![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
84 Cards in this Set
- Front
- Back
|
Standard Deviation |
Standard deviation is a measure of dispersion- allows us to see how spread out the scores are from the mean. |
|
|
Describe the graph |
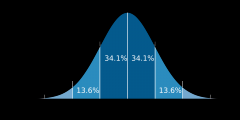
-34% of scores lie within one standard deviation of the normal = 68% in total -About 95% like within 2 standard deviations-Beyond 2 standard deviations is beyond normal limits = 2% above 2 sd and 2% below 2 sd |
|
|
Evaluation of statistical definition of abnormality Strengths (3)
|
1. Characteristics measured objectively e.g. cognitive tests = more scientific 2. Being objective means it is RELIABLE – resultsare consistent 3. Used to diagnose mental retardation |
|
|
Limitations of statistical definition of abnormality |
1. Limited to characteristics that can be measurede.g. phobias cannot be tested 2. Fails to distinguish between desirable and undesirable behaviour, gifted could be said as abnormal e.g an amazing guitarplayer is considered as abnormal and not gifted 3. Person may be classified as normal but still need help e.g. 70= normal, 71= not normal because more than 2sd away from normal 4. At what point do we draw the line between normal and abnormal? |
|
|
Social Norms definition of abnormality |
1. Norms are social ''rules'' that are not laws but customs and people in a society abide by these rules 2. Behaviour that conforms to social norms is normal 3. Behaviour that does not conform to social norms is abnormal |
|
|
The effect of culture |
1. Cultures vary within societies - made up of different cultures and subcultures 2. Behaviours seen as abnormal in one culture may not be seen as abnormal in another 3. e.g. hearing voices in your head |
|
|
The effect of context |
1. situation and context are important 2. e.g. person dressed up as a princess okay on dress up day but not to go to an interview. |
|
|
The effect of age and gender |
1. Normal for 3 year old to be afraid of monsters under their bed but not for an adult 2. Normal for woman to wear a dress but not for a man |
|
|
The effect of historical context |
1. Behaviours considered abnormal decades ago, may not be abnormal in today's society 2. e.g. homosexuality |
|
|
Evaluation of social norms definition of abnormality Strengths (2) |
1. Allows us to take into account the effect the behaviour have on others. Deviance = breaking rules, this is socially unacceptable behaviour and makes it difficult for people to live together 2. Allows us to take several behaviours into account, which all together makes people feel uncomfortable |
|
|
Evaluation of social norms definition of abnormality Limitations (6) |
1. Idea is culturally biased as what is seen as unacceptable in one may be seen as acceptable in another 2. Definition can lead to abuse of a persons rights e.g. slaves who had an ''irrational desire'' to run away from their masters 3. Hard to have a reliable idea about what is abnormal if age, gender, culture, etc need to be taken into account 4. Makes diagnosis difficult as not universal norms 5. Norms change over time, so would only be valid at that time and in one particular culture, with one gender, one age group and in a particular situation 6. e.g. pregnant single women used to be put in a mental asylum |
|
|
What does DSM stand for? What does it provide? |
Diagnostic and Statistical Manual Criteria from which mental disorders can be diagnosed |
|
|
Axis I |
All diagnostic categories e.g. schizophrenia, developmental disorders such as autism, phobias, eating disorders, etc. Problems tend to need immediate attention |
|
|
Axis II |
Personality Disorders and Mental retardation e.g. OCD, antisocial personality disorder |
|
|
Axis III |
Looks at mental and physical conditions that may aggravate existing conditions e.g. physical problems such as diabetes may be the root of mental problems |
|
|
Axis IV |
Looks at psychosocial and environmental factors that may affect the disorder e.g. financial problems, poverty, educational problems, dysfunctional relationships, etc. |
|
|
Axis V |
Assessment of global functioning - overall rating of someone's ability to cope with normal life (1=DANGER, 100=superior range of abilities) |
|
|
Strengths of DSM (3) |
1. Allows for a common diagnosis = RELIABLE 2. Allows for more accurate treatment 3. Draws upon a multi- axis system to draw upon different methods for diagnosis = VALID as less reductionist |
|
|
Weaknesses of DSM (2) |
1. Mental health issues are seen as "patients" in need of "treatment" 2. However, it could be said that some mental heath issues are just another way of living a life |
|
|
Question on reliability and diagnosis of metal disorders |
1. Reliability refers to the consistency in diagnosis 2. It is a joint enterprise between the diagnostic scheme and the person doing the diagnosing. SO important that people using DSM agree on symptoms 3. ISSUES - Different clinicians diagnose the same symptoms differently = unreliable SO - treatment may not work - predictions about progress of illness may not be valid 4. REASEARCH = GOLDSTEIN |
|
|
Clinical Psychology - define |
1. Explaining and treating mental illness 2. Seeks to define what makes behaviour abnormal and then diagnose to treat 3. Clinicians note of any symptoms and for how long they have had them |
|
|
Question on validity and diagnosis of metal disorders |
1. If sympotoms match those considered to be present in the disorder = VALID e.g (explain depression) 2. If the diagnosis accuretly predicts the course of the illness = VALID 3. If the treatment put in place after diagnosis is made is effective = VALID 4. If diagnosis is redone and is not the same, not only is it not RELIABLE, it is also not VALID 5. ISSUES - you need to operationalise measurements in order to meaure them. - may lose some understanding of illness- LACK VALIDITY 6. RESEARCH = Rosenhan - all patients had same symptoms but one was given different diagnoses = INVALID
|
|
|
Describe the statistical definition of abnormality |
1. About statistical infrequency - statistically rare = abnormal 2. Assumption that any human characteristic, including behaviour is spead in a normal way across the general population 3. Where an individuals score lies on the graph is an indication of where they are in relation to the rest of the popualtion |
|
|
Culture and the diagnosis of mental disorders definition |
2. The clinician and patient may be from differnt cultures, so cultural issues may have to be considered |
|
|
Give examples of differences in culture |
1. Clinicians may not recognise symptoms as condition may be specific to particular culture e.g. ghost sickness - Native American tribes - caused by associating with the dead
2. Cultures may vary on how much information they disclose -Sue and Sue found Asian Americans don't like to talk about their emotions
3. Clinicians reluctant to give culturally sensitive dianosis - schizophrenia in Japan - (Sato study)
4. Some behaviours are interpreted differently in differnt cultures - schizophrenia in Costa Rica = spirits talking to the individual - seen as a gift
5. An interpreter may be used - may filter quesions/answers to be culturally desirable |
|
|
Goldstein - Aim
|
1. To examine gender differences in schizophrenia patents over a 10 year period using hospital records from a previous study 2. To explain the effect of gender on the course of schizophrenia |
|
|
Goldstein - Method ( + assessment of the reliability )
|
1. Data originally gathered by Kriesman and Joy's + funded by the NIMH (national institute of mental health) 2. patients admitted from 1972-1973 following criteria - diagnosed with schizophrenia - stayed for less than 6 months - aged between 18-45 - none had other issues, e.g. drug/alcohol abuse -199 patients met this criteria 3. Goldstein and another researcher rediagnosed using DSM III 4. 169 patients were said to have schizophrenia 5. 8 were randomly selected for re diagnosis by 2 other psychiatrists = 0.8 INTER-RATER AGREEMENT |
|
|
Goldstein - assessment of gender differences in schizophrenia
|
1. Women, (from previous research) experience a less severe course of illness than men so a sample with multiple hospitalisations would exclude these. 2. SO only first time admission cases were used, BUT small sample, so 1 previous hospitalisation patients were also used. = 90 participants 3. Characteristics = - mean age of 24 -mainly never married -high level of education -middle class |
|
|
Goldstein - How the information was gathered
|
1. Premorbid functioning (before the illness) -measured using a rating scale -isolation, peer relationships and interests for pre-teen and teen years 2. Social functioning -information on marital status and occupational status 3. Course of illness -Number of re-hospitalisations and length of stay in hospital over 10 year period |
|
|
Results of Goldstein
|
1. Men had higher re-hospitalisations over 10 year period - pre morbid functioning due to this 2. Men's stay was also longer over the 10 years - mostly due to social functioning 3. Pre morbid and Social functioning accounted for gender differences |
|
|
Gottesman and Shields - Aim
|
1. To investigate how far schizophrenia is influenced by genes 2. To try and replicate other studies that have shown a genetic link |
|
|
Gottesman and Shields - Method
|
1. Analysed secondary data from hospital in USA, individuals diagnosed with schizophrenia over 16 year period 2. 62 patients who were one of a twin 3. 5 = both MZ twins had been diagnosed with schizophrenia 4. Of the 57, tracked down other twin 5. Blood groups, finger prints and visual tests were used to check whether MZ or DZ 6. "found twin" = semi structured interviews, hospital records, personality testing to see if been diagnosed with schizophrenia / disorder similar |
|
|
Gottesman and Shields - Results / Conclusions
|
1. 42 % of MZ twins had diagnosis of schizophrenia, compared to 9 % of the DZ twins 2. Some genetic basis for schizophrenia + 11 other studies that they looked at also agreed |
|
|
Evaluating Twin studies - generalising, validity, cause and effect, (2) ethics, external reliability, study
|
1. Use humans so good generalisability 2. Deal with real life cases, rather than inducing the condition = valid 3. We cannot say that genes cause an individual to develop schizophrenia 4. - Consent would need to be given. - If results in revealing symptoms the individual in unaware of - may cause distress 5. Difficult to replicate to test reliability as population of twins with schizophrenia is very low 6. No two individuals share the same environment - even in the womb they don't - Rosenthal studied the Genain triplets where they all gained schizophrenia but at different ages, suggesting yes, it may be genetic but they and sufficiently different experiences within the family to alter the onset of disorder TWINS = GOLD STANDARD OF GENETIC INFLUENCE |
|
|
Evaluating Animal experiments - generalising, validity (3), cause and effect, ethics (2), external reliability
|
1. Cannot generalise from animal to humans, brains may be similar but doesn't mean they work in the same way 2. - Internal valid as control of variables - Not possible to investigate symptoms such as hallucinations - Symptoms may be indicative of schizophrenia, but may not be the same 3. Even if amphetamines produce similar symptoms found in schizophrenia, cannot conclude dopamine hypersensitivity causes schizophrenia 4. - Possible to do things to animals you would not to humans. - Comply with strict ethical issues then study is ethical 5. Easy to replicate as study controlled all variables |
|
|
Randrup and Munkvad - Aim
|
A study using rats to see if schizophrenia like symptoms can be induced by injection of amphetamines
|
|
|
Randrup and Munkvad - Method
|
1. White, male rats aged 3-6 months used 2. Housed individually and fed same food for a duration of time 3. Observed to get a baseline measurement of behaviour 4. Rats were injected with amphetamines according to body weight 5. Observed continually for a period of 6 hours after injection |
|
|
Randrup and Munkvad - Results + Conclusions
|
1. Displayed stereotypical sniffing, licking, biting behaviours 2. Some had increased level of activity 3. As amphetamines increase the level of dopamine in the brain, study supports this explanation |
|
|
Rosenhan "On being sane in insane places" - Aim ( 2 )
|
1. To see if 8 sane people who gained admission to 12 different hospitals would be found out as sane 2. To find out what it feels like to be in such an institution and what it feels like to be treated as "insane" |
|
|
Rosenhan "On being sane in insane places" - Method
|
1. 8 pseudo patients (3 women, 5 men) 2. 12 different hospitals in 5 different states, varying in character 3. Patients made appointments and claimed they hear voices, unclear but some words like "empty" 4. Gave false names and changed some history 5. Once admitted, they behaved normally |
|
|
Rosenhan "On being sane in insane places" - Results
|
1. All except one was admitted with schizophrenia, one with manic depression 2. No records or behaviour showed by hospital staff doubted the diagnosis 3. Some real patients doubted, saying "you're not crazy" 4. Average of 19 days spent in hospital before being discharged |
|
|
Rosenhan "On being sane in insane places" - Conclusions
|
1. The staff couldn't distinguish between sane and insane = DSM was NOT a valid measure at the time
|
|
|
Schizophrenia - Symptoms ( definition and examples)
|
1. What characterise the disorder in terms of how the person thinks, feels and behaves 2. +ve symptoms (in addition to behaviour) - hallucinations - delusions e.g. grandeur, paranoid, etc - thought disorders - disorganisation of behaviour e.g. wearing winter clothes in summer -ve symptoms (absence from normal behaviour) - flattening affect - lack of emotion - social withdrawal - poverty of speech |
|
|
Schizophrenia - Features ( definition and examples)
|
1. Features are facts about the disorder and include statistics 2. - A quarter of people will have one episode and recover - A quarter will have it continually - Half will have periods of recovery and periods of symptoms - Equally common amongst men and women - There are different types of schizophrenia |
|
|
Name 3 different types of schizophrenia
|
1. Paranoid - suspicous of others and have delusions of grandeur 2. Disorganised - speech disorganised 3. Catatonic - very withdrawn and isolated, little physical movement |
|
|
Evaluation of diagnosis of schizophrenia (3)
|
1. +ve symptoms tend to have a greater weight when diagnosing, but can have cultural differences e.g. hearing voices 2. -ve symptoms tend to be less affected by cultural differences and can be measured more objectively e.g. social withdrawal 3. Initial features have been found present in many children but cannot on their own indicate schizophrenia |
|
|
What is schizophrenia?
|
A psychotic disorder that affects how a person thinks, feels and behaves. There are 3 types of schizophrenias- paranoid, disorganised and catatonic. There are also positive and negative symptoms that affect the individual. E.g. hallucinations and social withdrawal.
|
|
|
Biological Explanation of Schizophrenia Biochemical Factor - Dopamine Hypothesis (Describe) |
-Research suggest presence of excess dopamine receptors at synapse in brain leads to schizophrenia - as brain is "hypersensitive" - hallucinations may occur as brain is hyper-stimulated -effect of anti-psychotic drugs to treat schizophrenia = chlorpromazine blocks dopamine receptors, reducing sensitivity - logic = reducing sensitivity to dopamine means excess number is the cause |
|
|
Research evidence into Schizophrenia Dopamine Hypothesis (3)
|
1. Randrup and Munkvad 2. Recreational Drugs - Amphetamines cause excess dopamine and symptoms simular to +ve ones shown in schizophrenia e.g. hallucinations BUT doesnt produce -ve symtoms so dopamine hypothesis is insufficent ALSO amphetamines also have symptoms of over confidence + high alertness = mania not schizophrenia 3. Parkinson's - associated with low levels of dopamine + symptoms of stiffness and shaking of limbs - anti psychotic drugs (results in low levels) show symptoms simular to Parkinson's = LINK BETWEEN SCHIZOPHRENIA AND HIGH LEVELS |
|
|
Evaluation of Dopamine Hypothesis (5)
|
1. Evidence comes from variety of sources - TRAINGULATION = VALID - animal testing, PET scanning, looking at recreational drugs + Parkinson's disease 2. Biological reasearch such as animal testing enables good controls = scientific BUT obvious differences between animals and humans + scans are reliable and objective BUT lack sophistication so detail hard to study 3. Research is correlational - no cause and effect as could be schizophrenia that caused dopamine levels 4. Blocking dopamine receptors takes a few days to work - antt-psychotic drugs block immediately but symptoms take a few days to go suggests something other is causing symptoms 5. Other explanations - Twins (MZ) shows higher frequency = genes are involved - Social and Environment factors seem to trigger schizophrenia so not efficent enough -perhaps , stressful situations can trigger production of dopamine |
|
|
Social Explanation of Schizophrenia (Description- 4)
|
1. Prevalence of schizophrenia in Lower Social Classes -e.g. immigrants have higher incidence in the UK (African - Carribean and black immigrant) = social class is involved 2. Difference in course of illness + Different medical care - more likely to be brought in by social care or police 3. Lower SES associated with various forms of deprivation which are stressful -over crowding, discrimination, standard of housing - immigrant more likely to live in inner city areas = higher incidence rate 4. Could the reason be Genetic? - more likely to be associated with the stress of adapting to a new way of life - In the Carribean, population of schizophrenics is same as white population in UK - suggests social not genetic |
|
|
Evaluation of Social Causation Hypothesis (5)
|
1. Not everyone with certain environmental conditions has schizophrenia 2. Other explanations like dopamine and genetic 3. Possible that both have an effect 4. Those living in lower social economic groups more likely to be diagnosed = bias 5. Difficult to seperate environmental factors to see if they cause schizophrenia |
|
|
Comparing the Dopamine Hypothesis with the Social Causation Hypothesis (paragraphs 4)
|
1. Nature / Nurture debate 2. Role of genetics in both debates - social causation, black African, higher incidence BUT could be due to lower SES + enironment 3. Nature of research evidence 4. Applications - Dopamine = drugs, Social = better living conditions (more treatment = long term) (drugs= treats symptoms so short term) |
|
|
Treatment of Schizophrenia Biological Approach: Drug Treatment (chemotherapy- altering biochemistry of the brain) - Description |
- "typical" - treats +ve symptoms e.g. haloperidol, chlorpromazine - "a-typical" - both +ve and -ve symptoms e.g. risperidone - prescribed by a psychiatrist - orally- tablet or liquid- injection (depot- admission= slow release) - person has to be monitored to see if right drug / dosage okay |
|
|
Treatment of Schizophrenia Biological Approach: Drug Treatment (chemotherapy- altering biochemistry of the brain) - Evaluation (5) |
1. Drugs have side effects, so have to get a good balance between reducing symptoms and side effects - tiredness, shaking, problems with sex drive and weight gain 2. Meltzer, et. al. - 481 patients with schizophrenia - Given either a placebo or haloperidol (anti- psychotic drug) for 6 weeks - Gathered info on +ve and -ve symptoms - Haloperidol gave significant improvements compared to placebo = EFFECTIVE 3. Ethical issue = some see it as a "chemical strait jacket", raising issues over social control 4. Do not take into account a persons social and environmental conditions which may contribute to relapses 5. Tend to be more effective at +ve symptoms then -ve |
|
|
Treatment of Schizophrenia Social Approach: Care In the Community - Description (5) |
1. It is a programme of support and treatment provided while the patient lives in the community, either at home or in a shelted accommodation 2. Can call upon psychiatric nurses 3. Medication will be self-administered 4. Hospitalisation is last resort 5. Support it provided so individuals feel they are able to deal with enviromental conditions which may trigger their illness |
|
|
Treatment of Schizophrenia Social Approach: Care In the Community - Evaluation (6) |
1. Potentially improves quality of life as able to maintain a normal life 2. Problems/symtoms assciated with institutionalism reduced (social withdrawal, low self-esteem, etc.) 3. Chronic underfunding leads in inadequate provision e.g. emergency helplines restricted = drugs not taken = danger to patient/community 4. This is locally specific so affluent areas do well Kuno, et. al. - American study - Affluent white areas = higher quality than low income Afrian- American areas 5. Inadequate hospital beds = not admitted when should be 6. Coping with mentally ill person can put strain on families leading to further problems |
|
|
Treatment of Schizophrenia Learning Approach: Token Economy Programmes - Description |
-Operant Conditioning - Uses +ve reinforcement - Form of behaviour modification - Tokens used as rewards - They are secondary reinforcers |
|
|
Treatment of Schizophrenia Learning Approach: Token Economy Programmes - Evaluation (6) |
1. Mumford, et. al. - study into the effectiveness with long-term schizophrenic patients 2. Principles are based of reasearch - great work with e.g. animals provided the reliability of operant conditioning (Skinners Rats)
|
|
|
Symptoms of Depression
|
-Extreme Lathargy
-Distured sleep -Lack of sex drive -Permanent anxiety and irritability |
|
|
Features of Depression
|
-Twice as common in women -Tend to live a shorter life |
|
|
Psychodynamic explanation of Depression
|
Potential for depression was created in childhood - specifically in the oral stage of psychosexual development 1. Child Experiences loss, e.g. mother going to work 2. Child experiences sense of rejection - feels anger 3. Child is unable to express their anger so is interjected, resulting in blame/self punishment 4. IF FIXATED = Emotional bonds cannot be broken- seperation is not made and anger continuous to be directed towards the self. SO in adulthood - Person is likely to regress to the oral stage (most dependant) giving them comfort NOT FIXATED = Period of Mourning follows - memories of lost one are recalled, enabelling seperation |
|
|
Evaluation of Psychodynamic explanation of Depression (4) |
1. NIETZEL AND HARRIS provided evidence that people with depression are high in dependency - what would be predicted in psychodynamic explanation
|
|
|
Treatment of depression - Psychodynamic Approach Description (4) |
1. Described as "royal road to the unconscious" Dreams allow repressed material to leak out so people can express their desires SAFE RELEASE (cathartic release), once being made aware of the problem, person can deal with problem with an adult ego Relieving the tensions of repressed sexuality, traumatic events, etc. which must be controlled in civilised society = WISH FULFILMENT 2. Understanding = mental ill people can acknowledge thought and deal with them e.g. Depressed person could be made aware of the cause of processes in their unconscious which may be the cause of their depression 3. True meaning of dreams hidden SO needs therapist to interpret Symbols are unique to the individual
4. Transformation from forbidden desires to manifest content = DREAMWORK |
|
|
Evaluation of dream therapy for depression (6)
|
1. HEATON ET AL 2. Dream analysis is subjective = not scientific as differnt interpretations
= ethical issue as there is a sexual nature that the patient may transfer feelings of love onto therapist (erotic transference)
e.g severely depressed as no motivation to continually go to sessions 5. Biological psychologist dismiss that dreams have any meaning - by-product of random firing in the brain
|
|
|
The Cognitive Model/Explanation of depression - AARON BECKS EXPLANATION (2) |
1. Disfunctional beliefs/negative thinking give rise to cognitive errors which results in depression cognitive errors = -selective thinking - focusing on negative details, whilst ignoring positive ones -catastrophising - exaggerating a minor setback so the entire event is a complete disaster 2. Disfunctional belief system arises through early experiences e.g. seeing parents unable to cope in stressful situation |
|
|
The Cognitive Model/Explanation of depression - AARON BECKS EXPLANATION The cognitive triad |
Beck also stated that there are 3 dysfunction belief systems that dominated depressed peoples thoughts = COGNITIVE TRIAD
- 1.negative views of the world, 2. about ones self and 3. the future
|
|
|
The Cognitive Model/Explanation of depression - AARON BECKS EXPLANATION Evaluation (3) |
1. "evidence based" e.g. ALLOY AND ABRAMSON -longitudinal study = evidence way of thinking can cause depression
|
|
|
Treatment of depression - based on Cognitive Approach -Description |
Cognitive Behavioural Therapy (CBT) - Form of psychotherapy
|
|
|
Treatment of depression - based on Cognitive Approach -Evaluation (6) |
1. ELKIN ET AL. 2. Fairy quick to see results so cheap in relation to e.g. dream analysis
4. Ethics -although consent and motivation - there are ethical issues as the therapist chooses what behaviours are acceptable and attempts to change the persons beliefs
6. May not be suitable for all people - severely depressed may not have motivation/suitable mind frame to participate |
|
|
Elkin, et. al. Method (2) |
- 250 participants with depression, assigned to one of 4 groups CBT, drug therapy, Interpersonal therapy (IPT), placebo group - 18 months, after treatment ended = follow up analysis carried out |
|
|
Elkin, et. al. Results / conclusions (3) |
1. Recoverey = 36% for CBT on a psychiatric rating scale for depression, simular for drugs 2. Long term (18 months) = CBT maintained improvement above drugs + placebo
|
|
|
Elkin, et. al. Aim |
To investigate the success of different treatments for depression
|
|
|
Brown, et. al. Aim |
To see if the level of self-esteem and the amount of social support available to a person can predict the risk of depression for up to a year after a stressful event
|
|
|
Brown, et. al. Method |
1. Study took place in Islington, North America 2. Participants = working class women with one child 3. Data collected using semi-structured interviews 1st interview - asked about self - esteem personal ties with partner, friends and relatives any psychiatric illness in past 12 months YEAR LATER 2nd interview - looked at stressful events in past year amount of social support psychiatric illness 303 gave 2nd interview - 400 to start |
|
|
Brown, et. al. Results / conclusion |
about half of women had experiences a severe event or major difficulty in 12 month 32 had on set depression 1/3 of these 32 had low self-esteem women who were married + had a severe life event = reduced risk of depression IF partner gave them support CONC - increased risk associated with low self esteem and lack of support, especially at time of crisis |
|
|
Brown, et. al. Evaluation (4) |
1. Reliability = checked using 21 women 11 were interviewed by 2 researchers (2 interviews, asked same q's) 10 were rated by a second person using tape recorders - inter-rater reliability was HIGH 2. Biased minimised Contacted all eligible women and then sample was randomly selected 3. Not generalizable Conducted on working class women with at least one child 4. Valid Used trained interviewers Interviews gave in depth, rich and detailed info |
|
|
Goldstein Evaluation (3) |
1. Valid Supported by other studies e.g. Angermeyer et. al. found pre-morbid history was a good predictor of outcome 2. Reliable Random sample selected and sent off = 0.8 agreeement Diagnosis using DSM was reliable Objective data - number and duration of stays in hospital = scientific 3. Not generalisable Issues with age limit of 45 - Studies have shown that about 9% of womens onset of schizophrenia is after the age of 45 relatively small sample (199) unrepresentive sample- people around New York and simular cultural background (Non- Hispanic White) |
|
|
Randrup and Munkvad Evaluation (4) |
1. Not generalisable Animal findings cannot generalise to humans 2. Validity Issue Only valid if it is true that excess dopamine is causing the symptoms of schizophrenia 3. Bias Observation carried out by one person, so researcher bias affects data 4. Researchers gained baseline measurement so can see the changes the amphetamines made to rats behaviour |
|
|
Rosenhan's "Being sane in insane places" Evaluation (5) |
1. Generalisability 12 hospitals in 5 different states = good Only in USA so whether findings would be same in other countries in undecided 2. Reliability With 8 people in 12 different hospitals, we can say study was replicated = reliable Pseudo- patients tried to be objective in observations (what its like to be labelled as insane) BUT judgement could have been influenced by emotions DSM has changed since study, so unlikely you can test for reliability 3. Valid Ecologically valid - carried out in actual hospitals, real staff who were unaware of study 4. Ethical Issues Staff did not know they were taking part in study (concent was not obtained) pseudopatients did say they heard voices , so there was deception 5. Practical Clinicians wouldn't expect individuals to present themselves as mentally ill no to be so, so wouldn't doubt symptoms |
|
|
What is Primary data?
|
Data observed or collected directly from first-hand experienced |
|
|
What is Secondary data?
|
Published data which is collected in the past by someone else, collected for another purpose |
|
|
Evaluation of Primary data Strengths (4) Weaknesses (4) |
Strengths 1. Gathered 1st hand for a specific purpose 2. You know it is a reliable source - can easily be replicated bc researcher knows how results were collected and analysed 3. More valid as results collected at time and conclusions drawn 4. If required, may be possible to obtain additional data Weaknesses 1. Starting from scratch so requires large population. Requires large volumes of data = (money, time, effort) 2. Kind of data collected may be collected to fit hypothesis 3. Restricted in participants, time and place - restricted in range and detail 4. More likely to exploit participants - pressure on participants to carry on/ undertake certain tasks |
|
|
Evaluation of Secondary data Strengths (4) Weaknesses (4) |
Strengths 1. Saves time and expense as uses existing data 2. Provides larger database - bigger range so generalisability possible 3. Less ethical issues, consent not an issue if published + on domain 4. Only way of studying past trends Weaknesses 1. Reliability and validity may be unknown - may be flawed cause of original errors e.g. subjectivity 2. Data may have been incorrectly interpreted e.g. because it was originally answering a differnt hypothesis 3. Data may be out of date - attitiudes change over time 4. Obtaining additional data is not possible |