![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
85 Cards in this Set
- Front
- Back
|
What is Clinical Psychology? |
The study of mental health and disorders.
Abnormal Psychology The study of behaviour that is regarded as"not normal" |
|
|
When Defining Clinical Psychology Include... |
|
|
|
What is Abnormality? |
Abnormality is behavior which is concidered to disrupt our expectations and can create a negative response: behaviour that is seen as bring not "normal" |
|
|
Statistical Infrequency Image |
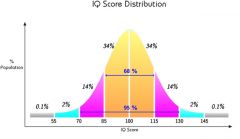
Definition of Abnormaility
|
|
|
Statistical Infrequency |
If the behavior is rare/infrequent within a population. Distribution curve used → behavior tail ends are abnormal whereas behavior in the middle is normal |
|
|
Evaluation of Statistical Infrequency |
|
|
|
Statistical Infrequency AO2 |
+ The determination of abnormality is based upon frequency and numbers, using quantitative analysis, which is more reliable. - The tests that are used to assess a particular characteristic, e.g. IQ, may not be valid - The 2% cut off point may not be applicable to other cultures where there isn't a normal distribution - The random nature of their statistical cut off point means there is no scope to account for how well an individual is coping |
|
|
Deviation from Social Norms |
When a persons behavior or beliefs are perceived as different to what is seen as acceptable and expected within a particular society they may be judged as 'abnormal' |
|
|
Deviation from Social Norms Image |
Definition of Abnormaility |
|
|
Evaluation of Deviation from Social Norms |
|
|
|
Deviation from social norms AO2 |
+ It allows the global nature of behavior to be assessed rather than relying on a specific symptom + The definition is in line with our common sense and everyday thinking of what constitutes abnormal behavior. - Social deviancy is not always negative. Some people are socially deviant because they have chosen our nonconformist lifestyle. It may be difficult to distinguish between someone who is eccentric and those who are abnormal - Behaviour deemed as normal in one society may be seen as abnormal in another → labeling someone abnormal inaccurately |
|
|
Common Features of Definitions of Abnormality |
|
|
|
Anti-Social Personality Disorders |
DSM-IV → A failure to conform to social norms with respect to lawful behaviors as indicated by repeatedly performing acts that are grounds for arrest
Socially unacceptable behavior with regards to the individuals context; culture, age, gender |
|
|
The statistical infrequency cut off point |
2.145% |
|
|
Failure to Function Adequately *Extension* → Alternative definition |
There's expectations for how people should live and contribute to society. If an individual cannot meet these expectations they may not be functioning adequately: this may be occurring due to the individual experiencing distress or discomfort. + This definition recognises that there may be degrees of normality and abnormality negative sign some of the criteria are based on social norms and thus may not be applied universally |
|
|
DSM-V |
DSM-V is a multi-axial diagnostic tool: it is a comprehensive manual that provides classifications of disorders. Classification of mental disorders involves taking sets of symptoms and putting them into categories. Diagnosis involves assessing the patients symptoms and deciding whether they meet the criteria for one or more mental disorders. |
|
|
DSM |
Diagnostic & Statistical Manual |
|
|
Diagnosing a patient with the DSM |
In the classification system, the disorders are listed along with a set of symptoms, all or some of which must be present for a specified period of time. When the set of abnormal symptoms are classified into a disorder, the individual can be diagnosed according to their symptoms.
Using axes to diagnose a patient allows them to be assessed more broadly, giving a more in depth picture. |
|
|
Multi-Axial Classification |
|
|
|
Revising DSM - Edition 5 |
- Some of the revisions are thought to lack empirical support - Inter-rater reliability is low from many disorders; several sections contain orderly written, confusing, or contradictory information |
|
|
DSM Supporting Points AO2 |
+ Lahey et al (2006) found that there was a good predictive validity in relation to their social and academic functioning over a six-year period for children diagnosed with ADHD. + Brown et al (1996) found that there was a 67% agreement rate for major depression, showing reasonable reliability. |
|
|
DSM Conflicting Research AO2 |
- Davidson and Neale (1994) thousand are variable reliability rate or different disorders, with 92% for psychosexual disorders, but its only 54% for somatoform disorders. - Rosenhan (1973) concluded that DSM-III was not valid, as hospital staff were unable to differentiate between initiatives who did have our mental disorder and those that did not. Hospital staff were easily fooled by pseudo-patients claiming to be experiencing one symptom of schizophrenia. - Casas (1995) found that many African-Americans do not like to share their personal information with people of a different race |
|
|
DSM Types of Reliability |
For classification systems to have inter-rater reliability different diagnosticians using the same system should arrive at the same diagnosis for the same individual. Test-Retest reliability can be said to occur when the same diagnosis an be replicated with the same patient after a period of time. |
|
|
DSM Reliability AO2 |
- Cooper (1983), the newest classification systems leave little room subjective judgements and thus the reliability of the diagnosis is high. - Nickhols et al compared the reliability of DSM-IV with the ICD-10 for children with eating disorders. ICD had a reliability rate of 36%, and the DSM 64% but only because 50% of the raters agreed they couldn't make a diagnosis. This shows neither have good inter-rater reliability for the diagnosis of eating disorders in children. |
|
|
DSM Validity |
Valid diagnosis means the classification of symptoms must actually show an underlying illness, leading to a suitable treatment and prognosis. |
|
|
DSM Validity AO2 |
+/- Andrews et al found good criterion validity on particular disorders when comparing DSM-IV with the ICD-10. They found good agreement on depression, general anxiety disorders and substance abuse. However, only moderate agreement was found on other anxiety disorders and poor agreement on post-traumatic stress disorder. |
|
|
Types of Validity |
|
|
|
DSM Cultural Issues |
DSM is used widely across different cultures. The potential impact of cultural issues on diagnosis raises a further validity problem for example through different perceptions of symptoms or attitudes to mental disorders across the cultures.
|
|
|
What is Schizophrenia? |
Schizophrenia is a mental illness that can affect the way someone thinks, feels and speaks (disruption in cognition, emotion, and language) to such a degree that they lose focus on reality
According to DSM-IV, the diagnosis of Schizophrenia requires at least 1-month duration of two or more positive symptoms, unless hallucinations or delusions are especially bizarre, in which case one alone suffices for diagnosis |
|
|
Features of Schizophrenia |
|
|
|
Negative Symptoms |
Involves loss of normal functioning e.g. reduced emotional responsivness and reduced quality of speech
Negative symptoms are associated with disruptions to normal emotions and behaviors |
|
|
Symptoms of Schizophrenia |
|
|
|
Explanations of Schizophrenia |
No single cause has been identified for schizophrenia; biological, behavioural and social research suggests a complex interplay between factors. For example, people might have an inherited tendency towards schizophrenia that is triggered by environmental circumstances.
|
|
|
The Dopamine Hypothesis Biological Explanation of Schizophrenia |
Chemical imbalance stemming from a problem with neurochemicals working differently in the brain; an increase of activity at dopamine synapses. The excess of the neurotransmitters in the brain increases feeling of paranoia and can cause hallucinations; theses are symptoms of schizophrenia. |
|
|
The Dopamine Hypothesis AO2 Biological Explanation of Schizophrenia |
+ The effectiveness of drugs that reduce the availability of dopamine support its role as implicated in the disorder. Neuroleptic drugs relive the symptoms of schizophrenia (such as hallucinations and delusions) by blocking the post-synaptic dopamine receptors; decreasing amounts of dopamine. + Lindtroem et al found that when L-DOPA (a chemical which is used by the brain to produce dopamine) was administered and traced using a radioactive label, it was taken up more quickly in schizophrenic patients than a control group. This indicates that the patients with schizophrenia were producing more dopamine then the control group.This indicates that the patients with schizophrenia were producing more dopamine than the control group. - Though aniti-psychotic drugs reduce dopamine availability in a very short time the effect on symptoms takes several weeks to appear, suggesting other factors involved - The dopamine hypothesis may explain positive symptoms but it would be expected that negative symptoms would be associated with low rather than high levels of dopamine. |
|
|
Genetic Factors Biological Explanation of Schizophrenia |
Schizophrenia or a vulnerability to the condition may run in families and thus may be inherited from parentd. It is thought that the presence of certain types of genetic mutations may be necessery for the disorder to be triggered. These genes can cause critical neural pathways in the brain to be disrupted or damaged. It is also possible that it is genetics that cause excess production to dopamine. The disorder is caused by a number of genes |
|
|
Genetic Factors AO2 Biological Explanation of Schizophrenia |
+ Family and twin study evidence, such as gottesman, gives support for a genetic component as concordance rates go up in direct relationship to the degree of relatedness. + Gottesman found an overall rate of 48% concordance for MZ twins and 17% for DZ twins, which indicates a genetic link. - However because concordance rates are not 100% for MZ twins it suggests other factors play a role too. - Also, MZ twins usually share their environments, so both genes and environment are similar: cause and effect cannot be concluded |
|
|
Structural Brain Differences Biological Explanation of Schizophrenia |
It has been suggested that schizophrenics have larger than normal ventricles which may have restricted the growth of brain development or allowed for tissue damage. Brain Metabolism levels are lower than average, resulting in poorly performed tasks. There is also less space occupied by neurons and they can also be disorganised. |
|
|
Structural Brain Differences AO2 Biological Explanation of Schizophrenia |
+ Zipursky et al found, using MRI techniques, that many schizophrenics have larger than normal ventricles, suggesting there is less space occupied by neurons. - The evidence for brain structural differences is only correlational e.g. enlarged ventricles may be a symptom and not a cause; Non-schizophrenics can also show the difference - Also structural differences are not found in all people with schizophrenia, non-schizophrenics can also show this difference so it cannot be used as a diagnostic tool. |
|
|
Social/Environmental Explanation of Schizophrenia |
Schizophrenics come from all types of social backgrounds, but most are clustered in the lower socio-economic groups and live in the poorest areas of cities. This has led to suggestions that social factors might be important. |
|
|
Social Causation Hypothesis Environmental Explanation of Schizophrenia |
Schizophrenia is more associated with cities than rural communities. People in declining inner-city areas and of lower social classes, are more likely to develop schizophrenia. Possibly due to increased stress from poor social conditions; degrading treatment from others, low levels of education and the unavailability of reward and opportunity. |
|
|
Social Causation Hypothesis AO2 Environmental Explanation of Schizophrenia |
+ The social causation hypothesis is less deterministic than for example the biological approach and implies that the condition could be treated if person's environment were to be improved. + Fearon et al estimated that there are four times as many incidences of schizophrenia in the African-Caribbean and black immigrant population as in the white indigenous population, and some studies suggest a higher figure - Warner has indicated that the relationship between incidence, recovery rates, and cultural and economic factors is more complex than a simple correspondence with socioeconomic deprivation.
|
|
|
Family Communication Environmental Explanation of Schizophrenia |
Some psychologists suggest that dysfunctional family relationships with 'abnormal' communications may play a part, creating highly stressful environments. However, this might be due to difficulties in coping with a member of the family who is mentally disturbed, not the reason for the illness. |
|
|
Twin Studies Studying Schizophrenia |
Twin studies involved comparing MZ and DZ twins to see what differences there are in the incidence of a certain characteristic, such as schizophrenia, which is indicated by the rate of concordance. If the disorder is genetic and based on nature it is believed that MZ twins would both show the characteristics and have high concordance, whereas there would be the same degree of similarity between MZ twins and DZ twins is schizophrenia is not genetically given but come from environmental factors. |
|
|
Twin Studies AO2 Studying Schizophrenia |
+ Twin studies involve the collection of quantitative data, which is objective and scientific + In twin studies there is a natural control for comparison, which provides evidence for the nature side of the debate, furthering psychological knowledge of the understanding of genetic influences on behavior and cognitive processes. - Twin studies do not show cause and effect, due to the lack of control over extraneous variables. The similarity between twins may not be due to genetics as they also share the same environment which could lead to a higher concordance rate. - Sample sizes may be limited, particularly in studying schizophrenia, as it is difficult to find a large sample of identical twins which possess the variable being studied. |
|
|
Interviews Studying Schizophrenia |
A type of survey which involves direct verbal questioning of the participant by the researcher about a topic, such as schizophrenia. The researcher also asks personal questions; demographic information |
|
|
Interviews AO2 Studying Schizophrenia |
+ Interviewers can be used to gather both quantitative and qualitative data which can enhance validity. + into new areas can gather in-depth information and can use follow-up questions when conducted in a semi-structured or unstructured way, which enhances validity. + Potential bias can be reduced by the use of independent interviewers or single-blind techniques.
- Interviews can be subjective if the interviewer is required to interpret the interviewees answers. - Interviews are much more time-consuming than questionnaires and thus likely to reduce the number of participants used, lowering generalisability. - Schizophrenic patients often find it hard to relate to others, so they may find it hard to respond coherently to an interview question. - Symptoms such as paranoia, loose association and disorganised thinking may have an effect on responses which will make them |
|
|
Examples of Interviews AO2 Studying Schizophrenia |
|
|
|
Closed & Open Questions |
Closed Questions: Require a fixed response which can be analysed quantitatively. + Enhances Validity & Easy to Analyse
Open Questions: Encourage extended answers and tend to generate qualitative data - Increased Bias & Hard to Analyse |
|
|
Unstructured Interviews |
Start with same opening questions and may have some prompts: Flexible format: Conducted with a open framework which allows for focused communication: There will be a schedule and areas to cover. |
|
|
Structured Interview |
Involve all the participants being asked the same questions in a set order: Standardization |
|
|
Semi-Structured Interview |
The interview has a standardized set of questions but the researcher can ask additional follow up questions → that can be changed and adapted to meet the objectives |
|
|
What is a Phobia? |
Phobias are categorised as an anxiety disorder. A phobia is defined as an irrational and intense fear of a specific object or situation. The fear experienced is intense and persistent; individuals are compelled to avoid the feared object or situation. There are three categories of phobia: specific, agoraphobia, and social phobias. Symptoms of phobias include excessive and out-of-proportion feeling of panic, dread, or terror even when there is no real danger. |
|
|
Types of Phobias |
|
|
|
Features of Phobias |
|
|
|
Explanations For Phobias Learning Theories |
In terms of classical conditioning a phobia may be learned through an association forming between fear and a particular object or situation. In terms of Social Learning Theory phobias may be learned through observation and imitation of role models.
|
|
|
Classical Conditioning As An Explanation for Phobias |
Phobias may be learned through an association forming between fear and a particular object or situation. An Originally neutral stimulus becomes associated with an unpleasant or traumatic experience and so becomes a fear-eliciting conditioned stimulus: e.g. Watson and Rayner
Rat causes no response
Noise creates fear
Rat+ Noise creates fear
After several pairings the Rat alone causes fear |
|
|
Mowrer's 'Two-Factor' Theory Phobia Explanation |
This theory explains the persistence of phobias: It suggests that phobias are acquired through classical conditioning but are maintained through operant conditioning: e.g. The avoidance of unpleasant phobic situation and the reduction in anxiety is negatively reinforced |
|
|
Operant Conditioning As An Explanation for Phobias |
Explains the maintenance of phobias; e.g. avoiding phobic stimuli acts as negative reinforcement due to the reduction in anxiety when the person adopts alternative strategies |
|
|
Social Learning Therory As An Explanation for Phobias |
Phobias develop via learning when a child observes and imitates a role model who shows fear or avoidance of objects or situations. Through modelling our behavior on role models that we identify with, we learn avoidance behavior and the fear of an object or situation:
For behavior to be learned and modelled:
Attention, Retention Motivation and Reproduction
|
|
|
Vicarious Learning As An Explanation for Phobias |
If The Observer sees the consequences of somebodies behavior, they will learn whether to imitate the behavior or not.
Vicarious Reinforcement explains how the observer is second-hand-reinforced - if they see an action being rewarded they are more likely to copy it. E.g. If the observer sees a model being rewarded for showing a fear response they will be more likely to imitate the behavior →Once the behavior is learn t may be reinforced or punished by its consequences |
|
|
Explanations For Phobias AO2 Learning Theories |
+ Watson and Rayners study of Little Albert supports the classical conditioning explanation as they demonstrated that a fear could be conditioned by paring a previously neutral stimulus (white rat) with and unconditioned stimulus (loud noise) to create anxiety at what became the conditioned stimulus (white rat). +/- classical conditioning and operant conditioning cannot explain why people have phobias of objects or situations that they have never experienced, however social learning theory can explain this. +/- DiNardo found 50% of dog phobics had been involved in a dog related incident that they found traumatic, however some people who had similar experiences with dogs did not develop a phobia: theory is not a complete explanation - Biological factors such as genetics and evolution are not considered
|
|
|
Psychoanalytic Theory Explanations For Phobias |
Suggests phobias are an expression of an unconscious conflict between the Id, ego and superego stemming from childhood (unresolved Oedipus and Electra complexes).
Phobias are caused by displacement of repressed unconscious anxiety onto harmless external objects; repressing the Id.
Freud believed that phobias are expressions of unacceptable wishes, fears and fantasies from their original, internal source onto some external object or situation that can be easily avoided. |
|
|
Psychoanalytic Theory AO2 Explanations For Phobias |
+ Freud found support for the psychodynamic explanation of displaced emotion with his study of Little Hans who was believed to have displaced his fear of his father onto horses. - Hans's phobia was more likely to have stemmed from witnessing a serious accident involving a horse and cart; the psychodynamic explanation ignores this much more obvious classical conditioning explanation - There is no empirical evidence to support Freud's theory directly. It is very difficult if not impossible to study the unconscious mind as it is an abstract concept and unfalsafiable |
|
|
Biological Approach Treatment |
Disorders are considered to stem from physical causes such as genetics and brain chemistry or structure. If it is assumed that psychological problems originate from a biological problem then the treatment for the condition will be biologically based. Biological treatments aim to treat the underlying physical causes of mental illness or remove the symptoms.
Treatments include:
→ Damaging or removing parts of the brain
→ Drug Treatments
→ Electric current through the brain |
|
|
Chemotherapy Example of Drugs Used Biological Approach Treatment
|
E.g. Chlorpromazine → Schizophrenia
E.g. Valium and Beta-Blockers → General Anxiety Disorders
E.g. Prozac → Depression and Phobias |
|
|
Biological Approach Treatment → Schizophrenia |
Anti-Psychotic drugs are used in the treatment of schizophrenia. They remove the symptoms, such as thought disorder, delusions, and hallucinations, but do not treat the underlying cause of the illness. These drugs can also cause unpleasant side affects; Though second-generation drugs have fewer less fatal side effects. Anti-Psychotics can be administered in tablet form, syrup or as an injection, in regards to individual preference.
Chemotherapy allows schizophrenics to live outside of mental institutions and become more independent and live successfully in society. |
|
|
Biological Approach Treatment → Schizophrenia |
- Drugs do not necessarily provide a long-term cure, they only alleviate the symptoms; When patients stop taking the drugs the symptoms can return - Drug treatments are only effective for positive symptoms so those with mainly negative symptoms are not really helped by chemotherapy. The treatment can leave as many as 60% of patients with symptoms that aren't affected by the drug +/- Drugs may be necessary as a means of protecting society at large from individuals who are dangerous. However this infringes upon the persons rights as the drugs are being used as a 'chemical-straitjacket' by controlling peoples behavior + Anti-Psychotic drugs have massively reduced the need for institutionalisation, enabling many schizophrenics to be cared for in the community; leading to independence and a better quality of life |
|
|
Social Approach Treatment |
Mental disorders can be triggered by factors in the environment.
Psychological problems are seen to stem from an interaction between the individual, their environment and social systems. Social approach treatments aim to enable the person to be independent, to function in society and form healthy relationships.
This Approach...
|
|
|
Social Approach Treatment → Schizophrenia |
Uses Community-based care to treat schizophrenia. The aim is to rehabilitate the patient, avoiding institutionalisation and ensure they can function as normally as possible in society. Support is provided so clients are able to deal with the environmental factors thought to trigger or make the condition worse. Patients are encouraged to make their own decisions & be independent.
Examples of Community Care:
|
|
|
Social Approach Treatment → Schizophrenia AO2 |
+ The treatment is more human than others as the client is empowered and able to take responsibility for themselves + Outcome research has shown that community care has the potential to enhance quality of life and perhaps reduce symptoms for patients with schizophrenia + Leff showed that patients with schizophrenia who were housed in long-term sheltered housing showed much lower levels of symptom severity than hospitalised patients +/- most patients find living in the community preferable to being in hospital, although others may find the situation overwhelming - There may be a lack of co-ordination between the different services involved, so patients may get different advice from different people |
|
|
Learning Approach Treatment |
Psychological disorders are the result of learning from the environment: learned via classical and operant conditioning. It is suggested that the behavior can be unlearned; treatments focus on learning more adaptive ways of responding → Counterconditioning
Treatments Include:
|
|
|
Systematic Desensitisation Learning Approach Treatment → Phobias |
Developed by Wolpe → based on reciprocal inhibition: 'One cannot be anxious and relaxed at the same time.'
This treatment is based on classical conditioning and is used for the treatment of phobias. It involves three stages:
|
|
|
Systematic Desensitisation AO2 Learning Approach Treatment → Phobias |
+ Systematic Desensitisation is more ethical than some other behavioral treatments such as flooding; patients can control the exposure and only move on when they're comfortable + Treatment is quick and cheep; only requires 6-12 sessions: psychoanalysis can be very time consuming, sometimes taking years = expensive + Watson and Rayner study shows that phobias can be learnt via conditioning and thus Systematic Desensitisation which involves counterconditioning should be effective in unlearning the phobia +/- Capafons et al showed that the treatment worked with fear of flying, which gives evidence of the success of the treatment with specific phobias. However, Craske and Barlow found between 60% and 80% of agoraphobics showed some improvement after treatment, but it was only slight and some clients relapsed completely after 6 months. - The treatment only focuses on observable symptoms, but the individual may experience other problems if there are underlying causes which have not been addressed |
|
|
Psychodynamic Approach Treatment
|
Mental disorders stem from the unconscious mind, due to repressed thought or emotions from childhood.
Freud developed psychoanalysis as a therapeutic method of uncovering unconscious issues at the root of disorders. Dream analysis is a technique that is employed within Psychoanalysis.
Freud believed that treatment should involve identifying the deeper, underlying unconscious mental causes of disorder, so that they can then be dealt with: do this by exploring the patient's past and linking it to their current symptoms: → Also used interpretation of symbols in dreams, dream reports, and free associations. |
|
|
→ Phobias Psychodynamic
Approach Treatment |
The source of phobias is believed to be material that has been repressed into the unconscious and emotions that have been displaced onto a particular object or situation.
Dream Analysis is used to interpret manifest content in symbols which then reveals the latent content to give insight into the unconscious causes, so the issue can be dealt with.
Freud believed that phobias and other psychological disorders are caused by unconscious desires. Individuals repress unacceptable desires. A phobia is a symbolic expression of these , as repression prevents the expression of the unconscious impulses and this leads to anxiety. |
|
|
Freud's Dream Theory |
Dream Work Purpose is to transform the forbidden wish into a non-threatening form, so reducing anxiety and allowing us to sleep in peace.
Displacement When someone or something is used as a replacement for an object or a person we are really concerned about.
Condensation When different factors are combined into one aspect of the manifest content.
Concrete Representation The expression of an abstract idea in a very concrete way
Secondary Elaboration Occurs when the unconscious mind strings together images into a logical succession which can further obscure the latent content
|
|
|
Psychodynamic Approach Treatment AO2 → Phobias |
- Hobson and McCarley argue that dreams are a purely physiological process; an accidental by-product of neural activity - they are random and meaningless. This therefore invalidates the treatment as dreams may hold no meaning - Dream analysis lacks credibility lacks credibility due to lack of scientific support: in contrast Hobson and McCarley's explanation is supported by empirical evidence = credible
- Dream Analysis is highly subjective as the interpretation of symbols is based on the therapists own opinion - Dream Analysis is unreliable as different therapists could draw different conclusions
+ Supported by Freud's case study of Little Hans |
|
|
Cognitive Approach Treatment |
Focuses on an individuals thoughts or cognitions as being the cause of abnormal behavior. Some People have Maladaptive Thinking: treatment aims to replace these with more adaptive ways and in tern change the person's feelings and behaviors.
Ellis believed that the existence of certain irrational beliefs reduces people's ability to withstand the effects of adverse events. |
|
|
Rational-Emotive Therapy Cognitive Approach Treatment → Maladaptive Thinking |
Disorders stem from maladaptive thinking. Ellis proposed the ABC model involving cognitive restructuring. A = Activating Event B = Clients Belief System C = The Consequence The client believes that A causes C, the therapist has to convince the client that actually B causes C. This is called Disputation and aims to rationalise the clients beliefs. When the client puts this to use, its leads to E, the outcome of the therapy (B+C no longer exists) |
|
|
Rational-Emotive Therapy AO2 Cognitive Approach Treatment → Maladaptive Thinking |
+ Anxious clients who are treated with RET improve more than those who receive no treatments. Hollon and Beck found that Cognitive therapy has been very effective for treating Depression. + Brandsma et al found that RET is especially effective with clients who feel guilty because of their own perceived inadequacies and who generally impose high demands on themselves
- Haaga and Davidson suggests there's problems in evaluating the effectiveness of RET because of the difficulty in defining and measuring 'irrational beliefs'. - Therapists using RET tend to be rather argumentative and direct, showing less concern for client's sensitivities. This has been particularly criticised by those who feel empathy is an important part of therapy. |
|
|
Primary Data |
Primary data means original data that has been collected by those who witnessed an event first-hand or who collected data themselves for for a specific purpose. Examples of primary data include raw data such as results from a questionnaire or a tally of behavior during an observation: e.g. Charlton et al |
|
|
Primary Data AO2 |
+ Primary data, especially gathered from scientific studies should involve less subjectivity as there is less need to interpret the findings than with secondary data + Primary data can be more reliable as the researcher knows the procedure and how the data was collected and thus they can replicate the study to check the results + Primary data may be more valid and relevant as it was collected for a specific purpose
- Primary data can be expensive to obtain as the researcher has to design the experiment from scratch and the research procedure may involve expensive equipment or other costly resources - It is more time consuming to gather primary data as the researcher has to plan the procedure, conduct the study and spend time analysing the findings. |
|
|
Secondary Data |
Secondary data is second-hand analysis of pre-existing primary data. It is the analysis of data that has been collected by someone else usually involving interpretation, evaluation, and commentary E.g. Gottesman and Bachrach et al. |
|
|
Secondary Data AO2 |
+Secondary data saves time and expense that would otherwise be spent collecting data. +In some cases secondary data may be the only way to conduct some research; examining the past. + Quicker to obtain as there is no need to develop the research materials such as questionnaires. +Data can be obtained cheaply and sometimes without cost such as using resource available on the internet as the data already exists + The data can be drawn from different sources which can enhance the validity due to the additional findings that can be included adding a richness to the data used.
-The data used may have been originally collected to meet a particular research purpous; and may not be fully applicable to the current research, lowering validity - There can be higher level of subjectivity with secondary data as the researcher may have to use their own interpretation to draw conclusions from the primary data. - The researcher cannot check that data so its reliability may be questioned. |