is a MPSV4 (polysaccharride vaccine) for adults and a MCV4 (conjugate vaccine) for children. What serogroups do these vaccines protect against?
|
Meningococcal meningitis
Neisseria meningitidis • Protects against A, C, γ, and W-135 (not against B) |
|
|
What is used as antimicrobial chemoprphylaxis for close contacts of people with meningitis?
|
Rifampin
|
|
|
What meningitis-causing bugs can be transmitted during delivery?
|
• Streptococcus agalactiae (GBS)
• Escherichia coli |
|
|
What are the virulence factors of Strepococcus agalactiae?
|
• Polysaccharide capsule
• Peptidase (inactivates C5a, a chemoattractant of PMNs) • Hydrolytic enzymes (tissue destruction & systemic spread) |
|
|
What are the virulence factors of Escherichia coli?
|
• Strains containing the K1 polysaccharide capsule
• Pili • Cytotoxins • LPS |
|
|
What meningitis causing pathogen is a small G(+) rod that is β-hemolytic?
|
• Listeria monocytogenes
|
|
|
What are the characterisitcs of listeria monocytogenes growth? Why is this relevant to its spread?
|
• Non-spore forming, facultative intracellular anaerobes
**Broad temperature range of gowth 1ºC to 45º C** *Motile at 25ºC* and non-motile at 37º • Spread via the ingestion of contaminated food. |
|
|
What pathogen can be transmitted across the placenta during pregnancy and can result in meningitis?
|
Listeria monocytogenes
|
|
|
What pathogen grows inside macrophages and epithelial cells (thus avoiding the immune system)? How is it able to spread from cell to cell?
|
• Listeria monocytogenes (Facultative intracellular pathogen)
1. Internalins (attachment & entry into non-phagocytic cell) 2. --> Listeriolysion O (LLO: pore-forming exotoxin; escape from a vacuole of phagolysosome & release into the cytosol 3. --> ActA (surface protein - actin polymerisation --> motile comet tails which propels it out of the cell) |
|
|
What pathogen can cause early-onset sepsis "granulomatosis infantiseptica" in neonates?
|
Listeria monocytogenes
|
|
What meningitis-causing virus is shown here? What specifically is shown?
|
Herpes Simplex Virus
Intranuclear Inclusions Shown |
|
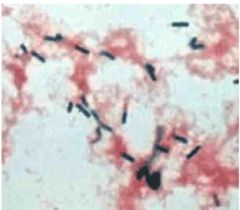
What meningitis causing bacteria is shown? What is its morphology and gram stain? How does it appear on blood culture? What demographics does it affect?
|
Listeria monocytogenes
G(+) Rods β-hemolytic on blood agar (can also use motility test) Affects all demographics |
|

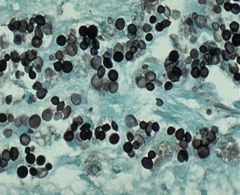
What meningitis causing fungi is shown? What is its main virulence factor? What is its natural habitat?
|
Cryptococcus Neoformans
• Antiphagocytic polysaccharide capsule • Habitat: soil enriched with bird droppings |
|
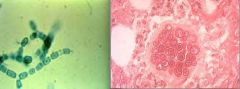
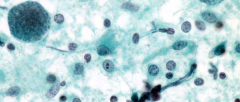
What meningits causing pathogen is shown? What form is shown on the left? Which on the right? What is the natural habitat?
|
Coccidioides immitis
• (L) Environmental form: hyphae breaking up into arthroconidia • (R) Tissue form spheules filled with endospores • Natural habitat is the dessert sand (causes valley fever) |
|
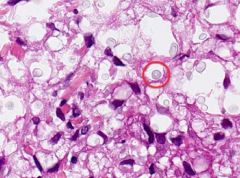
What is shown? What virulence factor is shown (circled?)
|
Cryptococcal scalp infxn in a lymphoma pt (immunocompromised)
• Can see a very thick mucoid capsule |
|
What is pictured? What visualization technique is being utilized?
|
• Cryptococcus neoformans
• Silver stain |
|

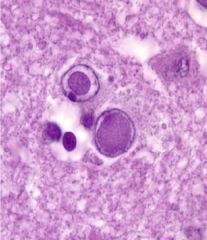
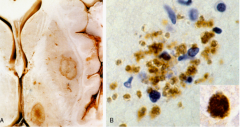
What is pictured on top? On bottom? What can this pathogen cause?
|
Top: Toxoplasma gondii tachyzoites (crescent shaped w/ prominent nuclei)
Bottom: Toxoplasma gondii cysts in brain tissue stained w/ hematoxylin & eosin Can cause: • Fatal encepahlitis in immunocompromised pts • Microcephaly/Still birth if infxn early during pregnancy • Neuro problems/blindness if infxn late in pregnancy |
|

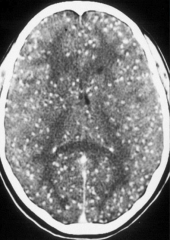
A patient. a 44 yo heart transplant patient, compainned to her 1º phys about headache nausea, & vomiting approx 1 yr after transplant. She had no skin lesions. A computed tomographic scan of the head demonstrated rign-enhancing lesions. A biopsy of the lsions was performed All cultures (bacterial, fungal, viral) were negative. Special stains do the tissue revealed multiple cystlike structures of varying size
a. Coccidioides immitis b. Cryptococcus c. Listeria d. Naegleria e. Toxoplasma gondii |
E. Toxoplasma gondii
|
|
What pathogen is caused? Who does it affect?
|
Toxoplamsis gondii: Cysts w/ bradyzoites
• Reactivation can occur in immunocompromised pts. |
|
What is shown on the left? What is shown on the right? What is the pathogen?
|
• (L) Abscesses in the putamen & thalamus
• (R) Free tachyzoites • Toxoplasmosis gondii |
|
What is shown?
|
Massive neurocysticercosis
|
|
|
What pathogen has a prediliction for brainsem & meninges that can lead to meningits, encephalitis, and brain abscesses?
|
Listeria monocytogenes
|
|
|
What meningitis causing pathogen is β-hemolytic on blood agar and can be identified using the motility test?
|
Listeria monocytogenes
|
|
|
What are the mechanisms (3) by which viral infections in the CNS cause problems?
|
• Direct cytolytic effects
• Inflammatory or immune mediated effects • Vasculitic effects |
|
|
What are the mechanisms (3) by which viruses enter the brain?
|
• Crossing the blood brain barrier directly
• Transportation via infected lymphocytes or macrohages • Retrograde axonal transport |
|
|
What family of viruses most commonly cause meningitis? Are these viruses enveloped or non-enveloped? DNA or RNA? ss or ds?
|
• Enteroviruses (members of the Piconaravirus family)
• Of these the most common are Coxsackie B virus & echoviruses • Non-enveloped viruses ssRNA virus |
|
|
Viral meningitis caused by enterovirus cause meningitis is 90% of ____?
|
• 90% of patients are < 1 yr old.
|
|
|
Polio virus is a member of what family? Enveloped? ss or ds? DNA or RNA?
|
• Enterovirus (Picornavirus)
• Non-enveloped ssRNA virus |
|
|
How does Polio cause paralysis?
|
• Transmitted fecal-oral route
• Replicates in oral cavity & gut • Infects and kills cells in the anterior horn of the spinal cord. |
|
|
What are the two types of polio virus vaccines? What are the differences?
|
• Salk vaccine: *Killed* virus vaccine
• Sabin vaccine: *Live* virus vaccine *Sabin virus provokes the production of secretory (mucosal) IgA - Nasal IgA and Duaodenal IgA* Salk does not. |
|
|
What CNS infection causing virus is bullet shaped and is an enveloped ssRNA virus?
|
• Rabies virus (rhabdoviridae)
|
|
|
What are the morphological characterisitcs of rabies? ss or ds? Enveloped? RNA or DNA? What family is the virus a member of? What disease does it cause?
|
• Bullet-shaped
• enveloped ssRNA virus • Rhabdoviridae virus • 100% fatal lethal encephalitis |
|
|
What is the most common cause of rabies in the US? Worldwide?
What animals are the most common reservoirs of rabies? |
• Bats (US)
• Dogs (Worldwide) • Reservoirs: Skunk (CA, Middle of the country N&S) Fox (NM, Texas, Alaska, NH & VT) Racoon (East coast) |
|
|
How does the rabies virus travel? What neurons does it target? What pathology finding is diagnostic?
|
• Retrograde movement up axons
• Affinity for hippocampal neurons (mne: why victims "forget" their friends and attack them) • *Negri bodes* (inclusion bodies in the cytosol) |
|
|
What are the two manifestations of rabies infection? Where is the virus present?
|
• Encephalitic (Furius) form: more common. Sx: excitement, tremors, muscular contractions/convulsions, phobic spasms, ↑ sensitivity of the nervous system, hypersalivation
• Paralytuc (dumb) form: Sx: lack of aggression, paralysis of muscles, speech & respiration • Virus is present in salica, tears, skin & brain |
|
|
What is the Tx for Rabies? When must it be given?
|
• No Tx possible once symptoms appear.
• Wounds should be washed • Vaccines given: • Passive immunixation: Anti-rabies Ig • Inactivate viral vaccine (given w/in 8 days) give IM in 3-5 doses at 0, 3, 7, 14 & 28 days (*0, 3, days, 1wk, 2 wk, 4 wks) |
|
|
What virus presents as painful often debilitating rash along a dermatome? What is the term for the pain that persists for more than 3 mos after the resolution of the skin lesions?
|
• Herpes zoster (shingles), from reactivation of latent varicella zoster virus
• Post-herpetic neuralgia |
|
|
Who is most often affected by Herpes zoster outbreaks? Why does it occur? What is the most frequent distribution?
|
• 50-70% occur in pts >50 yrs of age
• Occurs due to a decline in VZV-specific T-cell immunity • Can occur on any dermatome, most frequently affected are the *Thoracic nerves*, followed by the *Opthalmic division of CNV*. |
|
|
What are the first-line treatments for post-herpetic neuralgia? Second line? What drugs are inneffective? What is the only form of prevention?
|
• 1st line: gabapentin or pregabaline & lidocaine patches
• 2nd line: opiods, topical capsaicin, TCA antidepressants (amitriptyline or nortriptyline) • NSAIDs and anti-virals are inneffective • Zostavax (live attenuated vaccine for pts > 60 yo) |
|
|
What virus usually causes Herpes simplex encephalitis? Herpes simplex meningitis?
|
• HSV1 for HSE (except in neonates when it is HSV2)
• HSV2 for HSM |
|
|
What virus can cause focal hemorrhagic necrosis of the temporal & frontal lobes?
|
• Herpes Simplex I - causing Herpes simplex encephalitis which is a medical emergency, unTx ≈ 70% mortality
|
|
|
What virus is common in Mollaret's syndrome (a syndrome of benign recurrent episodes of aseptic meningitis?)
|
HSV2
|
|
|
What procedures are used to diagnose HSV infections in the CNS? What is the Tx?
|
• 1: PCR
• 2: Cranial CT or MRI • CSF analysis. Lymphocytosis is observed. *RBCs in CSF are typical but NOT diagnostic* • Tx: IV Acyclovir (reduces mortality) |
|
|
What virus family is West Nile Virus part of? What is the main vector?
|
• Flavivirus family
• Vector = mosquito Culex pipiens (US) |
|
|
What are the two manifestations of West Nile Virus? Who is at greatest risk? How is it diagnosed?
|
• Most infxns are asymptomatic
• 20% West Nile Fever (flu-like) • < 1% Neuroinvasive disease: Aseptic meningitis (<1% mortality), encephalitis (12-20% motality), poliomyelitis (10-50% mortality), multifocual chorioretinitis • Advanced age > 55 is greatest risk factor. • Dx: ELISA for IgM to WNV |
|
|
What is unique about West Nile Viral meningitis and encephalitis? How is it diagnosed?
|
• WNV meningitis: Tremor is present
• WNV encephalitis: Fever, headache, altered mental status and postural or kinetic *tremor* Dx: ELISA for IgM to WNV |
|
|
What flavivurs is mosquito born and causes episodic outbreaks (sometimes causing encephalitis)?
What flavivirus is the largest world-wide cause of epidemic encephalitis What togavirus is mosquito borne and causes local outbreaks of encephalitis? |
• St. Louis encephalitis (West Nile is also flavi and mosquito borne)
• Japanese B encephalitis (JBE, mortality 20-30%) • Eastern equine encephalitis (mortality 33%) |
|
|
Describe the neuropathogenesis of HIV infxn
|
• Appears as an aseptic meningitis, Asym. Mild neurocognitive impairment (ANI), Mild neurocognitive disorder (MND), HIV-associated dementia (HAD)
• *HIV does not directly infect neurons* --> HIV infected monocytes provoke a neuropath response by releasing cellular toxins --> behavioral abnormalities, motor dysfunction, frank dementia • MND (30% of pts) does NOT progress to HAD • ***HAD is characterized by progressive neuro abnormalities and is associated with HIGH viral loads*** (is AIDS defining) |
|
|
The JC polyoma virus is a member of what family? Enveloped? Ss or ds? RNA or DNA? What does it cause? How does it cause its damage?
|
• Member of the polyoma virus subfamily of papavaviridae
• Non-enveloped ds DNA virus • Opportunistic, causes progressive multifocal leukoencephalopathy (PML) • Most common opportunistic CNS infxn after toxoplasmosis • Damage by cytolysis of glial cells and oligodendrocytes |
|
|
What CNS virus can present as hemiparesis, ataxia, visual distrubances, higher cortical dysfxn, w/ rapid progression to death in immunocompromised pts?
|
• Progressive multifocal leukoencephalopathy caused by JC polyoma virus
|
|
|
What cells does the JC polyoma virus preferentially target?
|
*Cytolytic* for glial cells and oligodendrocytes
|
|
|
What are the steps for JC polyoma virus diagnosis?
|
• MRI
• PCR of CSF |
|
|
What three viruses can cause encepthalitis? What two viruses can cause poliomyelitis? What virus can cause meningitis?
|
• Encephalitis: Herpes Simplex, Rabies, West Nile
• Poliomyelitis: Poliovirus, West Nile • West Nile |
|
|
What are some complications of neonatal CMV infections?
|
• Microcephalus
• Cortical atrophy and periventricular calcifications |
|
|
What encapsulated yeast can cause meningitis in pts with depressed immunity? What is the natural habitat for this fungi?
|
Cryptococcus neoformans
• Soil enriched with bird droppings |
|
|
What is the main virulence factor of cryptococcus neoformans?
|
• Antiphagocytic polysaccharide capsule
|
|
|
What preparations (2) are used for diagnosis of cryptococcus neoformans? What test? How does the CSF appear?
|
• Sabouraud agar (culture) and India Ink stained preparation
• Use latex agglutination tests for capsuar antigen detection • CSF appear w/ lymphocytes, high protein & low glucose. |
|
|
What meningitis causing pathogen is best visualized on an india-ink stained preparation? What kind of pathogen is it?
|
• Cryptococcus neoformans
• Encapsulated yeast |
|
|
What meningits causing pathogen is a dimorphic fungi that has two forms:
environmental: hyphae breaking up into arthroconidia tissue: spherules filled with endospores? What is its natural habitat? |
• Coccidioides immitis
• Habitat: desert sand (common in the SW - and San Juaquin Valley!) |
|
|
How does coccidioides immitis infect? What is the main virulence factor?
How can you diagnose infection? |
• 1º site of infxn is the lung
• Virulence factors arthroconidia --> Spherules (resistant to phagocytosis) • CSF: lyphocytes, high protein, low glucose (culture is only possible in < 50% of cases) |
|
|
How does an autoposy of a brain infected by cryptococcal encephalitis appear?
|
• Appearance of soap bubble cysts.
• Disseminated cocci looks very granulomatous |
|
|
What free-living amoebae can cause primary meningoencephalitis? Who does it tend to affect? How is it transmitted?
|
• Naegleria fowleri
• Affects children and young adults • Swimming in fresh, shallow water during warm weather • Fatal! |
|
|
What are the 3 stages of Naegleria fowleri's life cycle? Which form is infective? How do they enter the body?
|
• Cysts, Trophozoites, and flagellated forms
• Infective forms: trophozoites & flagellated forms • Enter the body via the olfactory neuroepithelium then reach the CNS --> purulent hemorrhagic inflammatory rxn |
|
|
What pathogen causes a meningoencephalitis that presents with rapid onset, severe headache, altered sense of smell, progresses rapidly to coma and death in a few days? What is the Tx?
|
• Naegleria fowleri
• Amphotericin B |
|
|
Labs come back as:
• CSF: purulent, bloody, lots of PMNs, high protein, low glucose • Motile trophozoites in CSF • Use of Trichrome of Giemsa stained smear • Cuture on plates seeded w/ G(-) bacteria What pathogen is this? What does it cause? |
• Naegleria fowleri
• Causes a hemorrhagic meningoencephalitis |
|
|
What free-living amoebae that lives in soil; fresh, brackish, and sea water; sewage; swimming pools; and contact lens equipment can cause a diffuse necrotizing granulomatous encephalitis? Who does it tend to affect?
|
• Acanthamoeba species
• Immunocompromised patients (in contrast to Naegleria fowleri which tends to affect immunocompetent pts) |
|
|
What are the 2 stages of Acanthamoeba? What is the infective form? How does it enter the body? What does it cause? What is the Tx?
|
• Cysts & Trophozoites
• Infective form: trophozoites • Enters the body via the lower respiratory tract or broken skin --> invades CNS through hematogenous spread • Causes diffuse necotizing granulomatous encephalitis • Ketoconazole & Amphotericin B |
|
|
In addiion to the subacute or chronic granulomaouts amebic encephalitis, what else can Acanthamoeba cause? What is the Tx?
|
• Keratitis and corneal ulcers following corneal trauma or in association with contact lenses
• Propamidine & miconazole nitrate w/ neomycin |
|
|
Labs show:
• Stained smears of cornea and brain biopsy which show trophozoites and cysts • Culture on media seeded w/ G(-) bacteria • Identification by direct immunofluorescent Ig • What pathogen is this? What does it cause? |
• Acanthamoeba
• Causes Subacute or chronic granulomatous amebic encephalitis or keratitis/corneal ulcers |
|
|
What intracellular pathogen has cats as its definitive host? How is it transmitted?
|
• Toxoplams gondii
• Tranmitted by ingesting undercooked infect meat containing cysts, ingestion of oocysts via fecal oral route, transplascental transmission, blood or organ transplant |
|
|
After ingestion of oocysts how is Toxoplasma gondii spread? What can occur in immunosuppresesed pts?
|
• Ingestion --> mature to tachyzoites --> invade macrophages (intracellular pathogen) --> transported through lymphhematogenous system to all organ systems --> cyst development in the brain, heart & skeletal muscles.
• Can remain latent, but if immunosuppressed you can have reactivation of the cysts (parasitologic relapse) |
|
|
What are the risks of Toxoplasma gondii infxn in immunocompromised hosts?
|
• Toxoplamic encephalitis (reactivation of parasite) --> highly lethal
|
|
|
If a mother already has toxoplams gondii what happens?
• If she is infected early druring the pregnancy what happens? • If she is infected late during the pregnancy what are the consequences? |
• Already has it, maternal Ig protect the baby
• Early infxn: Crosses placenta --> severe conential infxns, hydro/microcephaly, still birth • Later infxn: Crosses placenta --> infxn may not be apparent --> if untreated, congential infxns may lead to progressive blindess or neurological problems |
|
|
How can you diagnose Toxoplasma gondii infxn? What is the Tx?
|
• Serologica testing (rising or high titers of IgM)
• Observation of parasite in tissue biopisies or body fluids • Intraperitoneal inoculation into mice • PCR • Tx: Sulfadiazine + pyrimethamine (in immunocompromised pts). • In pregnant women pyrimethamine can not be used (teratogenic). Use Clidamycin & spramycin |
|
|
What is one of the risky sequelae associated with epidural abscesses?
|
• Dangerously increase intracranial pressure (Think! The dura is all connected through the spinal canal)
|
|
|
What is the w/u for a epidural abscess? What abx should be used?
|
• CBC, blood culture, culture of abscess
• MRI **cornerstone of diagnosis** • CT scanning • Vancomycin for G(+), 3rd and 4th generation cephalosporins (require CNS penetration), Meropenem (penetrates well into CSF) |
|
|
What can cause spongiform encephalopathies? What is the name of the disease?
|
• Prions
• Creutzfeldt-Jakob disease (or Bovine Spongiform encephalopathy - mad cow disease) • Variant Cruetzfeld-Jakob is infections • Degenerative and 100% lethal |
|
|
What is the pathogenesis of prion disease?
|
• Infxn agent is mutant protein Prp-sc
• Prp-sc is pathogenic and is a misfolded version of the normal PrP-c protein (infectious in vCJD or Kuru, and sporadic in CJD) • Brains exhibit pronounced spongiform ∆, neuronal degeneration/death, astogliosis |