Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
93 Cards in this Set
- Front
- Back

You are shown a posteroanterior (PA) and lateral chest radiograph of a 64-year-old man with chest pain (Figures 1A and 1B). What is the MOST likely diagnosis?
A. Congestive heart failure B. Aortic stenosis C. Mitral valve disease D. Pericardial effusion |
B. Aortic stenosis
The chest radiograph shows normal heart size and vascularity. On the lateral view, there is calcification of the aortic valve, consistent with aortic stenosis. Identification of calcification of the aortic valve on a chest radiograph is usually associated with clinically significant aortic stenosis. |
|
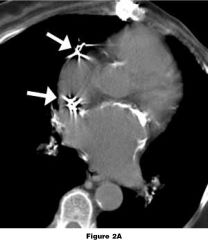
You are shown two images from a non-enhanced CT scan in a 77-year-old woman who has undergone pacemaker placement (arrow) and mitral valve replacement (arrowhead) (Figures 2A and 2B). The calcifications are related to which one of the following?
A. Pericarditis B. Pulmonary hypertension C. Rheumatic heart disease D. Coronary atherosclerosis |
C. Rheumatic heart disease
The calcifications are secondary to endocarditis from rheumatic heart disease. Other causes of endocarditis can also cause calcification of the left atrial wall. |
|

You are shown a posteroanterior (PA) and lateral chest radiograph of a 75-year-old woman (Figures 3A and 3B). What is the MOST likely diagnosis?
A. Atrial septal defect B. Chronic pulmonary embolism C. Pulmonary venous hypertension D. Cor pulmonale |
D. Cor pulmonale
This case shows enlargement of the central pulmonary arteries with diminished size of the peripheral vasculature, characteristic of pulmonary arterial hypertension. In this patient, the pulmonary arterial hypertension is a result of the severe emphysema as manifested by markedly increased lung volumes, flattening of the diaphragm and increase in AP diameter of the chest. Cor pulmonale is defined as pulmonary hypertension secondary to chronic lung disease. |
|
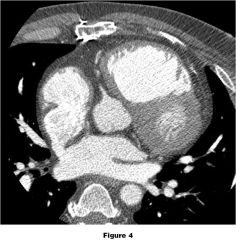
You are shown an axial contrast-enhanced CT scan of the chest (Figure 4). What is the MOST LIKELY diagnosis?
A. Ostium primum defect B. Ostium secundum defect C. Sinus venosus defect D. Patent foramen ovale |
C. Sinus venosus defect
Sinus venosus defects are the third most common ASD accounting for approximately 10 percent of all cases. The sinus venosus portion of the atrial septum separates the left atrium from the superior vena cava. The defect in this case is located in the superolateral aspect of the atrial septum at the junction of the superior vena cava and right atrium, near the insertion of the right pulmonary veins, consistent with a sinus venosus ASD. |
|
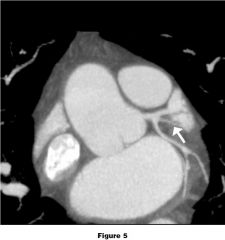
You are shown an oblique coronal reformatted image from a contrast-enhanced CT (Figure 5). Which coronary artery is depicted by the arrow?
A. Diagonal branch B. Obtuse marginal branch C. Ramus intermedius D. Septal branch |
C. Ramus intermedius
The left main coronary artery may trifurcate giving off the left anterior descending artery, the left circumflex artery and the ramus intermedius, or intermediate artery, which arises between the left anterior descending and left circumflex arteries as shown in this case. |
|

You are shown axial (see Figures 6A and 6B) and sagittally-reconstructed (Figure 6C) images from a contrast-enhanced CT scan of the chest obtained after a motor vehicle collision. What is the MOST LIKELY diagnosis?
A. Patent ductus arteriosus B. Traumatic aortic tear C. Ductus diverticulum D. Penetrating ulcer |
C. Ductus diverticulum
The combination of a small, smooth bump along the bottom edge of the aorta along with the lack of any evidence of flap or mediastinal hematoma is typical of a ductus diverticulum. The soft tissue strand joining the bump to the pulmonary artery represents the ligamentum arteriosum, the remnant of the ductus arteriosus. |
|
|
Concerning the morphologic right ventricle, which of the following is the MOST reliable indicator?
A. Anterior location of the ventricle B. Trabeculation of the ventricular wall C. Separation of the inflow and outflow valves by a muscular infundibulum D. The ventricle receives blood from the right atrium |
C. Separation of the inflow and outflow valves by a muscular infundibulum
Normally, the right ventricle receives blood from the right atrium, lies anterior to and is more trabeculated than the left ventricle. The inflow and outflow valves of the right ventricle are separated by the muscular infundibulum in contrast to the left ventricle where the valves are contiguous. In complex congenital cardiac anomalies, the separation of the inflow and outflow valves is the most reliable indicator of the morphologic right ventricle. |
|
|
Concerning the location of cardiac valves on a posteroanterior (PA) and lateral chest radiograph, which one is TRUE?
A. The aortic valve is located superior to the other valves. B. The tricuspid valve is the most anteriorly located valve. C. The mitral valve lies inferior to the other valves. D. The aortic valve lies closest to the pulmonary valve. |
B. The tricuspid valve is the most anteriorly located valve.
The tricuspid valve is the most anteriorly located valve. |
|
|
Concerning the position of the interventricular septum on short axis images of the heart, which one is TRUE?
A. It has a normal convexity toward the right ventricle. B. It has a sinusoid shape. C. It has a straight course separating the right and left ventricles. D. Its convexity varies in position during the cardiac cycle. |
A. It has a normal convexity toward the right ventricle.
On short axis images, the interventricular septum is curved with the convexity toward the right ventricle. This appearance is maintained during systole and diastole. Straightening, bowing with convexity toward the left ventricle and sinusoidal appearance of the interventricular septum are abnormal. |
|
|
Concerning cardiac aneurysms, which one is TRUE?
A. True aneurysms of saphenous vein grafts are a manifestation of atherosclerosis. B. Rupture of a sinus of Valsalva aneurysm occurs more commonly on the left. C. Left ventricular pseudoaneurysms typically occur at the cardiac apex. D. The neck of a left ventricular aneurysm is typically narrow. |
A. True aneurysms of saphenous vein grafts are a manifestation of atherosclerosis.
It is thought that atherosclerosis of saphenous vein bypass grafts results in decreased wall elasticity and resulting dilatation of the graft lumen over time. |
|
|
Concerning coronary artery atherosclerosis, which one is TRUE?
A. Coronary artery calcification is strongly associated with coronary atherosclerosis. B. On angiography, a stenosis greater than 40 percent of the luminal diameter is considered to be significant. C. On angiography, a stenosis greater than 60 percent of the luminal diameter is considered to be severe. D. When present, coronary artery calcifications make up about 50 percent of the total plaque burden. |
A. Coronary artery calcification is strongly associated with coronary atherosclerosis.
Coronary artery calcification is almost always associated with coronary atherosclerosis. |
|
|
Which one of the following congenital anomalies is MOST commonly associated with anomalous pulmonary venous drainage?
A. Ostium primum atrial septal defect B. Ostium secundum atrial septal defect C. Ventricular septal defect D. Sinus venosus atrial septal defect |
D. Sinus venosus atrial septal defect
Drainage of the pulmonary veins should be assessed in all patients with congenital anomalies. Nearly all patients with sinus venosus atrial septal defect have anomalous pulmonary venous drainage, most commonly drainage of the right upper lobe to the superior vena cava. Approximately 10 percent of patients with an ostium secundum atrial septal defect will have anomalous pulmonary venous drainage. |
|
|
What is the greatest advantage of conventional CR imaging systems over DR imaging systems?
A. Better detective quantum efficiency with lower dose B. Positioning flexibility C. Instantaneous readout of the latent image D. Better intrinsic spatial resolution |
B. Positioning flexibility
This is the main advantage of CR…. A passive, cassette-based imaging detector that emulates the screen-film paradigm, allowing use of conventional imaging equipment and providing excellent positioning flexibility that active, DR detectors in their current technology state cannot provide. |
|
|
Which one of the following structures directly communicates with the transverse sinus?
A. Oblique sinus B. Postcaval recess C. Superior aortic recess D. Posterior pericardial recess |
C. Superior aortic recess
The superior aortic recess arises from the transverse sinus and extends superiorly to surround the posterior, right lateral and anterior aspect of the ascending aorta. |
|
|
Concerning coronary artery dominance, which one is TRUE?
A. It is determined by which coronary artery supplies the majority of the heart. B. 85 percent of patients have a codominant system. C. It is determined by which artery supplies the posterior descending artery. D. 70 percent of patients have a left dominant system. |
C. It is determined by which artery supplies the posterior descending artery.
Dominance is determined by which artery supplies the posterior descending artery (PDA). In most patients (85%), the PDA is supplied by the right coronary artery and therefore is a right dominant system. If the PDA is supplies by the circumflex coronary artery, it is considered to be a left dominant system. A codominant system is one in which both the right coronary artery and circumflex oronary artery supply the PDA or when the right coronary artery supplies the PDA and the left circumflex coronary artery supplies the inferior left ventricular wall. |
|
|
Concerning a patient presenting with an acute myocardial infarction accompanied by severe bradycardia, which coronary artery or branch is MOST LIKELY involved?
A. Diagonal branch B. Left anterior descending coronary artery C. Right coronary artery D. Circumflex artery |
C. Right coronary artery
The atrioventricular (AV) node artery, supplies the AV node. In 85-90 percent of patients, the AV node artery arises from the right coronary artery at the point where it gives off the posterior descending artery. |
|
|
Concerning pulmonary vein ablation, which one is TRUE?
A. Accessory pulmonary veins are more common on the left. B. Myocardial sleeves are longest and thickest in the inferior pulmonary veins. C. The presence of left atrial thrombus is a contraindication. D. A common pulmonary vein is more common on the right. |
C. The presence of left atrial thrombus is a contraindication.
Due to the risk of stroke following manipulation of the left atrium, the presence of left atrial thrombus is a contraindication to pulmonary vein ablation. |
|
|
Concerning the Ross procedure, which one is TRUE?
A. It is suitable for children because the pulmonary autograft grows with the child. B. Patients undergoing the Ross procedure require lifelong anticoagulation. C. It is preferred because it is technically easier to perform than standard valve replacement. D. The procedure is performed to correct pulmonary valve stenosis. |
A. It is suitable for children because the pulmonary autograft grows with the child.
The Ross procedure replaces the aortic valve with the patient’s pulmonary valve and replaces the pulmonary valve with a cryopreserved pulmonary valve homograft. Follow-up studies have shown interval growth of the aortic valve graft in children and infants. |
|
|
Concerning the Blalock-Taussig shunt, which one is TRUE?
A. It connects the subclavian artery to the pulmonary artery. B. It creates a conduit between the right atrium and the pulmonary artery. C. It creates an atrial switch using an intra-atrial baffle made of pericardium. D. It connects the superior vena cava with the pulmonary artery. |
A. It connects the subclavian artery to the pulmonary artery.
The Blalock-Taussig shunt creates a connection between the systemic and arterial systems and is a palliative procedure that increases systemic arterial oxygenation by increasing blood flow to the pulmonary artery. |
|
|
What is the MOST common congenital heart defect?
A. Tetralogy of Fallot B. Atrial septal defect C. Bicuspid aortic valve D. Ventricular septal defect |
C. Bicuspid aortic valve
Bicuspid aortic valve is the most common congenital heart defect and occurs at a rate of 50-200 per 10,000 live births. |
|
|
Regarding cardiac CT scans, keeping all scan parameters the same, the dose to the patient with retrospective ECG gating when compared to prospective ECG triggering.
A. Increases B. Decreases C. Remains the same |
A. Increases
During retrospective ecg gating with multidetector CT (MDCT), the x-rays are ON throughout the cardiac cycle, however, only part of the data is used for reconstruction to achieve high temporal resolution with minimal motion artifacts. Whereas in prospective ecg triggering, the x-rays are ON only during certain part of the ecg signals, there by yielding lower radiation dose to the patient. |
|
|
Concerning isolated aortic valve stenosis, what is the MOST likely cause in an adult?
A. Rheumatic heart disease B. Calcific degeneration C. Congenitally stenotic aortic valve D. Infective endocarditis |
B. Calcific degeneration
Congenital aortic stenosis implies that the valve is stenotic at birth. Congenital bicuspid aortic valves are usually not stenotic at birth. Due to increased turbulence, the valve becomes traumatized leading to fibrosis and calcification. |
|
|
What is the MOST likely explanation for enlargement of the right atrium in a patient with mitral valve stenosis?
A. Tricuspid valve regurgitation B. Pulmonary valve stenosis C. Tricuspid valve stenosis D. Tricuspid valve prolapse |
A. Tricuspid valve regurgitation
Chronic pulmonary venous hypertension in patients with mitral stenosis leads to elevated pulmonary arterial and right ventricular pressures. If severe, these will result in failure of the right ventricle, usually with tricuspid regurgitation. |
|
|
Concerning differentiation of pseudoaneurysms from true aneurysms of the left ventricle, what is the MOST reliable imaging finding?
A. Identification of the number of myocardial layers in the wall of the aneurysm B. Involvement of the posterior or inferior walls of the left ventricle C. Size of aneurysm neck or mouth D. Thrombus lining the aneurysm. |
C. Size of aneurysm neck or mouth
Regardless of the imaging technique employed or the vascular structure involved, the sine qua non of a pseudoaneurysm is a narrow neck or mouth. |
|
|
Concerning left atrial enlargement in a patient with dilated (congestive) cardiomyopathy, what cause is MOST LIKELY?
A. Mitral valve regurgitation secondary to displacement of the papillary muscles B. Mitral valve regurgitation secondary to fusion and shortening of the chordae tendinae C. High left ventricular end-diastolic pressure resulting in left atrial hypertension D. Mitral valve regurgitation secondary to ischemic papillary muscle dysfunction |
A. Mitral valve regurgitation secondary to displacement of the papillary muscles
Left ventricular dilatation results in lateral displacement of the papillary muscles rendering them less efficient and resulting in mitral regurgitation. |
|
|
Concerning tricuspid valve regurgitation in adults, what is the MOST common etiology?
A. Infective endocarditis B. Right ventricular hypertension C. Ebstein’s’ anomaly of the tricuspid valve D. Rheumatic heart disease |
B. Right ventricular hypertension
The majority of cases of tricuspid regurgitation in adults result from high right sided pressures with or without right ventricular failure. |
|
|
Which structure is indicated by the arrow (Figure 1)?
A. Inferior aortic recess B. Transverse sinus C. Superior aortic recess D. Posterior pericardial recess |
C. Superior aortic recess
The superior aortic recess is the superior extension of the transverse sinus and extends anterior, lateral and posterior to the ascending aorta |
|
|
You are shown an image from an EKG-gated cardiac CTA (Figure 2). Which artery is indicated by the arrow?
A. Conal B. Sinoatrial nodal C. Posterior lateral D. Acute marginal |
B. Sinoatrial nodal
The sinoatrial nodal artery arises from the RCA in 50-60% of patients and supplies the sinoatrial node located at the junction of the superior vena cava and right atrium. |
|
|
You are shown turbo spin-echo (Figures 3A and 3B) and delayed gadolinium enhanced (Figures 3C and 3D) MR images of a 49 year old athlete with multiple episodes of syncope. What is the MOST LIKELY diagnosis?
A. Myocardial ischemia B. Arrythmogenic right ventricular dysplasia C. Left ventricular mass D. Myocardial scar |
D. Myocardial scar
The delayed, enhanced images (Figures C and D) demonstrate a focal area of increased signal in the posterolateral left ventricular wall consistent with an area of scarring. Normal myocardium will show transient enhancement after administration of gadolinium. Gadolinium accumulates in areas non-viable myocardium on delayed images since it is able to be distributed throughout the involved tissue due to cell membrane rupture. |
|
|
You are shown an axial image from a contrast enhanced CT of a 55-year-old man (Figure 4). The image shows calcification. Which one of the following is the location of the calcification?
A. Mitral annulus B. Coronary artery C. Left ventricular wall D. Pericardium |
C. Left ventricular wall
The calcification is located within the left ventricular myocardium consistent with dystrophic calcification within an area of previous infarction. |
|
|
You are shown the PA (Figure 5A) and lateral (Figure 5B) chest radiographs of a 66-year-old woman. Which one of the following is the MOST LIKELY diagnosis?
A. Mitral regurgitation B. Aortic regurgitation C. Pulmonary hypertension D. Mitral stenosis |
A. Mitral regurgitation
There is enlargement of the left atrium and left ventricle. The enlarged left atrium gives a “double” right heart border. On the lateral view the left atrium is seen extending posteriorly. The pulmonary arteries are not enlarged and there is no pulmonary edema. |
|
|
You are shown a contrast-enhanced CT image (Figure 6). Which of the following is the MOST LIKELY diagnosis?
A. Cardiac myxoma B. Cardiac fibroma C. Primary cardiac osteosarcoma D. Thrombus |
A. Cardiac myxoma
Cardiac myxoma is the most common benign primary cardiac tumor. The majority of cardiac myxomas arise within the left atrium, typically arising from the fossa ovalis. Calcification within the tumor may be seen. |
|
|
In regards to myocardial bridge, which one of the following statements is TRUE?
A. They occur in 5% of autopsy specimens. B. They are better depicted by CT than by angiography. C. They require surgical therapy. D. They most frequently affect the right coronary artery. |
B. They are better depicted by CT than by angiography.
Because multiplanar reformatted images can be obtained from the CT dataset, CT is better able to detect the intramuscular course of the coronary artery. |
|
|
Enlargement of which one of the following structures is the MOST reliable radiographic sign of pulmonary valve stenosis?
A. Enlargement of the pulmonary trunk B. Enlargement of the right ventricle C. Enlargement of the left main pulmonary artery D. Enlargement of the right and left main pulmonary arteries |
C. Enlargement of the left main pulmonary artery
Enlargement of the left main pulmonary artery, with or without pulmonary trunk enlargement, is the radiographic hallmark of pulmonary valve stenosis. |
|
|
Which of the following findings is the MOST reliable sign of elevated right ventricular pressure on a contrast-enhanced CT scan of the chest?
A. Leftward bowing of the interventricular septum B. Right ventricular hypertrophy C. Right ventricular enlargement D. Reflux of contrast into the inferior vena cava |
A. Leftward bowing of the interventricular septum
Abnormal curvature of the ventricular septum toward the left ventricle indicates elevated right ventricular pressure. |
|
|
Regarding cardiac transplantation, which one of the following statements is TRUE?
A. Accelerated atherosclerosis is an early complication. B. Postoperative screening for lymphoproliferative disease is the most common indication for imaging. C. Cyclosporine results in left ventricular hypertrophy. D. Cytomegalovirus and Aspergillus species are the most common cause of early postoperative infection. |
C. Cyclosporine results in left ventricular hypertrophy.
Ventricular hypertrophy can be caused by cyclosporine immunosuppressive therapy. |
|
|
Concerning cardiac neoplasms, which of the following is TRUE?
A. Myxoma is the most common benign cardiac tumor. B. Metastases to the heart are most commonly caused by renal cell carcinoma. C. Primary cardiac malignancies are more common than metastases to the heart. D. Malignant primary cardiac neoplasms are more common than benign neoplasms. |
A. Myxoma is the most common benign cardiac tumor.
Myxoma accounts for half of all primary cardiac tumors. |
|
|
Concerning the coronary circulation, which of the following statements is TRUE?
A. Dominance is determined by which vessel gives rise to the posterior descending artery and posterior left ventricular branches. B. Left dominant circulation is more common than right dominant circulation. C. The left coronary artery supplies the sinoatrial node in most individuals. D. The diagonal branches arise from the right coronary artery. |
A. Dominance is determined by which vessel gives rise to the posterior descending artery and posterior left ventricular branches.
Most patients are right dominant with the right coronary artery giving rise to the posterior descending artery and posterior left ventricular branches |
|
|
A 3-D cardiac CT image data set is acquired at 0.5-mm slice thickness. If the reconstruction interval is reduced from 0.5 mm to 0.3 mm, which of the following changes is MOST LIKELY to occur?
A. Increase patient dose B. Decrease patient dose C. Increase image size D. Increase scan time |
C. Increase image size
If the reconstruction interval is decreased, it results in higher number of slices yielding higher image size for 3D images |
|
|
Concerning prospective ECG gating in cardiac CT imaging, which of the following is TRUE?
A. Data is acquired throughout the cardiac cycle. B. Data is acquired only at pre specified points throughout the cardiac cycle. C. It allows for dynamic assessment of the heart and functional status. D. It involves more radiation dose to the patient than retrospective gating. |
B. Data is acquired only at pre specified points throughout the cardiac cycle.
Data is ideally only acquired when the heart is relatively motionless, as in diastole. So there are parts of the ECG cycle in which data is not being acquired, namely during systole (when the heart moves more). |
|
|
Concerning the use of B Blockers in cardiac CT imaging, which of the following statements is TRUE?
A. Heart rates of below 70 beats per minute are optimal. B. They can be administered to patients with asthma. C. Verapamil is not a useful alternative to beta-adrenergic blocking agents. D. Atrial fibrillation is a contraindication to beta-blocker use. |
A. Heart rates of below 70 beats per minute are optimal.
Several studies which used 4 and 16 detector row CT have shown consistently that at heart rates of greater than 70 beats a minute, cardiac motion degrades the images. |
|
|
Which of the following digital detectors directly converts x-ray signals into an electrical charge?
A. Photostimulable storage phosphor B. Structured cesium-iodine (CsI) scintillator C. Amorphous selenium (aSe) semiconductor D. Charge-coupled devices (CCD) photodiode |
C. Amorphous selenium (aSe) semiconductor
Digital detectors are classified by the signal transfer stages that occur during the image formation process in two categories. Indirect conversion is the process by which the x-rays are absorbed and converted into a secondary signal such as x-rays to light by a scintillator material or x-rays to trapped electrons to stimulation by a laser to light emission by a photostimulable phosphor. This light energy is subsequently converted to electron signals that comprise the signal that generates the corresponding digital value. Direct conversion is the process by which the x-rays directly produce the electron/hole pairs that are used to generate the corresponding digital values. Semi-conductor materials that absorb x-rays without scintillation, such as amorphous selenium, are classified as direct conversion materials. |
|
|
In regards to constrictive pericarditis, which of the following statements is TRUE?
A. The normal pericardium measures up to 5mm in thickness. B. Tuberculosis is the most common cause of constrictive pericarditis in the United States. C. The degree of pericardial calcification correlates with the degree of constriction. D. Pericardial thickening and calcification can occur in the absence of constrictive pericarditis. |
D. Pericardial thickening and calcification can occur in the absence of constrictive pericarditis.
Pericardial thickening or calcification may be present without physiologic impairment, although constrictive physiology is usually present when there is extensive pericardial calcification. |
|
|
Concerning anomalous origins of the coronary arteries, which of the following is TRUE?
A. Coronary artery anomalies are usually hemodynamically significant. B. Anomalous coronary arteries that pass between the right ventricular outflow tract / pulmonary artery and the ascending aorta are characterized by abnormal myocardial perfusion. C. With hemodynamically significant coronary artery anomalies, compression of the coronary artery occurs during systole. D. Coronary artery anomalies with a retroaortic course are associated with sudden death in young athletes. |
B. Anomalous coronary arteries that pass between the right ventricular outflow tract / pulmonary artery and the ascending aorta are characterized by abnormal myocardial perfusion.
Coronary arteries that pass between the right ventricular outflow tract / pulmonary artery and the ascending aorta are hemodynamically significant. The coronary artery can become compressed between two arteries during systole, when the vessels expand. |
|
|
In regards to cyanotic congenital heart disease presenting in infancy, which one of the following is MOST common?
A. Hypoplastic left heart syndrome B. Tetralogy of Fallot C. Truncus arteriosus D. Ventricular septal defect |
B. Tetralogy of Fallot
Tetralogy of Fallot is the most common cause of cyanotic heart disease presenting in the first month of life. |
|
|
Regarding atrial morphology, which one of the following is the MOST reliable indicator of the morphologic right atrium?
A. Connection with the superior vena cava B. Connection with the inferior vena cava C. Presence of a thin appendage with a narrow neck D. Presence of a tricuspid atrioventricular valve |
B. Connection with the inferior vena cava
Connection with the inferior vena cava is a reliable indicator of right atrial morphology. This can be a useful tool to establish the cardiac anatomy in cases of situs abnormalities and atrioventricular discordance. |
|
|
Regarding coronary artery aneurysms, which one of the following statements is CORRECT?
A. Aneurysmal dilatation is defined as an increase in vessel diameter twice that of the normal adjacent artery. B. Most coronary aneurysms are secondary to infection. C. Small aneurysms (<4mm) seen in the setting of Kawasaki disease (mucocutaneous lymph node syndrome) tend to regress. D. Aneurysms due to atherosclerosis have a high frequency of rupture. |
C. Small aneurysms (<4mm) seen in the setting of Kawasaki disease (mucocutaneous lymph node syndrome) tend to regress.
Kawasaki disease has multiple manifestations in the heart, including coronary aneurysm formation. Large aneurysms (> 8mm) are frequently complicated by thrombosis and subsequent myocardial infarction. They may also rupture. Small aneurysms tend to regress to normal caliber over time. |
|
|
Regarding hypertrophic cardiomyopathy, which one of the following is an associated valvular abnormalty?
A. Aortic valve stenosis B. Mitral valve stenosis C. Systolic anterior motion of the mitral valve D. Mitral valve prolapse |
C. Systolic anterior motion of the mitral valve
The increased flow velocity occurring through the narrowed subvalvular left ventricular outflow tract draws the anterior leaflet of the mitral valve anteriorly due to the Venturi effect. This results in further obstruction of the left ventricular outflow tract. |
|
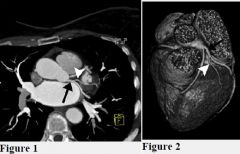
Figure 1 is an axial maximum intensity projection (MIP) image from a contrast-enhanced coronary CT angiogram. Figure 2 is a surface-rendered image from the same study, viewed from the anterior direction with the cardiac apex located at the bottom of the image. The black arrow indicates the left circumflex coronary artery. What vessel is indicated by the white arrowhead?
A. Diagonal branch B. Ramus intermedius C. Obtuse marginal branch D. Acute marginal branch |
C. Obtuse marginal branch
Rationale: Obtuse marginal branches represent the major branch vessels arising from the left circumflex coronary artery. |
|
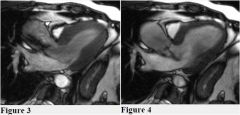
You are shown true steady-state free-procession (gated white blood) MR images of the left ventricular outflow tract during systole (Figure 3) and diastole (Figure 4). Which one of the following statements is TRUE?
A. There is aortic stenosis and mitral regurgitation. B. There is aortic stenosis and systolic anterior motion of the mitral valve. C. There is aortic regurgitation and mitral stenosis. D. There is aortic stenosis and aortic regurgitation. |
D. There is aortic stenosis and aortic regurgitation.
Rationale: Areas of signal void are present during both systole and diastole indicating valvular stenosis and regurgitation respectively. |
|
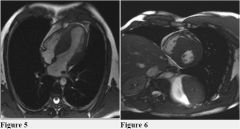
Figures 5 and 6 are steady-state free-procession MR images obtained in the axial and short axis planes, respectively. What is the MOST LIKELY diagnosis?
A. Hypertrophic cardiomyopathy B. Hypertensive cardiomyopathy C. Alcohol-related cardiomyopathy D. Ischemic cardiomyopathy |
A. Hypertrophic cardiomyopathy
Rationale: The images demonstrate marked thickening of the basal aspect of the interventricular septum. This is the characteristic finding of hypertrophic cardiomyopathy with asymmetric septal hypertrophy (formerly known as idiopathic hypertrophic subaortic stenosis). In hypertrophic cardiomyopathy with asymmetric septal hypertrophy, the interventricular septum is at least 1.3 times thicker than the left ventricular free wall, and is accompanied by obstruction of the left ventricular outflow. This characteristically results in systolic anterior motion (SAM) of the mitral valve. |
|
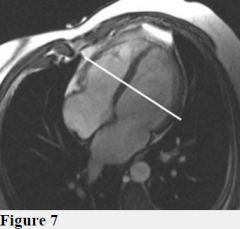
You are shown a cardiac MR image (Figure 7). Which of the following image planes is being prescribed?
A. Vertical long axis B. Horizontal long axis C. Short axis D. Four chamber view |
C. Short axis
Rationale: The short axis plane is obtained by running a line perpendicular to the horizontal or vertical long axis and interventricular septum. The short axis view images are obtained orthogonal to the long axis of the left ventricle (Image C). |
|
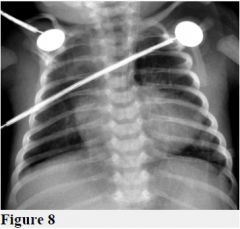
You are shown a portable chest radiograph (Figure 8) of a 3-day-old infant with respiratory distress. What is the MOST LIKELY diagnosis?
A. Total anomalous pulmonary venous return B. Ventricular septal defect C. Transposition of the great vessels D. Tetralogy of Fallot |
D. Tetralogy of Fallot
Rationale: The chest radiograph shows a right aortic arch, diminished vascularity and an uplifted cardiac apex with lung interposed between the heart and the left hemidiaphragm -the classic coeur en sabot. These findings are typical of Tetralogy of Fallot. |
|
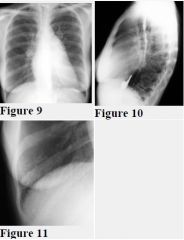
You are shown a PA and lateral chest radiograph (Figures 9 and 10) with a magnified image (Figure 11) of the right lower lobe. What is the diagnosis?
A. Mitral stenosis B. Left ventricular failure C. Pulmonary arterial hypertension D. Atrial septal defect |
A. Mitral stenosis
Rationale: Early changes of mitral stenosis include cephalization or redistribution of the pulmonary blood flow to the upper lobes. Enlargement of the left atrial appendage is specific for rheumatic mitral stenosis. The left ventricle is normal in size. There is mild left atrial enlargement. Kerley B lines represent interstitial edema often with an element of fibrosis. |
|
|
The length of image acquisition for a fast spin-echo (FSE) pulse sequence compared to a standard spin-echo pulse sequence is:
A. TR × # phase encoded steps × echo train length. B. TE × # frequency encoded steps × echo train length. C. TR × # phase encoded steps / echo train length. D. TE × # frequency encoded steps / echo train length. |
A. TR × # phase encoded steps × echo train length.
C. TR × # phase encoded steps / echo train length. |
|
|
Concerning coarctation of the aorta, which one of the following is TRUE?
A. The most common location of coarctation is pre-ductal. B. Aortic coarctation is associated with Turner syndrome. C. There is a measurable pressure gradient in aortic pseudocoarctation. D. Inferior rib notching affects the first through eighth ribs. |
B. Aortic coarctation is associated with Turner syndrome.
Rationale: Aortic coarctation is found in up to 20% of patients with Turner syndrome, making it the most common associated cardiac abnormality in this population. Aortic coarctation is also associated with patent ductus arteriosus, ventricular septal defect, bicuspid aortic valve, circle of Willis aneurysms and patent ductus arteriosus aneurysms. |
|
|
Concerning congenital absence of the pericardium, which one of the following is TRUE?
A. Complete absence is more common than partial absence. B. Partial absence is more commonly right sided. C. It can result in infarction of the left atrial appendage. D. It can mimic adenopathy in the aorticopulmonary window. |
C. It can result in infarction of the left atrial appendage.
Rationale: Partial absence of the pericardium can result in herniation of the left atrial appendage through the defect which can result in infarction. |
|
|
In order to have a left dominant coronary artery system, which one of the following must be supplied by the circumflex coronary artery?
A. Acute marginal artery B. Posterior lateral artery C. Posterior descending artery D. Conus artery |
C. Posterior descending artery
Rationale: Dominance is determined by the artery that crosses the crux of the heart (the junction of the atrioventricular and the interventricular grooves) and gives rise to the posterior descending artery. |
|
|
Which digital detector material directly converts x-ray signals into electronic charge when coupled to a thin-film transistor array?
A. Photostimulable storage phosphor B. Structured cesium iodine (CsI) scintillator C. Amorphous selenium semiconductor D. Charge-coupled device (CCD) photodiode |
C. Amorphous selenium semiconductor
Rationale: Digital detectors are classified by the signal transfer stages that occur during the image formation process in two categories. Indirect conversion is the process by which the x-rays are absorbed and converted into a secondary signal such as x-rays to light by a scintillator material or x-rays to trapped electrons to stimulation by a laser to light emission by a photostimulable phosphor. This light energy is subsequently converted to electron signals that comprise the signal that generates the corresponding digital value. Direct conversion is the process by which the x-rays directly produce the electron/hole pairs that are used to generate the corresponding digital values. Semi-conductor materials that absorb x-rays without scintillation, such as amorphous selenium, are classified as direct conversion materials. |
|
|
Where is the crista terminalis located?
A. At the junction of the left atrial appendage and left superior pulmonary vein B. Between the right ventricular free wall and the interventricular septum C. Between the inflow and outflow portions of the right ventricle D. In the right atrium extending from the superior vena cava to the inferior vena cava |
D. In the right atrium extending from the superior vena cava to the inferior vena cava
Rationale: The crista terminalis is a smooth muscular ridge that lies between the trabeculated right atrial appendage which arises from the primitive right atrium and the smooth-walled right atrium arising from the sinus venosus. It is of varying prominence in patients. |
|
|
What is the MOST common cause of tricuspid regurgitation in adults?
A. Rheumatic heart disease B. Pulmonary arterial hypertension C. Carcinoid disease D. Endocarditis |
B. Pulmonary arterial hypertension
Rationale: Most cases of tricuspid regurgitation in adults are caused by right ventricular or pulmonary arterial hypertension which can result in dilatation of the right ventricle and tricuspid annulus. |
|
|
Regarding myocardial bridging, which one of the following is TRUE?
A. It most frequently involves the right coronary artery. B. It is most easily demonstrated during diastole on cardiac catheterization. C. It refers to abnormal interconnections between major coronary arteries. D. It may result in ischemia. |
D. It may result in ischemia.
Rationale: Chest pain and myocardial infarction may occur if the degree of coronary narrowing is severe (>75%). |
|
|
From which cardiac structure do papillary fibroelastomas typically arise?
A. Pericardium B. Ventricular myocardium C. Cardiac valves D. Pulmonary vein ostia |
C. Cardiac valves
Rationale: Papillary fibroelastomas arise from cardiac valves in 90% of cases. They are typically less than one centimeter in size. Patients with tumors arising from the valves of the left heart may present clinically with embolic disease. |
|
|
Which of the following is TRUE about cardiac valvular disease secondary to carcinoid syndrome?
A. Valve dysfunction occurs only when carcinoid tumor metastasizes to the heart. B. The tricuspid valve is involved and the pulmonic valve if spared. C. The aortic and mitral valves can be affected in the presence of a right-to-left shunt. D. Right-sided cardiac chambers are generally normal in size. |
C. The aortic and mitral valves can be affected in the presence of a right-to-left shunt.
Rationale: Since the vasoactive substances produced by carcinoid tumors are inactivated in the lungs, left-sided valvular dysfunction is extremely rare, though it can be seen in the setting of right-to-left shunts, and has been reported with primary bronchial carcinoid tumors. |
|
|
Concerning complications of thoracic aortic dissection, which one of the following is TRUE?
A. The most common valvular complication is aortic regurgitation. B. The most common coronary artery complication is occlusion or dissection of the left main coronary artery. C. Stanford type B (DeBakey type III) dissections are frequently complicated by cardiac tamponade. D. In the aortic arch, the false lumen typically follows the lesser curvature of the arch. |
A. The most common valvular complication is aortic regurgitation.
Rationale: Dissections that involve the ascending aorta may result in a flail aortic valve leaflet or may disrupt the aortic valve annulus, leading to aortic regurgitation. Aortic regurgitation is seen in over half of patients with ascending aortic dissection. |
|
|
Which of the following pathologies result in delayed enhancement on perfusion MR imaging using contrast-enhanced T1-weighted images?
A. Myocardial infarction B. Myocardial stunning C. Myocardial ischemia D. Myocardial hibernation |
A. Myocardial infarction
Rationale: Delayed hyper-enhancement refers to areas of high signal intensity on contrast-enhanced T1 weighted images. This enhancement occurs because contrast is retained in areas of irreversible myocardial injury (i.e. infarction). It is thought to be due to contrast leakage into the intracellular space due to myocardial myocyte membrane disruption. Membrane disruption has been shown to be closely related to cell death. The increased tissue level of contrast results in high signal intensity. |
|
|
Regarding coronary calcium CT assessment, which one of the following is TRUE?
A. The amount of coronary calcium is not related to the extent of atherosclerosis. B. Retrospective ECG-gating is used. C. The Agatson score incorporates lesion attenuation and size. D. The amount of calcification is proportional to the degree of stenosis at that particular site. |
C. The Agatson score incorporates lesion attenuation and size.
Rationale: The two methods of scoring are volume scoring and the Agatson score. An attenuation of +130 HU (two standard deviations above HU of blood) and an area greater than 1mm2 have been arbitrarily selected to score calcified lesions. Regions of interest are placed around calcified lesions. Volume scoring involves measuring the area of the lesion, whereas the Agatson score also takes into account the attenuation of the lesion. Calcium scores are greater for areas of higher attenuation with the Agatson score. With both scoring systems, the values are compared to normalized scores based upon age and gender matched controls. |
|
|
Which of the following anomalous vascular structures results in posterior impression upon the trachea and anterior impression upon the esophagus?
A. Double aortic arch. B. Right aortic arch with aberrant left subclavian artery C. Left aortic arch with aberrant right subclavian artery D. Left pulmonary artery arising from the right pulmonary artery |
D. Left pulmonary artery arising from the right pulmonary artery
Rationale: A pulmonary artery sling is defined as an aberrant origin of the left pulmonary artery from the right pulmonary artery. This vessel typically passes between the trachea and esophagus, resulting in posterior impression upon the trachea and anterior impression upon the esophagus. The diagnosis of a pulmonary artery sling can be made on an esophagogram. |
|
|
Concerning cardiac failure, what is the primary cause of lung edema?
A. Increased hydrostatic pressure B. Decreased oncotic pressure C. Increased capillary permeability D. Failure of lymphatic resorption |
A. Increased hydrostatic pressure
Rationale: Pulmonary edema secondary to cardiac failure occurs when the pulmonary capillary pressure increases, raising the hydrostatic pressure between the capillary and the pulmonary interstitium. |
|
|
Concerning lipomatous hypertrophy of the intra-atrial septum, which one of the following is TRUE?
A. It is associated with ventricular arrhythmias. B. If large enough, it completely separates the atria. C. It may contain brown fat. D. It has malignant potential. |
C. It may contain brown fat.
Rationale: Histologically, lipomatous hypertrophy of the interatrial septum is composed of brown fat and is histologically distinct from a true, encapsulated lipoma. Increased uptake may be present on PET scan. |
|
|
Which of the following is the MOST LIKELY diagnosis for a newborn with cyanosis, diminished pulmonary vascularity, and an enlarged cardiac silhouette?
A. Tetralogy of Fallot B. Complete atrioventricular canal defect C. Complete transposition of the great vessels D. Pulmonary atresia with intact ventricular septum |
D. Pulmonary atresia with intact ventricular septum
Rationale: Patients with pulmonary atresia (or critical pulmonary stenosis) with an intact ventricular septum present with diminished pulmonary blood flow because of the outflow obstruction. The right atrium is always enlarged and right ventricular enlargement is also present when the tricuspid valve is regurgitant. Therefore, the cardiac silhouette is typically enlarged. Affected patients are dependent on a patent ductus. |
|

You are shown a transverse MIP image from a cardiac CT (Figure 1). What type of atrial septal defect is shown?
A. Sinus venosus B. Septum secundum C. Septum primum D. Coronary sinus |
A. Sinus venosus
A defect is present superior and posterior in the interatrial septum and has associated partial anomalous pulmonary venous connection on the right. |
|

You are shown PA and lateral chest radiographs (Figures 2 and 3) of a 70-year-old man. What is the MOST LIKELY diagnosis?
A. Constrictive pericarditis B. Calcified mitral annulus C. Aortic valvular stenosis D. Ascending aortic aneurysm |
C. Aortic valvular stenosis
Dense calcification is present in the anatomic location of the aortic valve. When calcification of the aortic valve is visible on chest radiograph, it typically indicates the presence of clinically significant aortic stenosis. |
|

You are shown an axial T1-weighted image of the great vessels (Figure 4). What is the MOST LIKELY diagnosis?
A. Takayasu arteritis Axial T1-weighted MR shows abnormal thickening of the ascending aorta and the pulmonary artery, a finding seen in patients with Takayasu arteritis. B. Aortic coarctation C. Aortic aneurysm D. Kawasaki disease |
A. Takayasu arteritis
Axial T1-weighted MR shows abnormal thickening of the ascending aorta and the pulmonary artery, a finding seen in patients with Takayasu arteritis. |
|
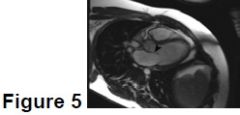
A steady-state free precession image in the three-chamber plane from a cardiac MRI is shown in Figure 5. What structure is indicated by the black arrowhead?
A. Anterior cusp of the mitral valve B. Posterior cusp of the mitral valve C. Anterior cusp of the tricuspid valve D. Posterior cusp of the aortic valve |
A. Anterior cusp of the mitral valve
The structure denoted in the image is the mitral valve. This is apparent as it is located between the left atrium and the thick-walled left ventricle. The anterior cusp of the mitral valve is interposed between the left atrioventricular orifice and the left ventricular outflow tract. Knowledge of the appearance of this valve and its relationship to the left ventricular outflow tract is important in the assessment of asymmetric septal hypertrophic cardiomyopathy. In this condition, the hypertrophied basal left ventricular septum results in narrowing of the LV outflow tract, and can result in systolic anterior motion of the anterior mitral valve cusp due to the Bernoulli principle, and further LV outflow obstruction. |
|

The images shown are from a cardiac MRI performed on an 18-year-old woman presenting with heart failure. Figures 6 and 7 are vertical long axis (two-chamber) steady-state free precession images obtained at end-diastole and end-systole, respectively. Figures 8 and 9 are short axis, steady-state free precession images obtained at end-diastole and end-systole, respectively. What is the MOST LIKELY diagnosis?
A. Myocardial noncompaction B. Hypertrophic cardiomyopathy C. Constrictive pericarditis D. Restrictive cardiomyopathy |
A. Myocardial noncompaction
Myocardial noncompaction is a rare disorder characterized by the failure of the myocardium to undergo appropriate compaction during embryogenesis. This compaction typically occurs during the fifth through eighth embryologic weeks, where the developing myocardium transitions from a loosely organized collection of myocardial fibers into a discrete muscular chamber. Failure of this mechanism results in a left ventricle comprised, in whole or in part, of noncompacted myocardial fibers, typically involving the inferior and lateral walls. This can result in heart failure, dysrhythmias, and thromboembolic disease. Imaging, either with MRI or echocardiography, reveals a ratio of noncompacted myocardium to normal myocardium of at least 2:1 in affected areas. |
|
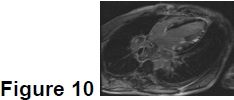
A 26-year-old man presents with chest pain, dyspnea, and ventricular dysrhythmia. A four-chamber, delayed, postcontrast, phase-sensitive inversion recovery MR image (Figure 10) was obtained. What is the MOST LIKELY diagnosis?
A. Hypertrophic cardiomyopathy B. Sarcoidosis C. Myocardial infarction D. Arrhythmogenic right ventricular dysplasia |
B. Sarcoidosis
Sarcoidosis is a multisystem disorder characterized by non-caseating granuloma deposition. Cardiac involvement is noted in approximately 5% of affected patients who typically present with heart block or other dysrhythmia. MRI can be a useful tool for diagnosis in patients with sarcoidosis and dysrhythmia. Granuloma deposition in the myocardium in the acute setting demonstrates increased T2 signal intensity and delayed myocardial enhancement. CT scan of this patient (not shown) demonstrated bulky mediastinal adenopathy and pulmonary nodules. The patient was subsequently found to have elevated ACE levels and granulomas were found on lymph node biopsy. |
|
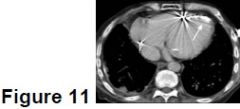
You are shown an axial contrast-enhanced CT image of the heart (Figure 11). What abnormality is depicted by the arrow?
A. Myocardial infarction B. False aneurysm C. Pericardial calcification D. Mediastinal fat necrosis |
A. Myocardial infarction
There is an irregular, curvilinear calcification of the left ventricular apex and interventricular septum typical of dystrophic calcification of a prior myocardial infarction. |
|
|
Concerning obstructive hypertrophic cardiomyopathy, which one of the following is TRUE?
A. Asymmetric thickening of the interventricular septum causes aortic valvular stenosis. B. Systolic anterior motion of the anterior mitral leaflet contributes to obstruction. C. It is a sporadic and not an inherited disease. D. Cardiomegaly is a common feature on chest radiograph. |
B. Systolic anterior motion of the anterior mitral leaflet contributes to obstruction.
While a variable finding, systolic anterior motion (SAM) of the anterior mitral valve leaflet often contributes to left ventricular outflow obstruction with the leaflet sometimes touching the interventricular septum. |
|
|
Which one of the following arteries typically supplies the sinoatrial node?
A. Right coronary artery B. Proximal left anterior descending artery C. Proximal circumflex artery D. Posterior descending artery |
A. Right coronary artery
The SA nodal branch arises from the proximal RCA in approximately 65% of the population coursing posteriorly toward the region of the SA node. |
|
|
What is the MOST common neoplasm to arise from the cardiac valves?
A. Fibroelastoma B. Elastofibroma C. Carcinoid D. Myxoma |
A. Fibroelastoma
Papillary fibroelastoma is a collection of avascular fronds of dense connective tissue lined by endothelium. Fibroelastomas account for approximately 10% of all primary cardiac tumors, with about 90% of them arising at valvular surfaces. |
|
|
What is the MOST common malignant cardiac neoplasm in adults?
A. Metastasis B. Myxoma C. Lymphoma D. Rhabdomyosarcoma |
A. Metastasis
Cardiac metastases are far more common than primary cardiac neoplasms. |
|
|
Regarding the management of heart rate in cardiac CT, which one of the following is TRUE?
A. Beta-blockers can be administered to patients with asthma. B. The optimal heart rate is less than 70 beats per minute. C. Atrial fibrillation is a contraindication to beta-blockers. D. Verapamil is not a useful beta-blocker alternative. |
B. The optimal heart rate is less than 70 beats per minute.
Numerous studies have demonstrated that heart rates below 70 BPM drastically reduce image degradation caused by cardiac motion. |
|
|
Which of the following is the MOST common cause of cyanotic congenital heart disease?
A. Ventricular septal defect B. Truncus arteriosus C. Patent ductus arteriosus D. Tetralogy of Fallot |
D. Tetralogy of Fallot
Tetralogy of Fallot is the most common cyanotic heart disease presenting during the first month of life. |
|
|
Concerning acute aortic intramural hematoma, which of the following is TRUE?
A. Conservative treatment is indicated regardless of the location within the aorta. B. Penetrating atheromatous ulcers are a common cause. C. The ascending aorta is most commonly involved. D. It is best identified with contrast-enhanced multidetector CT. |
B. Penetrating atheromatous ulcers are a common cause.
Penetrating atheromatous ulcer is a major cause of intramural hematoma. |
|
|
The two major factors that influence the in-plane spatial resolution in a CT scanner are which of the following?
A. kVp and mA B. Focal spot and acquisition field of view C. Scan time and acquisition pitch D. Beam hardening and scatter |
B. Focal spot and acquisition field of view
The focal spot size will determine geometric blurring, and the acquisition FOV will determine the effective sampling pitch of the projection data at the isocenter. These two components will have the major impact on the spatial resolution that can be reconstructed by the computer. |
|
|
In patients with mitral valve stenosis, what is the MOST LIKELY cause of right atrial enlargement?
A. Tricuspid valve prolapse B. Tricuspid valve stenosis C. Pulmonary valve stenosis D. Tricuspid valve regurgitation |
D. Tricuspid valve regurgitation
In patients with mitral stenosis, chronic pulmonary hypertension leads to elevation of pulmonary arterial and right ventricular pressures. If severe, this will result in right ventricular failure and dilatation which typically causes tricuspid regurgitation. |
|
|
Regarding congenital heart disease, which of the following congenital defects is MOST common?
A. Ventricular septal defect B. Atrial septal defect C. Tetralogy of Fallot D. Bicuspid aortic valve |
D. Bicuspid aortic valve
Bicuspid aortic valve is the most common congenital heart defect and occurs at a rate of 50-200 per 10,000 live births. |
|
|
Regarding aortic pseudocoarctation, which of the following statements is TRUE?
A. Pseudocoarctation begins proximal to the origin of the left subclavian artery. B. Significant pressure gradient across the stenosis is characteristic. C. Poststenotic aneurysmal dilation may progress over time. D. Patients are symptomatic and typically present with chest pain. |
C. Poststenotic aneurysmal dilation may progress over time.
Areas of aneurysmal dilation may occur distal to areas of narrowing in pseudocoarctation. These may become progressively dilated, and should be followed. |
|
|
Polysplenia is characterized by which one of the following?
A. Bilateral atrial appendages with triangular morphology and wide ostia B. More severe and complex cardiac anomalies than asplenia C. An association with azygous continuation of the inferior vena cava D. Bilateral eparterial mainstem bronchi |
C. An association with azygous continuation of the inferior vena cava
The most common cardiovascular anomaly associated with polysplenia is azygous continuation of the inferior vena cava. |
|
|
Regarding congenital absence of the pericardium, which one of the following is TRUE?
A. Complete absence is more common than partial absence. B. Partial absence occurs more commonly on the left. C. Pulmonary arterial stenosis is the most common complication. D. The left ventricle is the most commonly entrapped chamber. |
B. Partial absence occurs more commonly on the left.
In patients with partial absence of the pericardium, the a left-sided defect is more common than a right-sided defect. |
|
|
Which one of the following is characteristic of cardiac tamponade?
A. Decreased diastolic filling pressures B. Dilatation of the vena cavae C. Dilatation of the coronary sinus D. Left ventricular dilatation |
B. Dilatation of the vena cavae
As a result of increased diastolic filling pressures, the vena cavae become dilated. |
|
|
What is the MOST consistent feature of Ebstein anomaly on chest radiography?
A. Aortic enlargement B. Pulmonary trunk enlargement C. Left atrial enlargement D. Right atrial enlargement |
D. Right atrial enlargement
The underlying malformation in Ebstein anomaly is the downward displacement of the posterior and septal leaflets of the tricuspid valve into the right ventricle. Severe tricuspid regurgitation results in massive dilatation of the right heart. On chest radiograph, the left atrium is normal in size, the aorta is generally small, and the pulmonary trunk is generally not seen. |