![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
63 Cards in this Set
- Front
- Back
|
What are the 4 knee projections? |
AP Lateral PA Tangential |
|
|
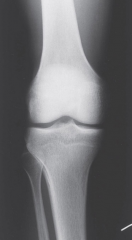
What can you see in AP view? |
Femorotibial joint, distal femur, and proximal tibia
Patella is obscured |
|
|
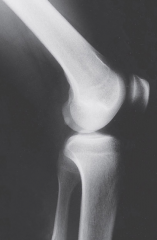
What can you see in Lateral View |
Patellofemoral joint, quads, suprapatellar bursa, patella shadow
|
|
|
What can you see in PA Axial of Intercondylar fossa
|
Shoes the fossa, posterior femoral condyles, tibial intercondylar eminence
|
|
|
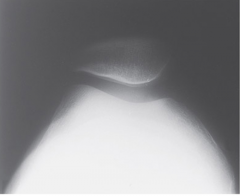
What can you see in Tangential (Sunrise) View |
Patellofemoral joint relationship |
|
|
What to assess on AP knee radiographs |
Patellar position Femorotibial joint space Long axes of femur and tibia |
|
|
What to asses in Lateral Knee view? |
Superimposed femoral condyles Patellar position Suprapatellar bursa (can see only if abnormal) Fabella |
|
|
What to assess in PA View? |
Tunnel appearance of the fossa Intercondylar eminences |
|
|
What to assess in Tangential View? |
Sulcus angle Congruence angle Articular surfaces |
|
|
What are CTs used for? |
Fragmentation (complex fx) and depression fracturess |
|
|
What are MRIs used for? |
Articular cartilage, menisci, ligament |
|
|
What are Bone scans for? |
Occult fractures and articular cartilage (very sensitive but inexact location) |
|
|
What are angiographs used for? |
Severe fractures and/or dislocations with associated vascular injury |
|
|
What are Decision rules? |
Help clinician to decide whether imaging is necessary |
|
|
What are the Ottawa Rules for Radiographs? |
•over55yo •Tendernessfibularhead •Isolatedtenderness of patella •Inabilityto flex knee to 90 •Inabilityto walk 4 steps |
|
|
What are the Pittsburgh Rules for Radiographs? |
•Blunttraumaor fall mechanism AND… •Ageunder 12 yo orover 50 yo AND/OR •Inabilitytowalk 4 weight-bearing steps |
|
|
When are Radiographs NOT needed? |
In a twisting knee injury when a patient can walk and no effusion is present |
|
|
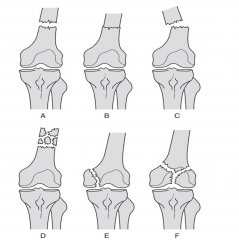
How are Knee fractures Classified? |
Near Femur -Supracondylar -Intercondylar -Condylar |
|
|
Describe Proximal Tibia fractures? |
Usually plateau fractures with the lateral plateau most commonly involved (non weight bearing!) |
|
|
What are the 2 types of patellar fractures? |
Fracture from direct blow and avulsion fracture (strong contraction of the quads) |
|
|
What are the types of Supracondylar fractures? |
Nondisplaced, impaccted, displaced, comminuted |
|
|
Describe Patellofemoral subluxation |
Chronic shown with hx or exam Radiographs needed for osteochondral frag, fractures, articular surfaces, and joint congruity MRI - articular surfaces CT - joint topography |
|
|
Describe Patella Baja |
abnormally low lying patella is associated with restricted TOM, crepitus and retropatellar pain |
|
|
What is Patella Alta? |
abnormallyhigh patella in relation to femur and may result in dislocation ofpatella. Note: a ruptured patellartendon may appear like patella alta. Pthx is the key |
|
|
What are the types of Articular Cartilage? |
Osteochondral Fractures Osteochondritis dissecans Spontaneous osteonecrosis |
|
|
Osteochondral fracture |
Fracture of the articular cartilage and the subchondral bone -Lat condyle MC often involved and are often sports related |
|
|
Osteochondritis dissecans |
Chondral injury in children and teens Medial Condyle MC |
|
|
Spontaneous Osteonecrosis |
Elderly females and is due to arteriole insufficiency Medial Condyle MC |
|
|
Describe knee discolations |
Femorotibia dislocation Rare occurrence that ruptures the cruciates and injures the collaterals, capsule and menisci |
|
|
Describe a Meniscal Tear |
Common in sports injuries Hx of clicking or locking (cannot fully extend) |
|
|
What is O'Donoghue's terrible triad? |
Medial Meniscus, Mcl and Medial capsule, and ACL T2 weighted MRI used to diagnose |
|
|
What is Pellegrini-Stieda |
Ossified MCL injury |
|
|
MCL vs LCL injuries |
MCL is more common |
|
|
Describe ACL injury
|
common with women 8x more likely to be injured Sports related 1 in 200,000/yr MOI: valgus and rotary forces |
|
|
Describe PCL injury |
More often due to contact injury, such as dashboard |
|
|
What are the Patellar-Tendon traction disorders |
Sinding-Larsen-johansson - proximal tendon Osgood-Schlatter - Distal tendon |
|
|
Degenerative conditions of the knee |
Present in radiographs in most people >50 treat patient not radiograph |
|
|
How does DJD appear? |
Dec joint space Sclerotic subchondral bone osteophyte formation at joint margins subchondral cyst formatoin varus/valgus deformities |
|
|
What can cause Functional Leg Length Discrepency |
Pelvic obliquity LumboSacral scoliosis Hip/knee flexion contractures Varus/Valgus deformities DJD ar ankles,knees hips Joint arthroplasty |
|
|
Knee Anomalies |
Genu Valgum - knock knees Genu Varum - bowlegs Genu recurvatum - hyperextended knees May develop in adult hood due to injruy or obesity and result in or from DJD |
|
|
AP Knee |
|
|
Lateral Knee
|
|

|
PA Axial (fossa/tunnel view) |
|
|
Tangential (Sunrise) View
|
|

|
Intercondylar Fossa |
|
|
A: Nondisplaced B: Impacted C: Displaced D: Comminuted E: Condylar F: Intercondylar |
|

|
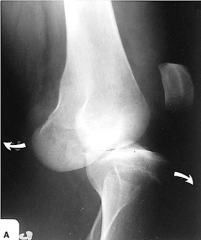
Tibial Plateau Fracture |
|
|
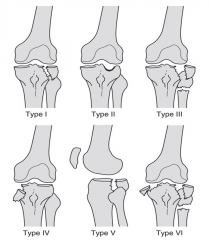
Hohl Classification of tibial Plateau Fractures |
|
|
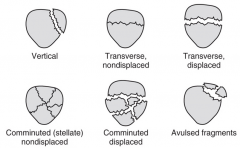
Vertical Transverse/Nondisplaced Transverse/Dsiplaced Comminuted/Nondisplaced Comminuted/Displaced Avulsed Fragments |
|

|
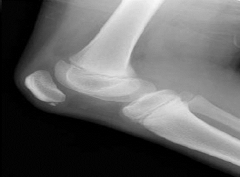
Patella Baja |
|

|
Patella Alta |
|

|
Osteocondral Fracture |
|

|
Spontaneous Osteonecrosis
|
|

|
Osteochondritis Dissecans
|
|

|
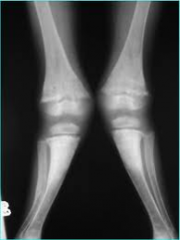
Bilateral Ostochondritis Dissecans |
|
|
Femoraltibial dislocation
|
|
|
Sinding-Larsen-Johansson |
|

|
Osgood-Schlatter |
|
|
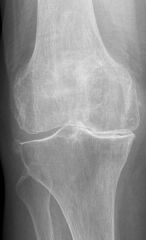
DJD in the knee |
|
|
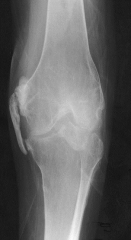
Pellegrini-Stieda - ossified MCL
|
|
|
Genu Valgum |
|

|
Genu Varum
|
|

|
Genu Recurvatum |