Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
90 Cards in this Set
- Front
- Back
|
In which of the following is cryosurgery NOT a primary indication?
a) Sarcoids b) Papilloma c) Melanoma d) SCC e) Ocular SCC |
c) Melanoma
(usually not also primary in sarcoids or SCCs too but I guess it can be) |
|
|
In which of the following is cryosurgery usually used after surgical debulking?
a) Sarcoids b) Papilloma c) Melanoma d) SCC e) Ocular SCC |
d) SCC
e) Ocular SCC (also sarcoids) |
|
|
Cryosurgery destroys tissues at temperatures below _______ degrees C.
|
<-20 degrees C
|
|
|
Which tissues are not directly amenable to cryosurgery and why? In which of these tissues can this fact be exploited?
|
Dry tissues (less water; can't freeze; eg: cornea - good for SCC cryo-sx without corneal damage)
Vascular tissues (more heat; can't freeze) Bone (damages matrix leading to fractures and OA) |
|
|
How can vascular tissues be cryo-surgerized?
|
Use local epinephrine or occlude vessels
|
|
|
Which of the following are important to cryosurgery?
a) rapid freezing b) rapid thawing c) slow freezing d) slow thaw e) 2-3 freeze/thaw cycles |
a) rapid freeze
d) slow thaw e) 2-3 freeze/thaw cycles |
|
|
What are the 3 types of probes in cryosurgery? Which has the fastest cooling? Which afford good control?
|
Spray (fastest cooling)
Hollow probe (slow cool; good control) Solid probe (fast cool; good control) |
|
|
How often should cryosurgery be repeated on a lesion? When should it be discontinued?
|
Every 4 weeks until skin is normal or biopsy is negative
|
|
|
Why is O2 not used in endoscopy?
|
air emboli
|
|
|
Regarding triangulation in arthroscopy, the instrument should be ___________ the lesion while the arthroscope should be ___________ the lesion.
|
Instrument = close to
Scope = far from |
|
|
Which of the following carries a poor outcome for arthroscopic treatment?
a) focal articular lesion b) DJD evidence c) weight bearing lesion d) superficial lesion |
b) DJD evidence
c) weight bearing lesion |
|
|
T or F:
Arthroscopic treatments heal faster than treatments via arthrotomy. |
False!
Usually the healing of the treated lesion is the limiting factor |
|
|
What are some indications/uses for laparoscopy in large animal surgery?
|
Umbilical, bladder sx
Ovariectomy Abdominal cryptorchid OVH Nephrosplenic space ablation Recurrent inguinal hernias Kidney resection Explore/biopsy Remove adhesions |
|
|
How do arthroscopes and laparoscopes differ?
a) size/length is different b) viewing angle is different c) triangulation only used in arthroscopy d) CO2 is not used for insufflation in laparoscopy d/t carbonic acid production |
a) size/length is different
b) viewing angle is different (25-30 degrees in arthroscope; 0 degrees in laparoscope) |
|
|
What are the 3 properties of laser light making it ideal for surgery?
|
Monochromatic (same wavelength)
Coherent (same frequency) Collimated (synchronized wavelengths in one vector) |
|
|
Which of the following are important safety measures for laser surgery?
a) anodized instrumentation b) appropriate signage c) moist drapes d) use of oxygen insufflation e) laser-specific eyewear |
a) anodized instrumentation
b) appropriate signage c) moist drapes e) laser-specific eyewear |
|
|
Which laser type has the most thermal necrosis?
a) laser absorbed well by water b) laser absorbed well by pigment c) short wavelength laser d) long wavelength laser |
b) laser absorbed well by pigment
c) short wavelength laser |
|
|
Which mode of laser emission heats the fastest? Which mode creates the least necrosis?
|
Fastest (continuous)
Less necrosis (Pulsed) |
|
|
Which of the following are NOT true regarding patellar fractures in the horse?
a) usually secondary to OCD b) marked, acute lameness of 4 to 6 of 6 c) skyline view is necessary d) no good way for lag fixation e) fragments within soft tissue are not removed |
a) usually secondary to OCD (TRAUMA)
d) no good way for lag fixation (LAG THE BIG PIECES) |
|
|
Which of the following are NOT true regarding tibial fractures?
a) Nondisplaced midshaft fx cause 6/6 lameness b) distal physeal fx in foals c) Incomplete fx are often spiral d) Salter-Harris type II fractures of lateral aspect in foals e) Complete fractures just above the hock are non-repairable in adults |
a) Nondisplaced midshaft fx cause 6/6 lameness (5/6 LAMENESS; WEIGHTBEARING)
b) distal physeal fx in foals (PROXIMAL PHYSIS) |
|
|
T or F:
Patellar and Tibial fractures in adult horses both have poor prognoses. |
False!
Poor if complete tibial; fair if non-articular patellar. |
|
|
Which of the following are NOT true regarding equine femoral fractures?
a) Oblique fractures in young horses b) Simple fractures in foals c) Comminuted in adults d) May look like hip luxation in foals e) Fair prognoses are only possible with proximal/capital fractures. |
a) Oblique fractures in young horses (SIMPLE)
b) Simple fractures in foals (OBLIQUE) |
|
|
Which of the following are NOT TRUE regarding upward fixation of the patella in horses?
a) lateral incarceration b) straight legs can predispose c) rarely bilateral d) surgical repair is gold standard e) mostly in ponies |
a) lateral incarceration (MEDIAL)
c) rarely bilateral (OFTEN BILATERAL) d) surgical repair is gold standard (ONLY FOR INTRACTABLE/CHRONIC) |
|
|
What are some non-surgical techniques for treating upward fixation of the patella?
|
Benign neglect (will grow out of it)
Flex fetlock and back the up Strengthen quads Inject crap (iodine) Estrogen therapy??? |
|
|
Choose upward patellar fixation, patellar luxation, or BOTH:
Lateral Surgical repair preferred Often bilateral Hypoplasia of trochelar ridge |
(LUXATION) Lateral
(LUXATION) Surgical repair preferred (FIXATION) Often bilateral (LUXATION) Hypoplasia of trochelar ridge |
|
|
Damage to which ligamentous/meniscal stifle structure has a good prognosis?
|
Incompletely torn collateral ligaments
|
|
|
OH NO! Mr. Ed can flex his stifle while extending his hock! What gives? How is this treated?
|
Ruptured pepperonieus tertius;
Allow to rest and it should scar down |
|
|
The peroneus tertius originates on the ________ and inserts on the ___________.
|
Origin (Extensor fossa of femur)
Insert (MT3 and 4th and fibular tarsal bones) |
|
|
Which of the following are associated with a ruptured gastrocnemius tendon in the horse?
a) concurrent SDF rupture b) dropped hock c) good prognosis d) inserts on tuber calcis e) extend hock/flex stifle |
b) dropped hock
c) good prognosis (w/no SDF rupture) d) inserts on tuber calcis |
|
|
Which of the following are NOT true regarding equine skin grafts?
a) partial thickness pinch grafts are most commonly done b) local blocks of graft placement site are necessary c) Inverted L block is ideal for collection site d) grafts should be placed proximal to distal to ensure continued vascularization e) debride placement area 1-2 days before procedure |
b) local blocks of graft placement site are necessary (NO, GRANULATION TISSUE IS NOT INNERVATED)
d) grafts should be placed proximal to distal to ensure continued vascularization (NO, GO DISTAL TO PROXIMAL D/T BLEEDING) |
|
|
What are the 3 ways to perform non-topical local antibiotic therapy?
|
Intra-articular
Regional Abx impregnated PMMA |
|
|
Which antibiotics are often impregnated into PMMA?
|
Gentamycin
Metronidazole |
|
|
Define lameness, punk!
|
Deviation from normal gait, behavior, performance, or MUTHAFLIPPIN POSTURE due to pain or mechanical dysfunction
|
|
|
Choose the AAEP lameness grade associated with:
- Always consistent at a walk - Inconsistent lameness - Consistent lameness in certain circumstances - Non weight-bearing - Consistent at a trot - Minimal weight-bearing |
4 - Always consistent at a walk
1 - Inconsistent lameness 2 - Consistent lameness in certain circumstances 6 (Huber) - Non weight-bearing 3 - Consistent at a trot 5 - Minimal weight-bearing |
|
|
What is probably the most important part of signalment/history in a lameness exam?
|
Use of horse and expectations for future use
|
|

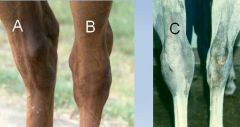
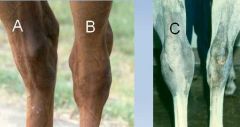
Name the confirmation depicted in each image!
|

A - Base Narrow
B - Base Wide C - Carpus valgus |
|
Describe the swelling depicted for each letter!
|
A - Cellulitis or edema of hock
B - NORMAL (saphenous vein) C - Effusion of tarsal joint |
|

Describe the swelling
|

A - effusion
B - effusion & boxy hock |
|

Describe the swellings
|

A - bowed tendon (swelling proximal to fetlock)
B - effusion of tibiotarsal joint C - stifle effusion (gonitis) |
|

Which is the lame foot?
|

Right!
|
|
|
Which of the following are NOT true regarding equine lameness?
a) in frontlimb lameness, head will nod when sound limb is down b) in frontlimb lameness, head will bob when sound limb is down c) w/no lameness, head moves up and down at the trot d) w/no lameness, hindquarters move up and down at the walk or trot e) hip roll describes the maximal difference between rise and fall of hindquarters |
b) in frontlimb lameness, head will bob when sound limb is down (BOB UP ON LAME LIMB)
c) w/no lameness, head moves up and down at the trot (HEAD IS LEVEL AT TROT; MOVES AT THE WALK) e) hip roll describes the maximal difference between rise and fall of hindquarters (THIS IS HIP EXCURSION) |
|
|
If you see a right hip hike when the left limb is on the ground, where is the lameness?
|
L hind limb lame
|
|
|
If you see a right hip drop when the left limb is on the ground, where is the lameness?
|
R hind limb lame
|
|
|
If you see more left hip excursion when the left hind limb is on the ground than right hip excursion when the right hind limb is on the ground, where is the lameness?
|
L hind limb lame
|
|
|
Which of the following are NOT true regarding congenitally weak flexor tendons?
a) often bilateral b) bandaging and toe extension is key to treatment c) will see a dropped fetlock and sloped pastern with toes pointed up d) unilaterally dropped fetlock may be d/t sesamoid fracture |
b) bandaging and toe extension is key to treatment (DO NOT BANDAGE; NEED TO PROTECT AND EXTEND HEELS)
|
|
|
Choose weak flexors, ruptured extensors, or flexor contractures for the following:
- do not bandage - usually unilateral - treated with tetracycline - often resolves with rest - bandaging/splinting required |
WEAK FLEX- do not bandage
RUPTURE - usually unilateral CONTRACTURES - treated with tetracycline RUPTURE - often resolves with rest CONTRACTURE - bandaging and/or splinting required |
|

What is this and what is it used for?
|

Batame splint; used for fetlock contractures that are over vertical (only leave on for 2-3 hrs at a time)
|
|
|
T or F:
SDF and DDF contracture are congenital issues affecting young horses. |
False! They are acquired (but do affect young horses - DDF 2-8 mos and SDF 10-18mos)
|
|
|
Choose the contracture associated with each of the following:
- high plane of nutrition - fetlock affected - coffin joint affected - 10-18 month foal - club foot - knuckling - toe extension |
SDF and DDF - high plane of nutrition
SDF - fetlock affected DDF - coffin joint affected SDF - 10-18 month foal DDF - club foot SDF - knuckling BOTH - toe extension treatment |
|
|
You hear a clicking/snapping noise coming from the hock region of a horse. How is this treated?
|
NO TREATMENT - snapping hocks is NORMAL
|
|
|
You hear a clicking/snapping noise coming from the rear pastern region of a horse. How is this treated?
|
Transect medial head of DDF
|
|
|
What is the prognosis for an adult with SDF/DDF contracture?
|
Not so good...
|
|
|
Which of the following are NOT true regarding bowed tendons?
a) tendonitis of SDF more common b) hindlimbs and forelimbs equally affected c) low bowed tendon may affect carpal retinaculum d) acute defects are hypoechoic e) rest is important in acute and chronic treatment |
b) hindlimbs and forelimbs equally affected (FORELIMBS>HIND)
c) low bowed tendon may affect carpal retinaculum (HIGH BOW AFFECTS RETINACULUM) |
|
|
For which of the following is a distal check desmotomy an acceptable correction?
a) Clicking pasterns b) bowed tendons c) SDF contracture d) Suspensory desmitis e) DDF contracture |
b) bowed tendons
c) SDF contracture e) DDF contracture (note - clicking pasterns is in the REAR; no check ligaments; however you transect the medial head of the SDF which acts like a desmotomy) |
|
|
Which tendon is more often "bowed" and why?
|
Front SDF @ mid-cannon
Smallest cross-sectional area |
|
|
What are surgical options for chronic bowed tendons?
|
Tendon splitting
Proximal check desmotomy Palmar annular ligament resection (low-bow) |
|
|
Which of the following are true regarding the suspensory ligament?
a) inserts on SDF b) aka interosseous muscle c) inserts on sesamoids d) inserts on common digital extensor e) prevents fetlock overextension |
b) aka interosseous muscle
c) inserts on sesamoids d) inserts on common digital extensor e) prevents fetlock overextension |
|
|
Which of the following are NOT true regarding suspensory desmitis?
a) mid-ligament strain is most common b) most common in the rear c) most common in standardbreds d) tx include shockwave and stem cell injection e) no surgical treatment |
a) mid-ligament strain is most common (ORIGIN)
e) no surgical treatment (NEURECTOMY; Fascial release) |
|
|
What are the 3 etiologies of a breakdown injury?
|
Ruptured suspensory ligament
Bi-axial transverse sesamoid fracture Ruptured distal sesamoidean ligaments |
|
|
What gives in a racehorse with unilaterally, non-weightbearing, dropped front fetlock? How is it treated? What is the prognosis?
|
Traumatic suspensory rupture!
If closed, put in Kimsey Limb-Saver splint then perform arthrodesis of fetlock (guarded prognosis) |
|
|
Lacerations of which tendons have the best prognosis? Why is this so?
|
Extensor tendons! They have no tendon sheaths and horses rely more on their flexors.
|
|
|
What are the extensor tendons in the front? The rear?
|
Front (Common digital, lateral digital)
Rear (Peroneus tertius, long digital, lateral digital) |
|
|
How are extensor lacerations treated? What is the prognosis?
|
Clean/debride under GA
Cast in extension (maybe toe extension) Usually NOT sutured Favorable prognosis! |
|
|
What are the flexors?
|
SDF, DDF, Suspensory
|
|
|
Choose the lacerated structures for each of the following:
- fetlock drops to ground - fetlock drop, toe is up - mild fetlock drop |
SDF/DDF/Suspensory- fetlock drops to ground
SDF/DDF- fetlock drop, toe is up SDF- mild fetlock drop |
|
|
How are flexor lacerations treated?
|
Clean/debride under GA
Suture tendon ends Cast in flexion (elevate heel) Guarded prognosis... |
|
|
Which suture types are good for flat tendons? Round? What suture material should be used?
|
Triple pulley (round)
Locking Loop (flat) Use PDS or Nylon |
|
|
Which of the following are indications for a Caslick procedure?
a) gill flirter b) prevent CEM c) urine pooling d) windsucking e) infertility |
a) gill flirter
d) windsucking e) infertility |
|
|
How is urine pooling treated?
|
Improve body condition
Perineal reconstruction Urethral extension Transverse fold reposition |
|
|
What must you do to a filly before importing into the US or France?
|
Clitoral Sinusectomy - OUCH
|
|
|
Choose the correct type of perineal laceration associated with each of the following:
- feces in vaginal vault - forgot to take Caslick out! - through mucous membrane and part of perineal body - makes a cloaca - typically needs no repair |
3rd degree or rectovaginal fistula - feces in vaginal vault
1st degree- forgot to take Caslick out! 2nd degree - through mucous membrane and part of perineal body 3rd degree- makes a cloaca 1st/2nd degree - typically needs no repair |
|
|
How are 3rd degree perineal lacerations treated?
|
Minimal debridement
Systemic abx (penicillin) Oxytocin for uterine contraction Manual evacuation of feces Prevent constipation Pain control! Surgical repair @ 6 wks |
|
|
Which of the following are NOT true regarding C-sections in the mare?
a) often compromises further fertility b) Ventral midline approach is preferred c) Due to its epitheliochorial nature, the placenta should be removed d) 3 layer closure of the uterus is performed e) incise uterus on antimesenteric side |
a) often compromises further fertility (NOT IF DONE IN A TIMELY MANNER)
c) Due to its epitheliochorial nature, the placenta should be removed (NO WAY) d) 3 layer closure of the uterus is performed (KINDA WRONG - use ford interlocking/continuous on cut edges first then appositional pattern w/oversew) |
|
|
What is the most common type of fracture in the foal?
|
Salter-Harris II
|
|
|
Which of the following are NOT true regarding ovariectomy?
a) Pack animal indication b) colpotomy via ecraseur is preferred for tumor removal c) always put 20cc bupivicaine in each pedicle d) Granulosa thecal cell tumor most common ovarian tumor e) most commonly performed for cystic ovaries |
b) colpotomy via ecraseur is preferred (NO WAY; USE LAPAROSCOPY/LAPAROTOMY)
e) most commonly performed for cystic ovaries (NO WAY; CYSTIC OVARIES ARE REALLY RARE IN HORSES) |
|
|
What are some signs of granulosa cell tumors in horses?
|
Stallion-like behavior
Unilaterally enlarged ovary w/o palpable ovulation fossa Irregular estrus Elevated T2 and Inhibin in blood |
|
|
Which of the following are indications for standing laparoscopic ovary removal?
a) maiden mare b) large tumors c) Mare wants to kill you |
a) maiden mare
|
|
|
You see a mare in late pregnancy with a really really big abdomen that seems pulled cranioventrally. What gives?
|
...probably ruptured prepubic tendon
|
|
|
Choose the type of cutaneous neoplasia associated with:
- most common horse neoplasm - most common ocular tumor - often left untreated - non-pigmented areas - BPV |
SARCOID - most common horse neoplasm
SCC - most common ocular tumor LSA/MELANOMA/some sarcoids - often left untreated SCC - non-pigmented areas SARCOID- BPV |
|
|
Choose the type of cutaneous neoplasia associated with:
- regressin immunotherapy - usually young QH - black - subcut nodules over most of horse - usu on head, neck |
SCC/SARCOID - regressin immunotherapy
SARCOID - usually young QH MELANOMA - black LSA - subcut nodules over most of horse SARCOID - usu on head, neck |
|
|
What are the forms of equine sarcoid? Which is most benign and most severe?
|
Fibroblastic (SEVERE)
Mixed Nodular Verrucous (moderate) Flat (benign) |
|
|
What is important when diagnosing equine sarcoids?
|
COMPLETE EXCISIONAL BIOPSY - partial biopsy stimulates growth
|
|
|
T or F:
Sarcoids don't kill horses but many horses w/sarcoids are killed. |
Yup.
|
|
|
Which of the following are NOT true regarding equine sarcoids?
a) Laser and cryosurgery after debulkng have a 20-30% recurrence b) Cisplatin is best for eyelid sarcoids c) Flat and verrucous sarcoids are often not treated d) 1 or 2 doses of regressin are sufficient for regression e) Testing for BPV can predict sarcoid susceptibiltiy |
b) Cisplatin is best for eyelid sarcoids (REGRESSIN)
d) 1 or 2 doses of regressin are sufficient for regression (3-5 TREATMENTS) e) Testing for BPV can predict sarcoid susceptibiltiy (NO!) |
|
|
Cimetidine may be used to treat which cutaneous neoplasm?
|
Melanoma
|
|
|
Which of the following are NOT true about camelid dentition?
a) no incisors b) dental pad c) 6 fighting teeth d) fighting teeth commonly removed e) most common molar to extract is mandibular M2 |
a) no incisors (Upper incisor IS a fighting tooth)
d) fighting teeth commonly removed (NO - they're are clipped) |
|
|
Which of the following are NOT true regarding camelid orthopedics?
a) cannot often perform periosteal stripping b) carpus varus is common c) they're the cats of the large animal world d) transphyseal bridging is used to correct physeal ectasia e) carpus valgus is treated by transphyseal bridging and ulnar ostectomy |
b) carpus varus is common (CARPUS VALGUS)
d) transphyseal bridging is used to correct physeal ectasia (NO SURGERY FOR THIS; USE DIET/VIT D) |
|
|
If you castrate a llama before ____ months, the growth plates won't close.
|
<18 mos
|
|
|
What should you do if you see a male llama with urethral calculi?
|
RUN THE OTHER WAY - tough to deal with!
|
|
|
How can uterine torsion be corrected in camelids?
|
Rolling (flex limbs first)
Ventral midline celiotomy |