![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back
|
What is the immunogenic cause of Rheumatic Fever? |
Production of antibodies against protein M from Group A Strep pharyngitis protein M that cross-reacts with self-antigens in heart and CT |
|
|
What are the 5 major manifestations of Acute Rheumatic Fever? How many are needed for a diagnosis? |
1) Pancarditis 2) Polyarthritis (arthlagia only enough for minor) 3) Sub-Q Nodules 4) Chorea 5) Erythemia Marginatum *Need 2 major, or 1 major + 2 minor |
|
|
What EKG finding would be a minor indication for Acute Rheumatic Fever? |
prolonged PR interval |
|

|
Fibrinous pericarditis due to Acute Rheumatic Fever - results in a friction rub |
|
|
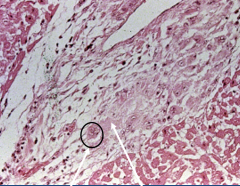
Myocarditis due to Acute Rheumatic Fever w/ Aschoff Body - granuloma containing lymphocytes, giant cell macrophages called Anitschkow cells (circled), and fibrinoid degeneration (right arrow) |
|
|
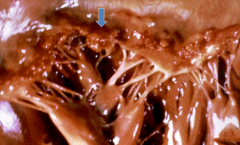
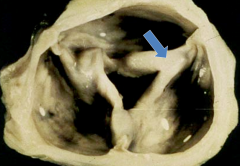
endocarditis due to acute rheumatic fever w/ small vegetations along the valve lines of closure called verracae (arrow) |
|
|
What are the 2 complications of acute rheumatic fever? |
1) die of an arrhythmia (1%) 2) increased susceptibility to RF if they get another strep ifxn (require penicillin prophylaxis) |
|
|
When does acute RF become chronic RF and what structural changes would indicate this transition? |
becomes chronic after 2-3 acute ifxns - look for leaflet and chordae tendinae thickening & fusion that leads to mitral stenosis (70%) or mitral & aortic stenosis (25%) |
|
|
What are the 3 complications of Chronic RF? |
1) A-fib leading to Mural Thrombosis w/ embolization 2) increased risk for bacterial endocarditis 3) CHF |
|
|
Compare the valve defects caused by acute and chronic rheumatic fever. |
Acute RF causes mitral/aortic regurgitation Chronic RF causes mitral/aortic stenosis |
|
|
Mitral Stenosis due to Chronic RF |
|
|
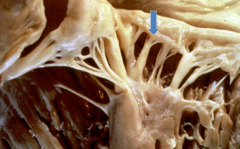
Fused chordae tendinae from Chronic RF |
|
|
Aortic valve leaflet fusion due to Chronic RF (probably has mitral stenosis as well!) |
|
|
What type of microbes cause acute endocarditis? What type of valves do they infect? How damaging are these infections? |
Virulent - Strep, Staph, Fungi Normal/Healthy valves Very destructive to valve |
|
|
What type of microbes cause subacute endocarditis? What type of valves do they infect? How damaging are these infections? |
Low-virulent organisms - Strep viridans Damaged valves only less destructive |
|

|
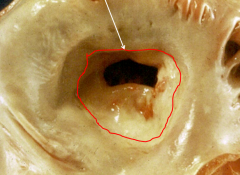
Infectious endocarditis that resulted in destruction of aortic valve (this would present as a new murmer) |
|
|
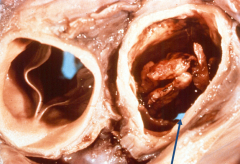
Acute Endocarditis that destroyed the aortic valve and resulted in perforation (arrow) that presents as a new murmer |
|
|
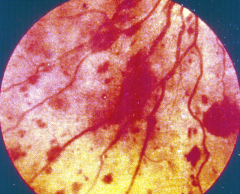
Roth spots from septic embolization of endocarditis vegetation to periphery |
|
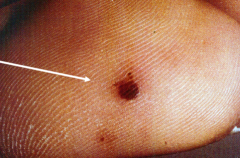
Spot is non-tender |
Janaway spot due to septic embolization of endocarditis vegetation to periphery - typically on palms and soles |
|

|
Osler's Node due to septic embolization of endocarditis vegetation to periphery - typically on fingers and toes |
|
|
A patient you are treating for endocarditis sudden has a sharp rise in BUN and creatinine on their labs. What has happened? |
Focal Glomerulonephritis due to immune complexes from inflammed endocardium getting filtered and trapped in kidney |
|
|
You find medium sized sterile vegetations that occur singly or in multiples along a valve's line of closure. What could this be and what would cause this? |
Non-bacterial Thrombotic Endocarditis - due to hypercoagulative states or underlying mucinous adenocarcinoma |
|
|
You find small sterile vegetations on the surface and undersurface of the mitral valve. What could this be and what would cause this? |
Liman-Sacks Endocarditis - due to SLE |