Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
All motor nuclei are grouped where in the spinal cord?
What can you say about their arrangement? |
All motorneurons innervating one muscle grouped together within a motor nucleus in the anterior horn of spinal grey matter.
They are arranged somatotropically! |
|
|
|
Define a motor unit. What can you say about the fibers involved?
|
Motorunit = motorneuron and all the muscle fibers that it innervates. Includers 10-100 fibers all of the SAME histological type!
|
|
|
|
Why do fast glycolytic fibers fatigue quickly?
|
Fast glycolytic fibers have little or no myoglobin (makes them pale) and few mitochondria, they thus rely on glycolytic metabolism and the fatigue rapidly when this causes a build-up of lactic acid.
|
|
|
|
The diameter of a motorneuron is proportional to what?
|
The speed of the fiber that it innervates:
small diameter = slow oxidative intermediate diameter = fast oxid/glycolytic large diameter = fast glycolytic |
|
|
|
What is the size principal of motorneurons?
|
Small diamter motorneurons (innervate slow msk fibers) are more excitable and are thus the 1st to be recruited by relatively low levels of excitatory synaptic input. Large diameter m.neurons (and their fast glycolytic fibers) are therefore the last to be recruited.
|
|
|
|
What are Renshaw cells and what do they do?
|
Inhibitory interneurons that lie adjacent to motor nuclei. They get stimulated by collateral axons of Mneurons and cause inhibitory feedback to limit m.neuron d/c rate
|
|
|
|
What is meant by "motorneuron Bistability". What is the purpose of this phenomena?
|
Following strong excitation the membrane of a Mneuron will stay depolarized to just below threshold. This makes it more easily excitable = allows for tonic contraction of postural muscles
|
|
|
|
What do gamma motor neurons do?
where are they found? What happens when they are stimulated? |
detect the amount and rate of change in muscle length (proprioception). They are found in muscle spindles. When they are stimulated they contract, pull on the spindle and make it more sensitive.
|
|
|
|
If you have excessive flexion at a joint - what 2 reflexes would correct this and how? (ie which 2 sensory afferent fibers)
|
Ia fibers in the muscle spindle would sense the stretch in the extensors and would trigger their (antagonistic) contraction.
Ib fibers in the golgi tendon organ, would sense the extensor tendon tension and use an inhibitory interN to suppress the a-motorN |
|
|
|
Describe the property of reciprocal inhibition.
|
activation of one motor nucleus is coupled to inhibition of antagonistic motor nucleus. (eg. activation of flexors will inhibit extensors)
** suppressed when you want to make the joint stiff (need to activate both groups) |
|
|
|
If the babinski reflex is +ve.... what do the toes do when stroked?
What does this mean? Ie where is there damage? |
The toes will extend (withdraw). A normal Babinski is to plantarflex.
If the toes dorsiflex then there has been damage to the corticospinal tract. |
|
|
|
What is the main mechanism for regulating and switching reflex effects?
|
Presynaptic inhibition of an afferent or interNeuron. This is more precise that post-synaptically inhibiting a whole neuron (b/c that will block each on of it's axonal targets - pre-synaptic block only one axonal target).
|
|
|
|
What causes motion sickness?
|
visual and somatosensory inputs are constantly being reweighted according to congruence with vestibular reference. Persistant incongruence between the two will elicit motion sickness.
|
|
|
|
When you close your eyes stading up - you will sway. How can you correct this? Make it worse?
|
Correct by touching a surface - not for stability but rather for somatosensory input.
Closing your eyes will make it 2x worse. |
|
|
|
define synergy?
What is the difference between the synergies that are organized by the reticulospinal vs. the rubrospinal tracts? |
Synergy = group of muscles contracting simultaneously in a specific motor act
Reticulospinal - very widespread (1/2 body) postural Rubrospinal - highly localized |
|
|
|
What are the 4 features of a medial medullary syndrome?
|
1. Ipsilateral paresis (d/t CN motor nuclei)
2. Atrophy & fibrillation of the tongue 3. Contralateral hemiplegia (b/c lost ↓ motor tracts during decussation), face spared! 4. Contralateral loss of position & vibration senses |
1.ipsilateral.......
2. Tongue? 3. contralateral......... with what spared? 4. contralateral......... |
|
|
For the stretch reflex state the:
- stimulus - response - function |
- passive stretch by a load or antag muscle contraction
- active contraction of the muscle (v. fast b/c spindle aff Ia has monosynaptic conection to motorN) - maintains joint position |
|
|
|
For the golgi tendon reflex state the:
- stimulus - response - function |
- stimulus: tension in the muscle tendon
- response: IIb uses an inhibitory interN to inhibit the a-motorN's = relaxation - function: maintains joint angle following overcorrection |
|
|
|
For the flexion withdrawel reflex state the:
- stimulus - response - function |
- stimulus: noxious injury of a limb
- response: extension distally, flexion proximally - function: drop the load and pull limb away! ** extensors get activated on opposite side to maintain balance |
|
|
|
For the neck flexion reflex state the:
- stimulus - response - function |
- stimulus: neck flexion
- response: facilitates flexion in rest of body - function: flex your head in an arm wrestle * same with other extension! |
|
|
|
For the vestibulospinal reflex state the:
- stimulus - response - function` |
- stimulus: ↓ward deviation on one side of head activates otolith
- response: contract extensors (antigravity) of the same side - function: maintain balance |
|
|
|
For the vestibulo-ocular reflex, name the:
-stimulus - response - function |
-stimulus: angular rotation of the head activates semicircular canals
- response: extra-occular eye movements in opposite direction - function: keeps gaze steady while head turns (can override) |
|
|
|
For the visual postural reflex, name the:
-stimulus - response & function |
-stimulus: perception of the vertical axis
- response: compliments other reflexes to align body with perceived axis |
|
|
|
What are the "two" pendulums in the pendulum model of locomotion?
|
During the swing phase, the leg is the pendulum, but during the stance phase the leg is an inverted pendulum and the body swings over it.
|
|
|
|
What are the 2 "half centres" of the locomotion CPG's?
How do they relate to each other? |
1. Flexor burst - drives flexor motor nuclei
2. Extensor burst - drives extensors * these mutually inhibit eachother and both are spontaneously active when not inhibited |
|
|
|
Flexor burst generator:
- how long does this phase last? - how is it shut-off? |
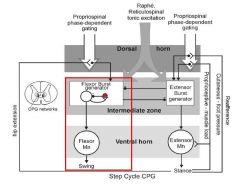
Flexor burst generator:
- has a fixed duration regardless of speed of locomotion - eventually shuts itself off = loss of reciprocal inhibition = extensor network gets activated |
|
|
|
For the stance phase of walking, describe:
-duration & regulation - pertinent reflexes |
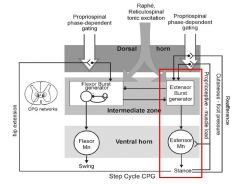
- duration will depend on speed of locomotion, regulated by sensory feedback
- when foot lands it suddenly takes the whole load of the body - triggers the stretch reflex and body gets propelled (therefore propulsion ~ load) |
|
|
|
How does the body transition to the swing phase? (3 conditions must be met...)
|
After toe off, these 3 condition must be met in order to disinhibit the flexor burst generator:
1. leg not bearing wt 2. hip extended 3. opposite leg bearing wt |
|
|
|
describe arm swing during walking
|
flexion phase is synchronized diagonally between arms and legs, via propriospinal tracts that link one segment of cord to another.
|
|
|
|
What is the role of the midbrain in walking?
What control speed? Pattern generation? |
Midbrain is the switch that turns on reticulospinal CPGs. It governs the speed of locomotion (using impulse rate) but NOT the pattern generation!
|
|
|
|
What is the cortical contribution to locomotion?
|
The cortex activates tibialis anterior --> dorsiflexion to prevent the foot from scraping. This is why stroke often = foot drop
|
|
|
|
The basal ganglia are involved in voluntary initiation of movement. What is the direct pathway involved in this?
|
When the striatum gets activated (d/t convergence of sensory input) it will inhibit the pallidum. Turning the pallidum off with disinhibit all the motor centers that the pallidum was inhibiting. The direct pway = "go" pathway
|
|
|
|
The indirect pathway in the basal ganglia goes between the striatum and the pallidum. Is it a "go" or "stop" pathway? How does it work (ie what's involved)?
|
The Globus pallidum externa inhibits the subthalamic nuclei. When the striatum gets activated it will inhibit the GPE = disinhibition of the STN. Newly freed, the STN will activate the GPinterna, and the Subst Nigra R ===> increased inhibition of premotor centres.
** antagonizes the direct pathway! |
|
|
|
How is the striatum activated? How does it learn?
|
The striatum is activated by dopamine that is released from the substantia nigra. These dopaminergic neurons respond preferentially to rewards. Thus rewards facilitate the striatum so that it can learn new input strategies. (dopamine cements connections that are right).
|
|
|
|
Symptoms of Parkinsons occur following the loss of what 3 things?
( 3 NT, their source and the effect of their loss) |
1. Dopamine from sub nigra and VTA - low dopamine makes it difficult to initiate d/c from striatal cells = direct pway suppressed & indirect pway unopposed
2. Noradrenergics in locus cerulus - loss of reticular activating system 3. Cholinergics in PPN - decreased facilitation of dopamine release |
|
|
|
What are the 4 symptoms of parkinsons disease? Why does each occur?
What is another common problem and how can pt's manage this problem? |
1. Akinesia - b/c unable to activate the striatum
2. Bradykinesia - slow b/c insuff pallidum inhibition 3. Tremor - subthalamic nuclei gets hyperpolarized then starts to oscillate 4. RIgidity - ? source, maybe PPN * Also get a loss of automatic routines ---> must break them down into individual commands for the pt |
|
|
|
What is Huntington's disease (symtoms)? What causes it?
|
In huntington's disease there is a loss of indirect pway projection neurons from the striatum. Thus the direct pway dominates and the pallidum is hypoactive = excessive, unopposed movments
|
|
|
|
What type of lesion causes Hemiballismus? What is the natural history of it?
|
Hemiballismus is caused by a lesion in the subthalamic nuclei such that it can't activate the pallidum = a loss of tonic inhibition from the pallidum = premotors disinhibited and you get spontaneous full-force movements. Resolves on its own as pallidum restores background activity by itself.
|
|
|
|
What are 2 functions that arise from the antagonism between direct and indirect pways?
|
1. Selection of motor action - inhibiting only a small zone within the pallidum
inhibition from direct pway is limited by an envelop of excitation from indirect pway 2. Modulation of motor action velocity - summation of 2 pways will determine velocity |
|
|
|
What is the relationship between the cerebral cortex & Bstem, cerebellar cortex, nuclei and the motor centres?
|
Input from the cerebral cortex, and brainstem get relayed in the pons. This input is then carried to the cerebellar cortex which when activated will inhibit the nuclei (via Purkinje + GABA). The nucleus provides excitatory output to motor centres
|
|