Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
45 Cards in this Set
- Front
- Back
|
When compared with a man, the chances that a woman will develop major depressive disorder, dysthymic disorder, or bipolar disorder over the course of her lifetime are, respectively
(A) higher, higher, equal (B) higher, higher, lower (C) higher, equal, higher (D) higher, higher, higher (E) equal, higher, equal (F) equal, higher, lower (G) equal, equal, equal |
Higher, Higher, Equal
|
|
|
What are the mood or affective disorders characterized by?
|
Primary disturbance in internal emotional state, causing subjective distress and problems in functioning
|
|
|
What is the term for when a patient emotionally feels somewhat worse than would be expected?
|
Dysthymia
|
|
|
What is the term for when a patient emotionally feels very much worse than would be expected?
|
Depression
|
|
|
What is the term for when a patient emotionally feels somewhat better than would be expected?
|
Hypomania
|
|
|
What is the term for when a patient emotionally feels very much better than would be expected?
|
Mania
|
|
|
What are the DSM-IV-TR categories of mood disorders?
|
Primary Mood Disorders:
- Major depressive disorder - Bipolar disorder (I and II) - Dysthymic disorder - Cyclothymic disorder Secondary Mood Disorders: - Owing to a general medical condition - Substance-induced mood disorder |
|
|
What are the differences in occurrence of mood disorders baed on ethnicity, education, marital status, and income?
|
No differences in occurrence based on these factors
|
|
|
What is the lifetime prevalence of major depressive disorder in males vs females?
|
- 5-12% for men
- 10-20% for women |
|
|
What is the lifetime prevalence of bipolar disorder in males vs females?
|
- 1% overall
- No sex difference |
|
|
What is the lifetime prevalence of dysthymic disorder in males vs females?
|
- 6% overall
- Up to 3x more common in women |
|
|
What is the lifetime prevalence of cyclothymic disorder in males and females?
|
- <1% overall
- No sex difference |
|
|
What are the characteristics of major depressive disorder?
|
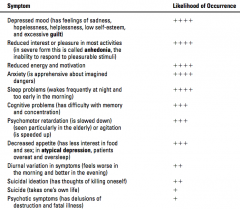
Recurrent episodes of depression, each continuing for at least 2 weeks
Approximate percentage of patients in which sign of symptom is seen: + = <25% ++ = 50% +++ = 70% ++++ = >90% |
|
|
What is "masked depression"? How common?
|
- Depressed patients who seem unaware of or deny depression
- Often present to PCP complaining of vague physical symptoms - As many as 50% of depressed patients |
|
|
How can "masked depression" present to the doctor? What can it be confused with?
|
- Often present to PCP complaining of vague physical symptoms
- May be mistaken for hypochondriasis |
|
|
How do depressed patients differ from patients with hypochondriasis?
|
- Depressed patients show other symptoms of depression (eg, severe weight loss, suicidality) in addition to their physical complaints
- Patients with hypochondriasis only have physical complaints |
|
|
What is Seasonal Affective Disorder (SAD)? Characteristics?
|
Subtype of major depressive disorder that is associated with the winter season and short days
- Characterized by atypical symptoms of depression (eg, oversleeping and overeating) and a heavy feeling in the limbs ("leaden paralysis") |
|
|
What is the suicide risk associated with Major Depressive Disorder?
|
- Patients with MDD at increased risk for suicide
- Certain demographic, psychosocial, and physical factors affect this risk |
|
|
What are the top five risk factors for suicide from highest to lowest?
|
1. Serious prior suicide attempt
2. Age >45 years 3. Alcohol dependence 4. History of rage and violent behavior 5. Male sex |
|
|
What are the types of Bipolar Disorder?
|
Bipolar I Disorder:
- Episodes of both mania and depression Bipolar II Disorder: - Episodes of both hypomania and depression |
|
|
Is there a disorder of just manic episodes?
|
No simple manic disorder, because depressive symptoms eventually occur (therefore one episode of symptoms of mania alone or hypomania plus one episode of major depression defines bipolar disorder)
|
|
|
Do psychotic symptoms occur in Bipolar Disorder?
|
Psychotic symptoms, such as delusions, can occur in depression as well as in mania
|
|
|
What are the symptoms of mania?
|
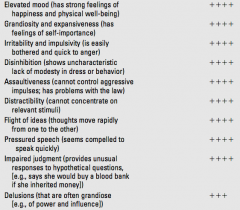
Approximate percentage of patients in which sign of symptom is seen:
+ = <25% ++ = 50% +++ = 70% ++++ = >90% |
|
|
When is a patient with a mood disorder more likely to be misdiagnosed as schizophrenia?
|
Some patients (eg, poor patients with low access to healthcare) with a mood disorder with psychotic symptoms can be severe enough that it is misdiagnosed
|
|
|
What is a key difference between mood disorders with psychotic symptoms and patients with true schizophrenia or schizoaffective disorders?
|
In mood disorders, the patient's mood and functioning usually return to normal between episodes
|
|
|
What is dysthymic disorder?
|
Dysthmia (feeling somewhat worse than would be expected) over a 2-year period (1-year in children) with no discrete episodes of illness
|
|
|
What is cyclothymic disorder?
|
- Periods of hypomania and dysthymia
- Occurs over a 2-year period (or 1-year in children) - No discrete episodes of illness |
|
|
What is the difference between major depressive disorder and dysthymic disorder, as well as between bipolar disorder and cyclothymic disorder?
|
Dysthymic and Cyclothymic disorders are less severe, non-episodic, chronic, and never associated with psychosis or suicide
|
|
|
What does the biologic etiology of mood disorders include?
|
- Altered NT activity
- Genetic component (strongest in bipolar) - Physical illness and related factors - Abnormalities of limbic-hypothalamic-pituitary-adrenal axis |
|
|
What does the psychosocial etiology of depression and dysthymia include?
|
- Loss of parent in childhood
- Loss of spouse or child in adulthood - Loss of health - Low self-esteem and negative interpretation of life events - Learned helplessness (ie, because attempts to escape bad situations in the past have proven futile, person now feels helpless) |
|
|
What medical conditions must be included in the differential diagnosis of depression?
|
- Cancer (particularly pancreatic and other GI tumors)
- Viral illness (eg, pneumonia, influenza, AIDS) - Endocrine abnormalities (eg, hypothyroidism, diabetes) - Neurologic illness (eg, Parkinson disease, Huntington disease, stroke - particularly left frontal) - Nutritional deficiency (eg, folic acid, B12) - Renal or cardiopulmonary disease |
|
|
Which psychiatric and pharmacologic conditions must be included in the differential diagnosis of depression?
|
- Schizophrenia (particularly after an acute psychotic episode)
- Anxiety disorder - Somatoform disorder - Eating disorder - Drug and alcohol abuse (particularly use of sedatives and withdrawal from stimulants) - Prescription drug use (eg, reserpine, steroids, anti-HTNs, anti-neoplastics) |
|
|
How do psychosocial factors affect the etiology of mania or hypomania?
|
Psychosocial factors are not involved
|
|
|
How common is treatment sought and received for patients with depression? How effective?
|
- 25% of patients with depression seek and receive treatment (many do not seek treatment because they believe it indicates personal failure or weakness)
- Depression is successfully treated in most patients |
|
|
What are the characteristics of untreated episodes of depression and mania? How long?
|
- Self-limiting
- Depressive episodes last approximately 6-12 months - Manic episodes last approximately 3 months |
|
|
What are the most effective treatments for mood disorders?
|
Pharmacologic
|
|
|
What are the types of pharmacologic treatments for depression and dysthymia?
|
Antidepressant agents
- Heterocyclics - SSRIs and SNRIs - MAOIs - Stimulants |
|
|
What are the mood stabilizers? Use?
|
- Lithium and anti-convulsants such as Carbamazepine and Divalproex used to treat bipolar disorder
- Also used for cyclothymic disorder (in similar doses) - Atypical antipsychotics (eg, Olanzapine and Risperidone) - Sedative agents (eg, Lorazepam) used to treat acute manic episodes because they resolve symptoms quickly |
|
|
What are the types of psychological treatments used for depression and dysthymia? Efficacy?
|
- Psychological treatment for depression and dysthymia includes psychoanalytic, interpersonal, family, behavioral, and cognitive therapy
- Psychological treatment in conjunction with medication is more effective than either type of treatment alone |
|
|
What is the primary indication for Electroconvulsive Therapy?
|
Major depressive disorder
|
|
|
When is Electroconvulsive Therapy used?
|
- When symptoms of MDD do not respond to anti-depressant meds
- When anti-depressants are too dangerous or have intolerable side effects (eg, particularly useful for elderly patients) - When rapid resolution of symptoms is necessary (eg, patient is acutely suicidal or psychotic) |
|
|
A 22-year-old male college student is taken to the emergency department by police because he tried to enter a state office build- ing to “have a conference with the governor” about conducting a fund drive to “finance my cure for cancer.” When police prevent him from entering the building, he becomes irritable and hostile and resists attempts to restrain him.
The most appropriate diagnosis for this patient is (A) dysthymic disorder (B) major depressive disorder (C) bipolar disorder (D) hypochondriasis (E) cyclothymicdisorder |
B - bipolar disorder
This patient is most likely to have bipolar I disorder. While this disorder involves episodes of both mania and depression, a single episode of mania defines the illness. The beliefs that one is important enough to demand a conference with the governor and cure cancer are grandiose delusions. Schizophrenic delusions are commonly paranoid in nature. Irritability and hostility are also common in a manic episode. |
|
|
A 22-year-old male college student is taken to the emergency department by police because he tried to enter a state office build- ing to “have a conference with the governor” about conducting a fund drive to “finance my cure for cancer.” When police prevent him from entering the building, he becomes irritable and hostile and resists attempts to restrain him.
The most effective long-term treatment for this patient is (A) a heterocyclic antidepressant (B) lithium (C) electroconvulsive therapy (D) psychotherapy (E) a monoamine oxidase inhibitor |
B - Lithium
Of the listed treatments, the one most effective for bipolar disorder is lithium. Heterocyclic antidepressants, electroconvulsive therapy, monoamine oxidase inhibitors, and psychotherapy are used primarily to treat depression. Antidepres- sants and psychotherapy are used to treat dysthymia. |
|
|
A 22-year-old male college student is taken to the emergency department by police because he tried to enter a state office build- ing to “have a conference with the governor” about conducting a fund drive to “finance my cure for cancer.” When police prevent him from entering the building, he becomes irritable and hostile and resists attempts to restrain him.
This college student has two brothers. The first is his monozygotic twin; the second is two years younger. The risks that his first and second brothers will develop bipolar disorder are respectively about (A) 75% and 60% (B) 75% and 20% (C) 60% and 10% (D) 50% and 10% (E) 10% and 1% |
B - 75% and 20%
The chances of the monozygotic twin and first-degree relative (e.g., brother) of this bipolar patient developing the disorder are about 75% and 20%, respectively. |
|
|
A 52-year-old overweight man reports that he often wakes up with a headache. He also notes that he is tired all the time and repeatedly falls asleep during the day. Evaluation of the arte- rial blood of this patient is most likely to reveal
(A) respiratory acidosis (B) respiratory alkalosis (C) metabolic alkalosis (D) increased PaO2 (E) decreased PaCO2 |
The answer is A.
This overweight middle-aged male patient is likely to have sleep apnea. Like other patients with pulmonary disorders leading to depressed breathing, patients with sleep apnea typically show chronic respiratory acidosis (increased partial pressure of carbon diox- ide [PaCO2]). Respiratory alkalosis (decreased PaCO2) results from hyperventilation as a result of anxiety, high fever, or stimulant abuse. Metabolic alkalosis typically results from excessive vomiting and resulting hypokalemia (and see answers to questions 9 and 10). |