Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
240 Cards in this Set
- Front
- Back
|
Most common disease of the paranasal sinuses?
|
Inflammatory disease
|
|
|
What characterizes acute sinusitis?
|
Air-fluid levels
Foamy appearing sinus secretions |
|
|
What characterizes chronic sinusitis?
|
Mucoperiosteal thickening without bony expansion
Osseous thickening of the sinus walls |
|
|
MR findings in sinusitis?
|
High signal on T2WIs
BUT, desicated secretions in chronic sinusitis may not have signal |
|
|
Disease in the infundibulum of the maxillary ostium will result in:
|
Opacification of the maxillary sinus
|
|
|
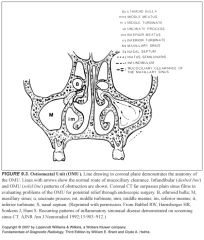
What structure is crucial for mucociliary drainage?
|
The ostiomeatal unit
|
|
|
What will happen if there is obstruction of the hiatus semilunaris (the middle meatus)?
|
Combined obstruction of the ipsilateral maxillary, anterior and middle ethmoid air cells, and the frontal sinus
|
|
|
What should you think about when you see opacification of the maxillary, anterior and middle ethmoid air cells and frontal sinuses?
|
You should try to identify the offending lesion within the hiatus semilunaris, rather than simply describing the presence of diffuse sinus disease.
|
|
|
Complications of sinusitis?
|
Inflammatory polyps, mucous retention cysts, mucoceles
Cavernous sinus thrombosis is the most important complication |
|
|
Why do inflammatory polyps form in the sinus?
|
Chronic inflammation leads to mucosal hyperplasia and redundancy
|
|
|
What is an antrochoanal polyp?
|
When a maxillary antral polyp expands to the point where it prolapses through the sinus ostium
|
|
|
What does an antrochoanal polyp look like on CT?
|
-Soft tissue mass extending from the maxillary sinus to fill the ipsilateral nasal cavity and nasopharynx
-Often the ostium of the maxillary sinus will be enlarged secondary to the mass effect of the polyp -Peripheral enhancement without any central enhancement |
|
|
Why is it important to differentiate a nasal polyp from a antrochoanal polyp?
|
Because if an antrochoanal polyp is snared and removed like a nasal polyp without regard for its antral stalk, it will recur
|
|
|
What is a mucous retention cyst?
|
Obstructed mucous gland within the mucosal lining
|
|
|
What do mucous retention cysts look like?
|
-Characteristic rounded appearance
-Measure one to several centimeters in diameter |
|
|
What is a mucocele?
|
-Similar to a retention cyst, but instead of a single mucous gland becoming obstructed, the entire sinus is obstructed
-Typically occurs because of a mass obstructing the draining sinus ostium |
|
|
What do mucoceles look like?
|
Frank expansion of the sinus with associated smooth sinus wall bony thinning and remodeling
|
|
|
Which sinus is most commonly affected by mucous retention cysts?
|
Maxillary
|
|
|
Which sinus is most commonly affected by mucoceles?
|
Frontal
|
|
|
What is an infected mucocele called?
|
A mucopyocele
|
|
|
What does an infected mucocele look like?
|
Like a mucocele with peripheral enhancement
|
|
|
Where do inverting papillomas tend to occur?
|
Almost exclusively on the lateral nasal wall
|
|
|
What is an inverted papilloma?
|
-Named based on their histologic appearance
-The neoplastic nasal epithelium inverts and grows into the underlying mucosa -NOT associated with allergy or infection |
|
|
How is an inverted papilloma treated?
|
It should be resected with wide mucosal margins
|
|
|
Why should inverted papillomas be resected?
|
They're associated with squamous cell carcinoma
|
|
|
What does an inverted papilloma look like?
|
-Enhancing mass centered in the middle meatus
-Local bony remodeling & ostiomeatal unit opacification -“cerebriform pattern” |
|
|
What should you think of in a teenage male with epistaxis?
|
Juvenile nasopharyngeal angiofibroma
|
|
|
Why is it super important to diagnose a JNA off of imaging?
|
Because life threatening hemorrhage can result if these things are biopsied or if limited resection is attempted
|
|
|
Is a JNA benign or malignant?
|
Benign tumor that can be locally aggressive
|
|
|
What tissue do JNAs arise from?
|
The fibrovascular stroma of the nasal wall adjacent to the sphenopalatine foramen
|
|
|
What do JNA’s look like?
|
-Location in the retromaxillary pterygopalatine fossa is a hallmark (if you see something in this location, think about JNA)
-They characteristically fill the nasopharynx and bow the posterior wall of the maxillary sinus forward -They enhance markedly which differentiates them from the rarer lymphangioma |
|
|
How are JNA’s managed?
|
NeuroIR often embolizes them before surgery
|
|
|
Symptoms of paranasal sinus squamous cell cancer?
|
-It is often clinically silent until it is quite advanced
-Early symptoms are related to obstructive sinusitis |
|
|
Imaging findings in paranasal sinus squamous cell cancer?
|
-Opacified sinus with associated bony wall destruction
-These findings are nonspecific and do not allow differentiation from non-Hodgkin’s lymphoma or a minor salivary gland malignancy |
|
|
Differential for opacified sinus with bony wall destruction?
|
-Squamous cell cancer
-Non-Hodgkin’s lymphoma -Minor salivary gland malignancy -Mucopyocele with osteomyelitis |
|
|
How does lymphoma of the paranasal sinuses present?
|
Constitutional symptoms with prominent hand and neck or systemic adenopathy, especially in a child or young adult
|
|
|
Where are the minor salivary glands located?
|
Throughout the upper aerodigestive tract but are most highly concentrated in the palate
|
|
|
Are minor salivary gland tumors usually benign or malignant?
|
Malignant
|
|
|
Are parotid salivary gland tumors usually benign or malignant?
|
Benign
|
|
|
What types of cancers arise from salivary glands?
|
Adenoid cystic carcinoma
Adenocarcinoma Mucoepidermoid carcinoma |
|
|
What is an esthesioneuroblastoma?
|
A tumor that arises from neurosensory receptor cells of the olfactory nerve and mucosa
|
|
|
Where are esthesioneuroblastomas located?
|
-Anywhere from the cribiform plate to the turbinates
-Usually high in the nasal vault -Involvement of the cribiform plate with extension into the anterior cranial fossa is not uncommon |
|
|
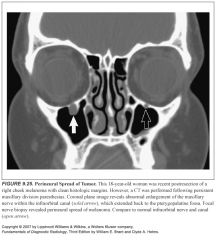
How can you tell a sinonasal tumor apart from the associated obstructed sinus secretions?
|
-Heavily T2W images help because sinus secretions will be brighter than the malignancy
-The malignancy is often isointense with respect to muscle |
|
|
Name the five bones of the skull base:
|
Ethmoid
Sphenoid Occipital Temporal Frontal |
|
|
Are most skull bases lesions primary or metastatic?
|
Metastatic
|
|
|
Three most common primary tumors of the skull base?
|
Chordoma
Chondrosarcoma Osteogenic sarcoma |
|
|
What is a chordoma?
|
It is a neoplasm that arises from remnants of the primitive notochord
|
|
|
Where can chordomas be found?
|
Anywhere along the craniospinal axis
35% involve the clivus 50% involve the sacrum 15% involve the vertebral bodies |
|
|
How do chordomas classically present in the skull base?
|
-As a destructive midline lesion of the clivus
-It has a predilection for the sphenooccipital synchondrosis -Sagittal images show tumor “thumb” indenting pons -Calcification, hemorrhage, retained bony fragments, mucoid material give tumor heterogeneous appearance |
|
|
What is a chondrosarcoma?
|
Malignant tumor that develops from cartilage
|
|
|
Why would the skull base be prone to chondrosarcoma?
|
It was preformed from cartilage
|
|
|
Where do chondrosarcomas like to form in the skull base?
|
They prefer the petroclival junction
|
|
|
Risk factors for osteosarcoma of the skull base?
|
Prior radiation or Paget’s disease
|
|
|
So, a midline clival destructive lesion=
And a paraclival destructive lesion= |
=Chordoma
=Chondrosarcoma |
|
|
What CT characteristics would tell you that a clival lesion might be fibrous dysplasia?
|
-Smooth, gound-glass appearance
-No bony destruction |
|
|
What CT characteristics would tell you that a clival lesion might be Paget’s?
|
-Trabecular coarsening
-No bony destruction |
|
|
Most common lesion of the jugular foramen?
|
Paraganglioma
|
|
|
Presenting symptoms of a jugular foramen paraganglioma?
|
Tinnitus, conductive hearing loss
|
|
|
MR findings in paraganglioma?
|
-“salt and pepper” signal due to numerous flow voids
-Widening of the jugular foramen |
|
|
What things pass through the jugular foramen?
|
-Cranial nerves IX, X, XI (remember the jug?)
-Sigmoid sinus -Posterior meningeal artery |
|
|
What lesions arise from the cranial nerves passing through the jugular foramen?
|
CNIX: schwannoma
CNX: paragangliomas CNXI: schwannoma |
|
|
What is a cholesteatoma?
|
Epidermoid cyst composed of desquamating stratified squamous epithelium
|
|
|
Why do cholesteatomas enlarge?
|
Because of progressive accumulation of epithelial debris within their lumen
|
|
|
How do congenital cholesteatomas develop?
|
From epithelial rests within or adjacent to the temporal bone
|
|
|
What specific tissue gives rise to acquired cholesteatomas?
|
The stratified squamous epithelium of the tympanic membrane
|
|
|
Imaging findings in cholesteatomas?
|
-Soft tissue mass in the middle ear cavity
-Typically has associated bony erosion -Classic: soft tissue in the middle ear with subtle bony erosion of the scutum and medial displacement of the ossicles |
|
|
What is the name of the space that is the superior recess of the tympanic membrane in the middle ear?
|
Prussak space
|
|
|
What foramen does the facial nerve exit through inferiorly in the middle ear?
|
The stylomastoid foramen
|
|
|
The stapes connects to which window?
|
The oval window
|
|
|
What's the name of the bone that covers the top of the middle and inner ear?
|
Tegmen tympani
|
|
|
Bony prominence that connects to the top part of the tympanic membrane?
|
Scutum
|
|
|
Why is the upper part of the tympanic membrane more prone to cholesteatomas?
|
Because it retracts easily
|
|
|
How can you differentiate otitis media from a cholesteatoma?
|
You can’t; they have similar densities
|
|
|
What does the ENT want to know about a cholesteatoma when he orders a CT?
|
-How big it is
-The status of the ossicles, the labyrinth, the tegmen, and the facial nerve. |
|
|
What is a cholesterol granuloma?
|
-Type of granulation tissue that may involve the petrous apex
-These lesions represent petrous apex air cells that have become partially obstructed and are filled with cholesterol debris and hemorrhagic fluid |
|
|
What do cholesterol granulomas of the petrous apex look like on MR?
|
They are characteristically high signal on both T1 and T2
|
|
|
Differential for opacified petrous apex?
|
Retained fluid secretions
Petrous apicitis Nonaerated petrous apex |
|
|
Differentiating feature of retained fluid secretions in the petrous apex?
|
-Parallels signal intensity of fluid
-Dark T1, bright T2, no enhancement |
|
|
Differentiating feature of petrous apicitis?
|
-Parallels signal intensity of an abscess
-Dark T1, bright T2, ring enhancement |
|
|
Differentiating feature of a nonaerated petrous apex?
|
-Parallels signal intensity of fatty bone marrow
-Bright T1, dark T2, no enhancement |
|
|
Are pediatric neck masses more likely benign or malignant?
What types of cancers present this way? |
-Benign congenital or inflammatory lesions
-If it’s cancer, it’s likely lymphoma (Burkitt lymphoma if rapid growth is noted) or rhabdomyosarcoma |
|
|
Are adult neck masses more likely benign or malignant?
|
Malignant, except thyroid lesions
|
|
|
What are the borders of the nasopharynx?
|
-Inferior: hard and soft palates
-Posterior: pharyngeal constrictor muscles -Anterior: nasal choana |
|
|
What separates the oral cavity and the oropharynx?
|
The circumvallate papillae, tonsillar pillars, and the soft palate
|
|
|
Can you name the seven spaces in the deep cervical fascia?
|
Superficial mucosal
Parapharyngeal Carotid Parotid Masticator Retropharyngeal Prevertebral |
|
|
Why are the deep cervical fascial spaces important?
|
Because if you know which space a lesion is in, and you know what normally lives in that space, you can figure out what sort of lesion it is!
|
|
|
What is in the deep cervical fascia mucosal space?
|
Squamous mucosa
Lymphoid tissue Minor salivary glands |
|
|
What is in the deep cervical fascia parapharyngeal space?
|
-Fat
-Trigeminal nerve (V3) -Internal maxillary artery -Ascending pharyngeal artery |
|
|
What is in the deep cervical fascia parotid space?
|
-Parotid gland
-Intraparotid lymph nodes -Facial nerve (7) -External carotid artery -Retromandibular vein |
|
|
What is normally in the carotid space?
|
-Cranial nerves IX, X, XI, XII
-Sympathetic nerves -Jugular chain nodes -Carotid artery -Jugular vein |
|
|
What structures are in the masticator space?
|
-Muscles of mastication
-Ramus and body of the mandible -Inferior alveolar nerve |
|
|
What structures are in the retropharyngeal space?
|
-Lymph nodes (lateral and medial retropharyngeal)
-Fat |
|
|
What structures are in the prevertebral space?
|
-Cervical vertebrae
-Prevertebral muscles -Paraspinal muscles -Phrenic nerve |
|
|
What is the pharyngobasilar fascia?
|
-The aponeurosis of the superior pharyngeal constrictor muscles, which insets into the skull base
-This tough fascia separates the mucosal space from the surrounding parapharyngeal space |
|
|
What are the most common benign lesions of the mucosal space?
|
Tornwaldt cysts and minor salivary gland lesions
|
|
|
What is a Tornwaldt cyst?
|
-Thought to be remnants of notochordal tissue
-1-2% in normal pts |
|
|
What do Tornwaldt cysts look like?
|
-Midline
-High T2 signal |
|
|
What does a pleomorphic adenoma look like?
|
Well circumscribed, rounded lesions that have high signal intensity on T2
|
|
|
What are the three most common malignancies of the mucosal space?
|
-Squamous cell ca.
-Non-Hodgkin lymphoma -Minor salivary gland neoplasms -Unfortunately, these all appear similar on CT and MR |
|
|
Imaging findings in mucosal space cancers?
|
-Mass effect, often associated with lateral compression or obliteration of the parapharyngeal space, followed by invasion of the skull base
An early triad consists of: -Superficial nasopharyngeal mucosal asymmetry -Ipsilateral retropharyngeal adenopathy -Mastoid opacification(early warning sign) |
|
|
What does mastoid opacification indicate?
|
-Dysfunction of the eustachian tube, frequently the result of tumor invasion of the tensor veli palatini muscles
-This findings should cause you to carefully evaluate the mucosa of the nasopharynx |
|
|
Which MR sequences are most helpful in evaluating for cancer of the nasopharynx?
|
Fat suppressed T2 and contrast enhanced sequences
|
|
|
What tumor of the mucosal space has a propensity for perineural invasion?
|
Adenoid cystic carcinoma
|
|
|
What makes nasopharyngeal carcinoma different from regular squamous cell carcinoma?
|
-It is a particular variant of squamous cell that has unique features
-Much more common in Asian countries -Not associated with smoking or alcohol -Associated with Epstein Barr virus |
|
|
What would make you worry that mucosal lesion is a lymphoma?
|
-Systemic manifestations
-Bulky supraclavicular and mediastinal adenopathy -Splenomegaly |
|
|
What are the cranio-caudal borders of the parapharyngeal space?
|
It extends from the skull base to the submandibular gland
|
|
|
What spaces border the parapharyngeal space?
|
Medial: mucosal space
Lateral: parotid Anterior: masticator Posterior: carotid |
|
|
What is the stylomandibular notch?
|
Angle that the styloid makes with the mandible
|
|
|
Masses in the carotid space will do what to the stylomandibular notch?
|
They will narrow it (because they displace the styloid anteriorly)
|
|
|
Which internal jugular vein is usually larger?
|
The right
|
|
|
What cells do paragangliomas arise from?
|
Neural crest cells
|
|
|
What are the different types of paragangliomas?
|
-Carotid body tumors (at the carotid bifurcation)
-Glomus vagale (at the vagus nerve ganglion) -Glomus jugulare (along the jugular ganglion of the vagus nerve) -Glomus tympanicum (Arnold and Jacobson nerves in the middle ear) |
|
|
Symptoms of paraganglioma?
|
-Painless, slowly progressive neck mass
-Pulsatile, may have associated bruit -Because they are in the carotid space, they are often associated with slowly progressive cranial neuropathies |
|
|
What should you look for if you see a paraganglioma?
|
More paragangliomas, they are often multiple (5-10%)
|
|
|
Why does neuroIR get involved in the management of paragangliomas?
|
They do pre-op embolizations, reducing blood loss during surgery
|
|
|
Imaging findings in paragangliomas and schwannomas?
|
-Both are densely enhancing, and typically indistinguishable
-Paragangliomas have lots of flow voids, “salt and pepper” -Schwannomas usually do not demonstrate flow voids and can be cystic BUT very vascular schwannomas may have flow voids |
|
|
Describe schwannomas:
|
-Arise from the nerve sheath covering
-Do not infiltrate the substance of the nerve -May occasionally show cystic change |
|
|
How do neurofibromas look different from schwannomas?
|
-They are not encapsulated
-They often involve multiple peripheral nerves -They permeate the substance of the nerve fibers -They have a characteristic low intensity center on T1 |
|
|
Most common malignancy of the carotid space?
|
Nodal metastases
|
|
|
How would a mass in the deep lobe of the parotid gland deviate the parapharyngeal space?
|
Medially
|
|
|
How would a mass in the parotid space deviate the styloid process?
|
Posteriorly , widening the stylomastoid foramen
|
|
|
Most common parotid gland tumor?
|
Mixed cell tumors (pleomorphic adenomas)
|
|
|
Second most common parotid gland tumor?
|
Warthin tumors (benign)
|
|
|
Can we tell benign from malignant parotid tumors?
|
No, but pleomorphic adenomas have characteristic features
|
|
|
What do pleomorphic adenomas look like?
|
-Well circumscribed
-Very bright on T2 -Heterogeneous enhancement |
|
|
What characteristics would be concerning for parotid malignancy?
|
-Tumor homogeneity
-Indistinct margins -Indistinct signal intensity -Infiltration into deep neck structures -Involvement of the facial nerve |
|
|
How often are Warthin tumors multiple?
|
10%
|
|
|
What is thought to cause Parotid cysts?
|
Partial obstruction of the salivary ducts by surrounding lymphocytic infiltration
|
|
|
What pts are prone to getting parotid cysts?
|
AIDS and collagen vascular disease pts
|
|
|
Muscles of mastication?
|
Temporalis
Medial pterygoid Lateral pterygoid Masseter |
|
|
Where are accessory parotid glands found?
|
-Along the anterior surface of the masseter
-These can be mistaken for a mass |
|
|
How could tumor spread from the masticator space into the cavernous sinus?
|
It can spread along the third division of the trigeminal nerve, though the foramen ovale
|
|
|
What spaces does the retropharyngeal space lie between?
|
The mucosal space and the prevertebral space
|
|
|
How can you tell a mass is in the retropharyngeal space, and not in the prevertebral or mucosal spaces?
|
It will displace the prevertebral muscles posteriorly
|
|
|
The lateral retropharyngeal nodes are also known as:
|
The nodes of Rouviere
|
|
|
Should you see lateral retropharyngeal nodes normally?
|
-Yes if a patient is younger than 30
-If they’re older than 30, you should be suspicious |
|
|
How can you tell an abscess from cellulitis on MR?
|
-An abscess will demonstrate a rim of contrast enhancement surrounding a liquefied center.
-Cellulitis won’t -Both are isointense to muscle on T1 and bright on T2 |
|
|
What processes are seen in the prevertebral space?
|
Anything involving the cervical vertebrae (tumor, osteo)
|
|
|
What do lymphangiomas and hemangiomas look like on MR?
|
-They look similar
-Increased signal on T2 -Infiltrative |
|
|
How can you tell a hemangioma apart from a lymphangioma?
|
-Hemangiomas can have phleboliths on CT
-Lymphangiomas tend to heterogeneous signal with evidence of blood degradation products |
|
|
Which diseases like to spread perineurally?
|
Fungal infections, squamous cell ca., adenoid cystic carcinoma
|
|
|
What is the highest node in the jugular chain called?
|
The jugulodigastric lymph node
|
|
|
Where is the jugulodigastric node located?
|
-Where the posterior belly of the digastric muscle crosses the chain, near the level of the hyoid bone
-Immediately posterior to the submandibular gland |
|
|
What nodal diameters are considered abnormal?
|
-The jugulodigastric node and submandibylar nodes may normally measure up to 1.5cm in diameter
-All other nodes of the head and neck are considered abnormal if larger than 1 cm |
|
|
What features of a lymph node suggest malignancy?
|
-Peripheral nodal enhancement with central necrosis
-Extracapsular spread with infiltration of adjacent tissues -Matted conglomerate mass of nodes BUT the above features are also seen in infection—you cannot tell malignancy apart from infection. Clinical history's super-important there. -A round shape without a normal fatty hilum suggests neoplastic infiltration |
|
|
What do normal lymph nodes look like on MR?
|
They have homogeneous signal on all sequences
|
|
|
What to optic nerve gliomas look like?
|
-Enlarged optic nerve sheath complex
-May be tubular, fusiform, or eccentric with kinking -Some have extensive associated thickening of the perioptic meninges (termed arachnoidal hyperplasia or gliomatosis) |
|
|
Optic nerve gliomas are associated with:
|
Neurofibromatosis type 1, particularly when there are bilateral optic nerve gliomas
|
|
|
What are optic sheath meningiomas?
|
They arise from hemangioendothelial cells of the arachnoid layer of the optic nerve sheath
|
|
|
What do metastatic lymph nodes look like on MR?
|
Any heterogeneity in signal, especially in the presence of cystic change or necrosis, is consistent with metastasis
|
|
|
The extraconal and intraconal spaces are contained in what space?
|
The retrobulbar space
|
|
|
What surrounds the optic nerve?
|
-The optic nerve sheath complex
-Composed of CSF surrounded by leptomeninges -The optic nerve is an extension of the brain |
|
|
Most common lesions of the optic nerve sheath complex?
|
Optic nerve gliomas and optic sheath meningiomas
|
|
|
What do optic sheath meningiomas look like? How can you tell them apart from optic nerve gliomas?
|
-They assume a circular configuration
-They grow in a linear fashion along the optic nerve -They demonstrate a characteristic “tram track” pattern of linear contrast enhancement because the nerve sheath enhances rather than the nerve itself -In contrast to optic nerve gliomas, meningiomas may invade and grow through the dura, resulting in an irregular and asymmetric appearance. -Optic nerve sheath meningiomas may extensively calcify, whereas optic nerve gliomas rarely have any calcification. |
|
|
What things might look like an optic nerve sheath meningioma?
|
-Infiltrates from sarcoid, leukemia, or lymphoma
-These may have “tram track” enhancement -Optic neuritis has abnormal T2 hyperintensity and contrast enhancement |
|
|
What vascular lesions are common to the orbit?
|
-Capillary hemangiomas
-Lymphangiomas -Cavernous hemangiomas |
|
|
Describe orbital capillary hemangiomas: What do they look like? Who gets them?
|
-Develop in infants
-May grow rapidly in size -Typically plateau during the first year or two then spontaneously regress -Infiltrative soft tissue complex -Multiple vascular flow voids |
|
|
Describe orbital lymphangiomas:
|
-One of the most common orbital tumors of childhood
-Occur in children 3-15 years -Noted by their propensity to bleed -An acute hemorrhage can result in proptosis |
|
|
What do orbital lymphangiomas look like?
|
MR reveals multiloculated, lobular mass with characteristic signal heterogeneity caused by blood degradation products (this distinguishes them from capillary hemangiomas)
|
|
|
Describe orbital cavernous hemangiomas: What do they look like?
|
-One of the most common orbital masses in adults
-Shaply circumscribed, rounded mass -Diffusely enhance, sometimes mottled apearance |
|
|
What does an orbital venous varix look like?
|
-Enormously dilated vein
-Characterized by marked change in size with Valsalva maneuver |
|
|
What would cause enlargement of the superior ophthalmic vein?
|
-Cavernous sinus thrombosis
-Cavernous-carotid fistulas |
|
|
How do patients with cavernous-carotid fistulas present?
|
Pulsating exophthalmos and bruit
|
|
|
Types of carotid-cavernous fistulas?
|
-Direct or indirect
-Spontaneous or posttraumatic |
|
|
What are the three most common orbital masses in adults (in order of prevalence)?
|
-Pseudotumor
-Cavernous hemangioma -Lymphoma |
|
|
What is pseudotumor of the orbit?
|
-Long name=idiopathic inflammatory pseudotumor
-Most common cause of an intraorbital mass in adults -Poorly understood -Inflammatory lymphocytic infiltrate around the orbit |
|
|
How do pseudotumor present?
|
-Rapidly developing painful proptosis
-Chemosis—swelling of the conjunctiva -Ophthalmoplegia |
|
|
How does lymphoma of the orbit present clinically?
|
Painless proptosis
|
|
|
What do orbital pseudotumor and lymphoma look like?
|
-They can look exactly the same (one will be painfull, the other painless)
-Diffusely infiltrating lesions involving and extending into any retrobulbar structures -It is suggested that T2 hypointensity is suggestive of pseudotumor -Infiltrating lesions do NOT enlarge the tendinous attachments of the extraocular muscles while pseudotumor does. |
|
|
What do you have to add to the differential if you see a diffusely infiltrative mass anywhere in the head and neck region in a child?
|
Rhabdomyosarcoma
|
|
|
What does thyroid ophthalmopathy look like?
|
-Unilateral or bilateral proptosis
-Inflammatory infiltration of the orbital muscles and orbital connective tissues -Enlargement of the extraocular muscles with sparing of the tendinous attachments to the globe -80% have bilateral extraocular muscle involvement In some cases, the extraocular muscles are notmal and exophthalmos is caused by increased retrobulbar fat. |
|
|
Which extraocular muscles are involved with Graves ophthalmopathy?
|
"IM SLOW"
Inferior rectus Medial rectus Superior rectus Lateral rectus |
|
|
What things are in the extraconal space?
|
-Fat
-Lacrimal gland |
|
|
What kinds of lacrimal gland neoplasms are there?
|
Epithelial
-Benign mixed-cell tumor -Adenoid cystic carcinoma Lymphoid -Lymphoma -Pseudotumor |
|
|
What does a lacrimal gland dermoid look like?
|
A mass with a fat-fluid level
|
|
|
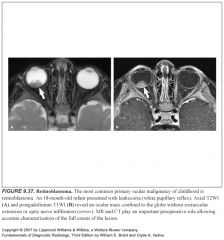
How does retinoblastoma present?
|
Leukocoria
|
|
|
What does retinoblastoma look like?
|
Calcified ocular mass
|
|
|
Most common cause of a neck mass in a child?
|
Thyroglossal duct cyst
|
|
|
Where does the thyroglossal duct originate?
|
The foramen cecum at the base of the tongue
|
|
|
When does the thyroglossal duct normally involute?
|
-8-10 weeks of gestation
-Any portion that fails to involute may give rise to a cyst or sinus tract -Thyroid glandular tissue can arrest anywhere along the course of the thyroglossal duct, giving rise to ectopic thyroid tissue |
|
|
What percent of thyroglossal duct cysts are midline?
|
75%
|
|
|
Where are most thyroglossal duct cysts located cranio-caudally?
|
At or below the level of the hyoid bone
|
|
|
Why are thyroglossal duct cysts treated surgically?
|
Because they tend to get infected
|
|
|
Why is it so important to determine the full extent of the thyroglossal duct cyst before surgery?
|
Because they tend to recur if incompletely resected
|
|
|
What do thyroglossal duct cysts look like?
|
-Cystic masses with a uniformly thin peripheral rim of capsular enhancement
-Occasional septations |
|
|
Differential for a suspected thyroglossal duct cyst?
|
-Necrotic anterior cervical nodes
-Thrombosed anterior jugular vein -Abscess -Obstructed laryngocele |
|
|
What is a laryngocele?
|
-The laryngeal ventricle separates the false and true cords and anteriorly ends in a blind pouch called the appendix
-A laryngocele develops are a consequence of chronically increased intraglottic pressure (musicians playing wind instruments, glass blowers, etc.) |
|
|
Where is an internal laryngocele located?
|
They are confined to the larynx
|
|
|
Where is an external laryngocele located?
|
-They protrude above the thyroid cartilage and through the thyrohyoid membrane
-These typically present as a lateral neck mass near the hyoid bone |
|
|
What should you think about if you see a laryngocele in a person that doesn’t have any predisposing factors?
|
You should be suspicious for an underlying neoplasm obstructing the laryngeal ventricle
|
|
|
Which branchial cleft gives rise to the most abnormalities?
|
The second
|
|
|
Where is the second branchial cleft located?
|
-It begins at the base of the tonsillar fossa and extends between the internal and external carotid arteries
-It is anterior to the middle portion of the sternocleidomastoid muscle and lateral to the internal jugular vein at the level of the carotid bifurcation |
|
|
What do branchial cleft cysts look like?
|
-Well-circumscribed cystic lesions
-Wall thickening, irregularity and enhancement are related to active or prior infections |
|
|
Branchial cleft cysts can be hyper and hypointense on T1, why?
|
The signal is related to proteinaceous cyst contents
|
|
|
Types of lymphangiomas?
|
-Capillary—composed of capillary sized thin walled vessels
-Cavernous—moderatly dilated lymphatics with fibrous adventitia -Cystic hygromas—enormously dilated lymphatic channels |
|
|
How are lymphangiomas formed?
|
-If primitive lymphatic sacs fail to communicate with the venous system, they dilate as they accumulate lymphatic fluid
-Thus, lymphangiomas represent sequestrations of the primitive embryonic lymph sacs -Extensive defects in the lymphovenous communication are incompatible with life and result in fetal hydrops |
|
|
What syndromes are associated with cystic hygromas?
|
Turners syndrome, fetal alcohol syndrome, Noonan syndrome, several chromosomal aneuploidies
|
|
|
How do lymphangiomas and cystic hygromas present?
|
-Painless compressible neck masses that can transilluminate if large enough
-Often occur in the posterior triangle of the neck |
|
|
What do lympangiomas and cystic hygromas look like?
|
-Multiloculated cystic masses with septations
-They have a propensity to hemorrhage into themselves -Associated with hemorrhage-fluid level or heterogeneous signal associated with blood degradation products -Associated with an acute, dramatic increase in size -They tend not to displace adjacent soft tissue structures -This may prove helpful in differentiating between other cystic structures, like necrotic lymph nodes. |
|

|
1
|
|

|
2
|
|
|
3
|
|

|
4
|
|

|
5
|
|

|
6
|
|

|
7
|
|

|
8
|
|
|
9
|
|

|
10
|
|

|
11
|
|

|
12
|
|

|
13
|
|

|
14
|
|

|
15
|
|

|
16
|
|

|
17
|
|
|
18
|
|

|
19
|
|

|
20
|
|

|
21
|
|

|
22
|
|
|
23
|
|

|
24
|
|
|
25
|
|

|
26
|
|

|
27
|
|

|
28
|
|

|
29
|
|
|
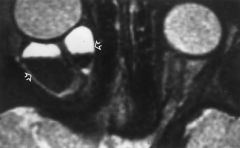
FIGURE 9.30. Lymphangioma. Axial T2WI reveals a cystic retrobulbar lesion (arrows) with a hematocrit effect (serum layered above red blood cells). Hemorrhage into a lesion is a characteristic feature of lymphangiomas and may be responsible for the rapid development of proptosis.
|
|

|
31
|
|

|
32
|
|

|
33
|
|

|
34
|
|

|
35
|
|

|
36
|
|
|
37
|
|

|
38
|
|

|
39
|
|

|
40
|
|

|
41
|