Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
Cerebral Cortex is
|
the thin gray covering on both hemispheres
- 90% neocortex - 10% allocortex motor cortex thickest; 4.5mm while visula thinest @ 1.5mm |
|
|
Cerebral Cortex Blood Supply
|
A, M, P cerebral aa.
|
|
|
How many layers in the cerebral cortex?
- neocortex |
6
1. Molecular layer 2. External granular 3. External pyramidal (association & commissural fibres) & major source of corticocortical fibres 4. Internal granular. Reives thalamocortical fibres 5. Internal Pyramidal; corticobulbur, corticospinal and corticostriatal fibres. Contains giant pyramidal cells of Betz only @ motor cortex (BA 4) 6. Multiform layer. source of corticothalamic fibres |
|
|
Brodmanns Distinct areas
|
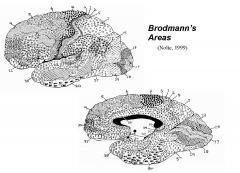
47
17= primary visual cortex - BASED ON ANATOMY |
|
|
Wilder Penfield
|
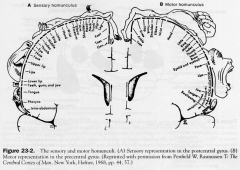
Homunculus
|
|
|
(1) Primary Cortical Areas (BA: 4)
|
(Motor, Somatosensory, Visual, Auditory, Gustatory)
1o deal with "raw" information and specific thalamus areas - usually topographically organised -In essence, a primary area receives information from the thalamus and passes it on to other cortical areas for further processing. |
|
|
(2) SECONDARY CORTICAL AREAS (BA: 6)
|
(Motor, Somatosensory, Visual, Auditory, Gustatory)
Each primary cortical area has a group of secondary areas that lie nearby. These secondary areas receive inputs mainly from their primary area, but some receive directly from the thalamus. Secondary cortical regions process the information from primary areas and add a layer of complexity to the information, i.e. they offer a more detailed analysis of a sensation or programme and plan a movement. |
|
|
(3) HIGHER-ORDER ASSOCIATION CORTICAL AREAS
|
3 major regions of higher-order cortex: prefrontal, parietal, limbic
- receive information from multiple sensory cortical regions - damage to cortices result in complex changes such as alterations in personality or the awareness of self. |
|
|
Central Sulcus
|
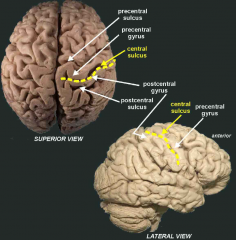
- the frontal sulcus run anterior to posterir and there are 3 (superior, m, inferior)
- the first sulcus to run horizontially is the precentral sulcus |
|
|
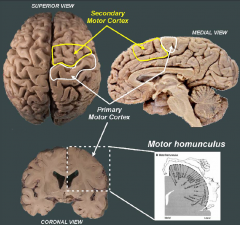
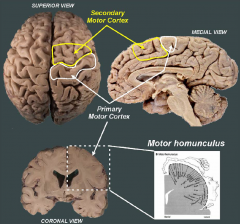
1o Motor Cortex
|
- The primary motor cortex (MI) encompasses the precentral gyrus and gives rise to most of the fibres in the corticospinal tracts (40%). It is involved in voluntary fine motor control.
- Stimulation of the medial aspect of the precentral gyrus will produce leg movements whereas stimulation of the most lateral aspect of M1 will result in face and tongue movements. - destruction causes contralateral spastic paresis |
|
|
2o Motor Cortex
|
The secondary motor cortex (MII) is not organized into movements. It receives information from association cortices and cerebellum and participates in movement planning. It has a dense projection to M1 and also sends projections directly to the spinal cord via the
corticospinal tract. Stimulation of M2 results in gross movements that require coordination among many muscles (turning head, trunk/limb movements). |
|
|
1o & 2o Motor Cortex
|
|
|
|
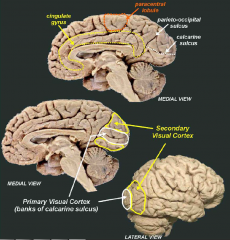
1o Visual Cortex
|
BA 17
- encompasses the upper and lower banks of the calcarine sulcus and receives visual input from the lateral geniculate nucleus (LGN) of the thalamus. - retinototopic organisation - superior banks of calcarine sulcus is contralateral inferior field vision |
|
|
2o Visual Cortex (V2) (BA 18, 19)
|
not organised retinotopically
- multiple regions v2-v5 -these regions add features such as motion, form and object recognition. Stimulation of secondary visual regions may cause complex visual changes such as the hallucination of formed images. |
|
|
V1 & V2
|
|
|
|
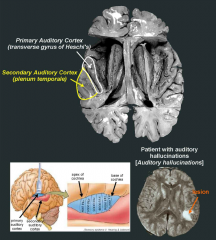
1o Auditory Cortex (BA 41)
|
temporal lobe within the lateral sulcus on the transverse gyrus of Heschl's. It receives auditory information from the medial geniculate nucleus (MGN) of the thalamus.
- tonotopic organisation (differing in Fq of sound) - Low frequency sounds are represented anterior and lateral, whereas high frequency sounds are represented posterior and medially. |
|
|
Secondary Auditory Cortex (BA 42)
|
The secondary auditory cortex is located immediately posterior to A1 in a region known as the plenum temporale
|
|
|
A1 & A2
|
|
|
|
Primary Gustatory Cortex (insula)
|
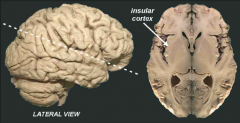
located in the frontal operculum and the adjacent insula
cortex. These regions receive taste information via the ventroposterior medial (VPM) nucleus of the thalamus. |
|
|
Higher-Order Association Cortical Areas
|
These primary and secondary regions then send projections to the higher-association cortical regions where various sensory modalities converge.
|
|
|
Prefrontal Association Cortex
|
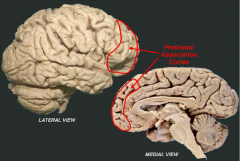
L: The prefrontal association cortex encompasses a large region of the fontal lobe immediately anterior to the secondary motor regions.
A: social and cognitive processing and may be responsible for higher order functions such as personality and cognition D: in the loss of ability to alter response when input changes – decision maker for appropriate movement. It may also result in: • difficulty going for the big picture; attention only to details. • They laugh or cry inappropriately • trouble with working memory – temporary data storage - deficits in concentration - problem solving - inappropriate social behaviour |
|
|
Phineas Gage
|
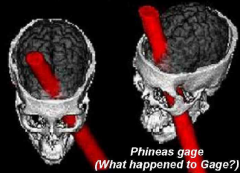
Before the accident he was a most
capable and efficient foreman, one with a well-balanced mind, and who was looked on as a shrewd smart business man. Following the prefrontal cortex damage he was said to be "irreverent, grossly profane, showing little deference for his fellows". He was also impatient and obstinate and unable to settle on any of the plans he devised for future action |
|
|
Parietal Association Cortex
|
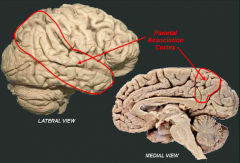
L: large region between the primary
somatosensory and secondary visual cortices and extends to include much of the temporal lobe. A: Given that this region lies in between most of the sensory cortical regions it is in a great position to receive multiple sensory modality information. As a result it is involved in complex multisensory perception including functions such as visuospatial localization, language, attention D: • finger agnosia (inability to recognize different fingers) • agraphia (inability to write) • alexia (inability to read) • dyscalculia ( decreased ability to calculate or use numbers) • left-right confusion • disturbances in the awareness of body image |
|
|
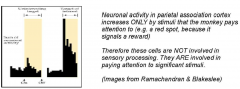
Stimulation of Parietal Association cortex
|
|
|
|
Contralateral Neglect Syndrome
|
- due to extensive parietal association damage
- not blind - common in stroke Patients bump into objects on contralateral side of lesion May not groom contralateral body May not eat food on side opposite to lesion The patients receive sensory information from the contralateral side of the body but they simply neglect it. |
|
|
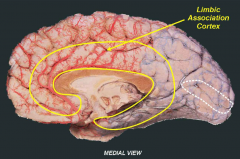
Limbic Association Cortex
|
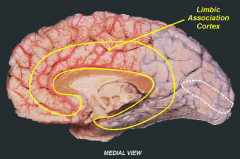
L: encompasses the cingulate gyrus and extends around the corpus callosum to include the parahippocampul gyrus.
A: Although it is most commonly associated with emotional state changes, it is involved in other functions such as motivation and attention. D: changes in emotional processing. For example, cingulate cortex damage has been reported to result in a patient being able to “feel” and accurately localize painful stimuli but they pain does not bother them. That is, the negative emotion associated with pain is lost |
|
|
Cerebral BS
|
- red= anterior cerebral aa.
- blue= post. |
|
|
SPEECH AND LANGUAGE REGIONS
|
- mostly left side of brain in most people
- There is a special area of cortex that deals with formulation of speech (motor) and one that deals with understanding speech (sensory): a major tract - arcuate tract - connects the two and is important for normal speech production and comprehension. |
|
|
Speech Lesions
|
- Cortical: speech formulation and/or comprehension
Subcortical (eg brainstem); may result in disturbance in speech articulation ([eg, whisper, explosive, strangled, slurring]) |
|
|
Broca’s area (BA 44, 45)
|
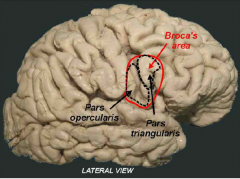
L: Posterior part of inferior frontal gyrus in dominant hemispherelies in the inferior frontal cortex in the regions known as the pars opercularis and pars triangularis. It lies immediately anterior to the region of M1 which
controls the muscle of the upper airway and so in some respects Broca's area acts as a premotor region. D: "expressive aphasia" - a lack of ability to produce coherent language, including spoken, written and signed forms. Patients suffering from Broca's aphasia can physically produce sounds and single words, but they cannot produce sentences or express thoughts. They will often use a single word or a short string of words and repeat them over and over; however they will not be able to grammatically express themselves. Similarly they can draw, but are not capable of writing coherent speech. They can understand speech, and often can form ideas to communicate, but they cannot put words together to communicate those ideas. - Output can be restricted to noun-verb combinations, with short sentence length and speech is usually laboured and slow. Broca's patient when asked what his favourite food was, replied: "Uh...uh...uh...choc...like...chocolate". + normally assoc. with contralateral facial & arm weakness due to motor strip involvement |
|
|
Wernicke’s area (BA 22,39,40)
|
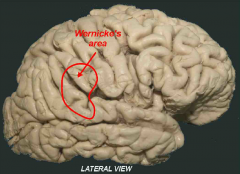
L: Post part of superior temporal gyrus
lies at the posterior extent of the lateral sulcus in the parietal and superior temporal regions. A: It is critical for language comprehension and damage to it results in "fluent aphasia" - the patient is unable to understand the content words while listening. D: They are unable to produce meaningful sentences; their speech has grammatical structure but no meaning - word salad. They have a similar disorder in writing, and impaired understanding of oral speech and reading. They can speak fluently, but their strings of words often lack coherent meaning. Thus unlike Broca's aphasia, Wernicke's damage does not result in difficulty with speech production, but with language production. |
|
|
Primary Somatosensory Cortex (BA,1,2,3)
|
L: postcentral gyrus
A: receives direct sensory input from the body and head. It receives information from somatic sensations such as touch, proprioception and pain from the contralateral face and body via the VPL and VPM thalamic nuclei. It is thought to be involved in the conscious perception of general sensation and in the accurate localization of these sensations. - Somatotopic fashion - Sensory homunculus based on greater nerves or 2 point discrimination can be detected - destruction results in contralateral hemihypesthesia & astereognosis |
|
|
SII
|
L: lies in the parietal operculum
A:has a gross somatotopic organization. It is thought that SII may be important in object recognition by touch and position sense |
|
|
Functional Areas;frontal lobe
|
1. Motor cortex
2. frontal eye field (BA 8) 3. Broca's Speech area 4. Prefrontal cortex |
|
|
Frontal Eye Field
|
BA 8
- destruction causes deviation of the eyes to ipisilateral side |
|
|
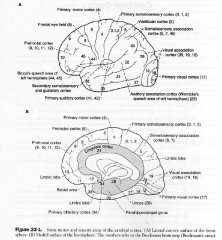
Cortex Overview
|
|
|
|
Functional Areas; Parietal Lobe
|
1. Sensory Cortex
2. Superior parietal lobule 3. Inferior parietal lobule of dominant hemisphere 4. Inferior parietal lobule of non-dominant hemisphere |
|
|
Superior Parietal Lobule
|
BA 5 & 7
- destruction= contralateral astereognosis & sensory neglect |
|
|
Inferior Parietal Lobule of Dominant Hemisphere
|
- Gerstmann's Syndrome
a. right & left confusion b. finger agnosia c. dysgraphia & dyslexia d. dyscalculia e. contralateral hemianopia or lower quadrantanopia |
|
|
Inferior Parietal Lobule of nondominant Hemisphere
|
destruction=
a. topographic memory loss b. anosognosia c. construction apraxia d. dressing apraxia e. contralateral sensory neglect f. contralateral hemianopia or lower quadrantanopia |
|
|
Language Production
|

|
|
|
Functional Areas: Temporal Lobe
|
1. 1o auditory cortex
2. Wernickes speech area (dominant hemisphere) 3. Meyer's loop 4. Olfactory bulb, tract & primary cortex 5. Hippocampal cortex 6. Anterior temporal lobe 7. Inferomedial occipitotemporal cortex |
|
|
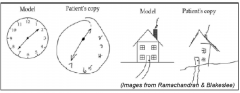
Construction apraxia Testing
|

|
|
|
Meyer's Loop
|
- consist of visual radiations that project to the inferior bank of calcarine sulcus. Interruption causes contralateral upper quadrantanopia (pie in the sky)
|
|
|
Olfactory Bulb, tract & 1o cortex
|
- ipsilateral anosmia
- irritative lesion causes olfactory hallucinations a. olfactory groove meningiomas b. Esthesioneuroblastomas; arise from bipolar sensory cells of olfactory mucousa, can extended past the cribiform plate into the anterior cranial fossa |
|
|
Hippocampal cortex
|
- bilateral lesion causes inability to consolidate short term memory into long term memory
|
|
|
Anterior Temporal Lobe
|
- amygdala
- bilateral damage= Kluver Bucy syndrome |
|
|
Inferomedial Occipitotemporal cortex
|
bilateral lesion= inability to recognise once-familiar faces (prosopagnosia)
|
|
|
Functional Areas: Occipital Lobe
|
bilateral lesions cause cortical blindness.
unilateral lesions cause contralateral hemianopia or quadrantanopia |
|
|
Focal Destructive Hemisphereic Lesions & Sx
|

|
|
|
Cerebral Dominance
|
- determined by Wada Test
- Amytal is injected into ICA, if the patient becomes aphasic, the anestheic was adminstered to the dominant hemisphere |
|
|
Dominant Hemisphere
|
responsible for (usually left)
- propositional language, speech & calculation |
|
|
Nondominant Hemisphere
|
responsible for 3D or spatial perception & non-verbal ideation
- allows superior recognition of faces |
|
|
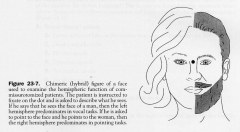
Split Brain Syndrome
|
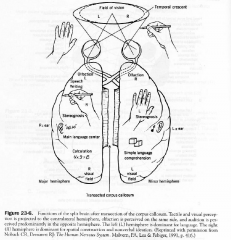
transection of corpus callosum
a. dominat better at vocal naming b. non-dominat (or mute) better at pointing. A blindfolded person cannot name objects that are presented to the nondominat sensory cortex through touch c. test (face test) d. Patient with alexia in left visual field the verbal symbols seen in the right eye cant access the language centers of the left |
|
|
Other Corpus callosum Injuries
|
- anterior corpus callosum lesion may result in akinetic mutism or tactile anomia
- post. cc lesion= alexia without agraphia - callostomy has been used to treat "drop attack" (colloid Cyst of 3rd ventricel) |