Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
81 Cards in this Set
- Front
- Back
|
What are some causes of denture induced oral lesions? (4)
|
1) ill fitting dentures
2) Lack of oral hygiene 3) Continuous wearing of the dentures 4) Some medications if the Pt is imunocompromised **Pt's often feel DDS exams are no longer needed if they wear dentures…this is not true.** |
|
|
What does the typical appointment for a denture Pt look like? (describe what you would do)
|
Review HH / Vitals
Inquire on fit of dentures/have Pt remove Perform IO/EO Examine dentures in front of PT (don't want to be accused of breaking them) Cleanse Dentures Identify homecare needs/education DDS Tx as needed |
|
|
Why does a denture Pt still need to brush the soft tissues?
|
To remove plaque and stiumlate the tissue.
*Always use a very soft brush.* |
|
|
A bridge is a __________ or _________ denture.
|
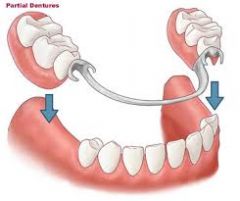
Fixed or Partial
|
|
|
What does the metal framework do with regard to the partial denture or bridge?
|
Makes it more stable
|
|
|
What does a "rest" sit on?
|

Existing structure to add support
|
|
|
What does a "clasp" do with regard to partials?
|
Wraps around a tooth to add stability
|
|
|
What are the 4 parts of a Complete Removable Denture?
|

1) Impression Surface (where the existing soft tissue lies) 2) Denture Border(rests in the vestibule)
3) Polished Surface (the pink polished surface) 4) Occlusal Surface |
|
|
An implant supported denture is a more/less common type of denture?
|
More Common!
It uses actual implants in the edentulous Pt to hold the denture in place |
|
|
An over denture is often used for a patient with….
|

Remaining tooth structure.
(could be existing teeth or roots remaining) |
|
|
If a patient has an over denture what sill needs to be done with the remaining tooth structure?
|
Still needs to be probed and examined for health.
Still need to scale those remaing structures too! |
|
|
What is the purpose for cleaning a prosthesis? (4)
|
1) Prevent irritation of oral tissue
2) Control Infection 3) Prevent Mouth Odor 4) Maintain Appearance (they will stain) |
|
|
What 3 deposits will show up on dentures?
|
Plaque, Calculus and Saliva!
(All of this will be on both sides of a denture. Calc especially so on the lower denture.) |
|
|
What types of things do I need to tell a Pt concerning the cleaning of their dentures?
|
Remove and brush after each meal. (if can't brush then rinse off)
Use denture cleaning products--Immersion is best w/denture detergent (avoid abrasives) Use a specially designed denture brush There are commercially available ultrasonic devices the Pt can purchase. |
|
|
Denture Cleansers need to be: (5 things)
|
Easy to use
Reasonably priced Effective at removing deposits Non-toxic Harmless to dental materials |
|
|
What can be the purpose of denture adhesive?
|

To fill the space when the tissues shrink as a result of healing.
*Be aware that food & plaque will stick to the adhesive and if not cleaned…will stink!* |
|
|
What is the procedure for a professional cleaning etc of complete/partial dentures?
|
1) Have Pt remove (unless they are unable then I should do it.)
2) Inspect for debris 3) Immerse in an ultrasonic cleaning solution 4) Rinse, inspect & polish-->just like typodont teeth 5) deliver to Pt |
|
|
What should always be done to avoid breakage of dentures when cleaning?
|

Fill the sink with water to avoid breakage in case you drop them. Also, always transport in a cup.
|
|
|
What are the advantages of cleaning by immersion? (5)
|
1) Solution reaches all surfaces
2) Minimize danger of dropping the appliance 3) Offers safe storage when not in the mouth 4) Aids person with limited dexterity 5) Immersion involves the least amount of handling/observation when distasteful! |
|
|
Salivary glands are classifed by their_________.
|
Location (Major or Minor)
|
|
|
In additional to their location, how else are salivary glands classified by?
|
The type of secretion…Serous, mucous or mixed.
|
|
|
What is the compositon of serous saliva?
|
Water, Enzymes, Salts & Organic Ions
|
|
|
What is the composition of Mucous Saliva?
|
Mucin
(Mucin is a glycoprotein constituent of mucus.) |
|
|
What are the major salivary glands?
|
Parotid Submandibular & Sublingual
*They give the most saliva and you want to check for any tenderness when palpating during the IOEO.* |
|
|
What duct is assocatted with the Parotid gland?
|
Stenson's duct
|
|
|
Which gland(s) is the Wharton's duct associated with?
|
Submandibular & Sublingual
|
|
|
Where is the Wharton's duct located?
|
Under the tongue on the floor of the mouth.
|
|
|
What portion of the total saliva comes from the Parotid gland? What is this fluid primarly comprised of?
|
25%
Serous fluid |
|
|
Which cranial nerve intervates the Parotid gland?
|
Glosopharyngeal (IX Nine)
|
|
|
Which gland produces 60% of the total salivary secretions? What is the fluid comprised primarly of?
|
Submandibular
The fluid is mixed but is predominatly serous |
|
|
What part of the facial cranial nerve impacts the submandibular gland?
|
The Chorda tympani of the facial nerve (VII 7)
|
|
|
What excreets the submandibular fluid?
|
The Wharton's duct.
|
|
|
How much of the total saliva output is released by the Sublingual gland?
What is the fluid primarly made up of? |
5%
Mixed secretions but primarily mucus. |
|
|
Which cranial nerve intervates the Sublingual Gland?
|
VII Facial Nerve….The same Chorda Tympani of the facial nerve intervates both the Sublingual & Submandibular glands.
|
|
|
What are the 3 locations of the minor salivary glands?
|
Labial minor Buccal minor & Palatal minor mucosas
|
|
|
What is primarily secreted from the minor salivary glands?
|
Mucous Secretions?
|
|
|
What is one other minor salivary gland, where is it located and what does it secrete?
|
von Ebner's gland, Located at the posterior of the tonge by the circumvalate papilla
Secetes ONLY Serous fluid! |
|
|
What causes the formation of the calcified stones which block the ducts?
|
The salts in the saliva
|
|
|
Since a blocked gland/duct causes pain and swelling; what is causing any infection that arrises?
|
An abundance of natural bacteria since the duct is backed up.
*It can cause infection or even a tumor could form.* |
|
|
How are salivary stones gotten rid of?
|
They either work themselves out OR they need to be excised.
**You could suggest the Pt increase the intake of fluids to flush it out, the Pt may also need antibiotics in response to any infection.* |
|
|
Mucositis is a condition associated w/radiation therapy. What is mucositis?
|
Inflammation & ulceration of the mucus membranes.
(aka apthous ulcer…everywhere) |
|
|
What is dyspgagia?
|
Difficulty swallowing…possibly due to a lack of saliva
|
|
|
Is Sjogren's (Show grens) Syndrome an autoimmune disease? If so, what is causing it?
|
Yes There is an abnormal # of antibodies in the blood
|
|
|
What is the difference between Primary Sjogrens & Secondary Sjogrens?
|
Primary: Inflammation of tear and salivary glands
Secondary: Inflamation of tear, salivary glands AND connective tissues |
|
|
What are some additional symptoms of Secondary Sjogren's Syndrome?
|
Rheumatoid arthritis, lupus & scleroderma
|
|
|
How is Sjogren's transmitted and who is most likely to "receive" it?
|
Its GENETIC in nature and 90% of those who get it are FEMALE
|
|
|
What can Sjogren's sometimes be associated with?
|
Juvenile diabetes
Thyroid disease |
|
|
What are some non oral symptoms of Sjorgen's?
|
Frequent Dry Cough
Difficulty Swalling Blurred vision or the sensation of burning Constipation Dry Skin Nasal Dryness |
|
|
What types of physicians might be included in the Tx of Sjogren's? Why?
|
Opthalmologist-->Dry Eyes
Rheumatologist-->Connective tissue disorder, arthritis |
|
|
What are some products to recommend for the Pt w/Xerostomia?
|
Biotene
Salivart (little pump spray that goes in the mouth) No alcohol Chewing gum (xylitol) or sugar free candy |
|
|
What meds might you see for a Pt with hyposalivation?
|
Pilocarpine 5-10 mg BID or Evoxac 30mg BID
(effects are 2-4 hours for each) |
|
|
What is an extrinsic stain? (Stain by locatin)
|

A stain that is outside the tooth surface
|
|
|
What is an intrinsic stain? (Stain by location)
|
A stain from within the tooth surface
|
|
|
Where does an Exogenous stain orginate?
|
Outside of the tooth
|
|
|
What is an exogenous stain the result of?
|
Exposure to environmental agents..the stain may be on the outside surface of the tooth (extrinsic) or become incorporated within the tooth structure (intrinsic).
|
|
|
What is an example of an exogenous stain source?
|

Coffee Tea Wine Smoking
|
|
|
Where is an endogenous stain orginate?
|
Comes from within the tooth
|
|
|
In terms of location (intrinsic or extrinsic) and by source; what would a metallic stain be classified as?
|
Exogenous (from outside of the body) &
Intrinsic (as it can stain dentinal tubules) |
|
|
What causes Orange/Yellow stain? What would be the classification?
|

Chromogenic Bacteria
Exogenous extrinsic-->comes from outside source & can be cleaned off. |
|
|
Where is Orange/Yellow stain usually located on the tooth surface?
|
Cervical 1/3 of anteriors-->adheres to the gingival margin.
|
|
|
What is Orange/Yellow stain associated with?
|
Poor Oral hygiene.
*Remember incisors get "self" cleaned by the act of eating. If this stain is present then Pt isn't cleaning very well.* |
|
|
What are Green Stains usually associated with?
|

An environmental metal-->metallic industry dust, perhaps from the work place
|
|
|
Where on the mouth is Green Stain usually found?
What is the classification of green stain? |

MX anteriors
Exogenous/Extrinsic |
|
|
Teeth with green stain are often ____________ (condition.)
In addition to the metallic dust, what is causing the green stain? |
Demineralized
Chromogenic bacteria, fungi and gingival hemorrhage. *Fungi has a higher acidity, since teeth become demineralized they are a "magnet" for this type of staining. |
|
|
Where is Black Line Stain usually located?
Which sex is more likely to experience it? |

Posterior linguals, along the gingival margin…often found in clean mouths.
Females |
|
|
What is often the cause of Black line stain?
|
Exposure to iron (ferric sulfide).
Can come from Pre-natal vitamins perhaps, or well water |
|
|
Since Black stain can come from well water or vitamins and can be polished right off, what is the stain classification?
|
Exogenous/ Extrinsic
**Remember the iron is constantly coming throug the saliva so the stain is "always" there.** |
|
|
How difficult is it to remove Black stain?
|
Very Easy-->remove with polishing cup.
**But because it flows through the saliva the stain will return right away.** |
|
|
What specificially causes the intrinsic stain of smoking tobacco?
|
The HEAT!
The heat is actually baking the enamel causing it to become yellow. |
|
|
What tool is good at removing the tar of tobacco stain?
|
Ultra Sonic!
*Otherwise, keep your instruments sharp!* |
|
|
What are 3 "reasons" to see endogenous intrinsic stains?
|
1) Pulpless teeth
2) Tetracycline Stain (Drug induced in offspring) 3) Developmental imperfections |
|
|
Review Nabors Probe on your own
|
Didn't have time to make questions
|
|
|
What is a Class 1 Furcation?
|
Slight root indention
|
|
|
What is a Class 2 Furcation?
|
1/2 way through
|
|
|
What is a Class 3 Furcation?
|
All the way through…but covered by Gingiva
|
|
|
What is a Class 4 Furcation?
|
All the way through & EXPOSED!
|
|
|
What constitutes a Class 1 perio Pt
(Like Class1 Lt or Class 2 Lt etc) |
No Attachment Loss
No bone loss (bone is 1.5-2.0mm from CEJ) |
|
|
What constitutes Class 2 perio Pt
(Like Class1 Lt or Class 2 Lt etc) |
10 places w/ 1-2 mm attachment loss
*Bone measures 1-2mm beyond the normal 2mm level** |
|
|
What constitutes a Class 3 perio Pt
(Like Class1 Lt or Class 2 Lt etc) |
10 places w/ 3-4 mm attachment loss
**Bone measures 3-4mm beyond the normal 2mm level** |
|
|
What constitutes a Class 4 perio Pt
(Like Class1 Lt or Class 2 Lt etc) |
10 places w/5-6 mm attachment loss
**Bone measures 5-6mm beyond the normal 2mm level** |
|
|
Review your Process Evals
|
Review the process Evals for:
Graceys Polishing Fluoride Tray vs Varnish Cleaning Prosthetic |