Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
518 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Qualitative?
|
•Non-numerical
•Based on direct observation •Equipment not necessary •Focus on time and space •Examples: –Rotation of femur during golf swing –Adduction of humerusduring freestyle swim |
|
|
|
Quantitative
|
•Numerical
•Based on data collected •Equipment necessary •Focus on forces •Examples: –Stress on shoulder during baseball pitch –Compression force on femur during landing |
|
|
|
Kinesiology
|
–Scientific study of human movement
–Anatomical, physiological, psychological, biomechanical |
|
|
|
Biomechanics
|
–Application of mechanics to biological systems
–More specific than kinesiology |
|
|
|
Kinematics
|
–Examines space and time
|
|
|
|
Kinetics
|
–Examines forces
|
|
|
|
Dextro
|
–relating to, or situated to the right or on the right side of something
|
|
|
|
Levo
|
–relating to, or situated to the left or on the left side of something
|
|
|
|
Volar
|
–relating to palm of the hand or sole of the foot
•Plantar |
|
|
|
Types of Bones?
|
•Long bones -humerus, fibula
•Short bones -carpals, tarsals •Flat bones -skull, scapula •Irregular bones -pelvis, ethmoid, ear ossicles •Sesamoid bones -patella |
|
|
|
Endochondral bones
|
–develop from hyaline cartilage
–hyaline cartilage masses at embryonic stage |
|
|
|
3 major classifications according to structure & movement characteristics
|
–Synarthrodial
–Amphiarthrodial –Diarthrodial |
|
|
|
Synarthrodial
|
•immovable joints
•Suture such as Skull sutures •Gomphosis such as teeth fitting into mandible or maxilla |
|
|
|
Amphiarthrodial
|
•slightly movable joints
•allow a slight amount of motion to occur –Syndesmosis –Synchondrosis –Symphysis |
|
|
|
Syndesmosis
|
Two bones joined together by a strong ligament or an interosseus membrane that allows minimal movement between the bones
–Bones may or may not touch each other at the actual joint –Ex. Coracoclavicular joint, distal tibiofibular jt. |
|
|
|
Synchondrosis
|
Typeofjointseparatedbyhyalinecartilagethatallowsveryslightmovementbetweenthebones
–Ex.costochondraljointsoftheribswiththesternum |
|
|
|
Symphysis
|
–Joint separated by a fibrocartilage pad that allows very slight movement between the bones
–Ex. Symphysis Pubis& intervertebral discs |
|
|
|
Diarthrodial Joints
|
•known as synovial joints
•freely movable •composed of sleevelike joint capsule •secretes synovial fluid to lubricate joint cavity •capsule thickenings form tough, nonelastic ligaments that provide additional support against abnormal movement or joint opening |
|
|
|
Degrees of freedom
|
–motion in 1 plane = 1 degree of freedom
–motion in 2 planes = 2 degrees of freedom –motionin3planes=3degreesoffreedom |
|
|
|
Diarthrodial Joints - six types?
|
–Condyloid (knuckle joint)
–Enarthrodial (ball and socket) –Sellar (saddle - only in the 1st carpometacarpal) –Arthrodial (glinding) –Ginglymus (hinge joint) –Trochoid (pivot joint) |
|
|
|
Osteokinematic motion
|
resulting motion of bones relative to 3 cardinal planes from these physiological
|
|
|
|
Arthrokinematics
|
motion between articular surfaces
|
|
|
|
3 specific types of accessorymotion
|
–Spin
–Roll –Glide |
|
|
|
Isometric contraction
|
Isometric contraction
– tension is developed within muscle but joint angles remain constant – static contractions – significant amount of tension may be developed in muscle to maintain joint angle in relatively static or stable position – may be used to prevent a body segment from being moved by external forces |
|
|
|
• Isotonic contraction
|
developing tension to either cause or control
joint movement – dynamic contractions – the varying degrees of tension in muscles result in joint angles changing • Isotonic contractions are either concentric or eccentric on basis of whether shortening or lengthening occurs |
|
|
|
Concentric contractions
|
– muscle develops tension as it
shortens – occurs when muscle develops enough force to overcome applied resistance – causes movement against gravity or resistance – described as being a positive contraction – force developed by the muscle is greater than that of the resistance – results in joint angle changing in the direction of the applied muscle force – causes body part to move against gravity or external forces |
|
|
|
Eccentric contraction (muscle action)
|
– muscle lengthens under tension
– occurs when muscle gradually lessens in tension to control the descent of resistance – weight or resistance overcomes muscle contraction but not to the point that muscle cannot control descending movement – controls movement with gravity or resistance – used to decelerate body segment movement – Some refer to this as a muscle action instead of a contraction since the muscle is lengthening as opposed to shortening – described as a negative contraction – force developed by the muscle is less than that of the resistance |
|
|
|
Kinesthesis
|
conscious awareness of
position & movement of the body in space. Through proprioceptors. |
|
|
|
• the types of Proprioceptors specific to joints & skin?
|
. Meissnerfs corpuscles
. Ruffinifs corpuscles . Pacinian corpuscles . Krausefs end]bulbs |
|
|
|
Proprioception
|
– Subconscious mechanism by which body is able
to regulate posture & movement by responding to stimuli originating in proprioceptors of the joints, tendons, muscles, & inner ear |
|
|
|
• Phases of a single muscle fiber contraction
or twitch? |
– Stimulus
– Latent period – Contraction phase – Relaxation phase |
|
|
|
• the types of Proprioceptors specific to joints & skin?
|
. Meissnerfs corpuscles
. Ruffinifs corpuscles . Pacinian corpuscles . Krausefs end]bulbs |
|
|
|
Proprioception
|
– Subconscious mechanism by which body is able
to regulate posture & movement by responding to stimuli originating in proprioceptors of the joints, tendons, muscles, & inner ear |
|
|
|
• Phases of a single muscle fiber contraction
or twitch? |
– Stimulus
– Latent period – Contraction phase – Relaxation phase |
|
|
|
If angle is LESS than 90 degrees,
the force is a ________because its pull/ directs the bone toward the joint axis |
stabilizing force
|
|
|
|
If angle is GREATER than 90
degrees, the force is ________ due to its pull directing the bone away from the joint axis |
dislocating
|
|
|
|
Uniarticular muscles
|
– Cross & act directly only on the joint that they
cross – Ex. Brachialis |
|
|
|
Biarticular muscles
|
cross & act on two
different joints – Depending, biarticular muscles may contract & cause motion at either one or both of its joints |
|
|
|
Multiarticular muscles
|
on three or morejoints due to the line of pull between their origin & insertion crossing multiple joints
|
|
|
|
Active insufficiency
|
reached when the muscle becomes shortened to the point that it
can not generate or maintain active tension |
|
|
|
Passively insufficiency
|
reached when the opposing muscle becomes stretched to the point where it can no longer lengthen & allow
movement |
|
|
|
Three major types of muscle fibers:
|
Type I, IIa, IIb.
|
|
|
|
Type I
|
Contraction velocity- Slow-twitch oxidative (OS)
Contraction force-Slow Fatigability- Fatigue resistant |
|
|
|
Type IIa
|
Contraction velocity- Fast-twitch oxidative-glycolytic(FOG)
Contraction force - Moderately fast Fatigability- Somewhat fatigue resistant |
|
|
|
Type- IIb.
|
Contraction velocity- Fast-twitch glycolytic(FG)
Contraction force-Fast Fatigability- Rapidly fatiguing |
|
|
|
Distal maleoli (of tibia and fibula) serve as _____ for _______to increase _____ of muscles in performing inversion & eversion actions
|
pulley
posterior tendons mechanical advantage |
|
|
|
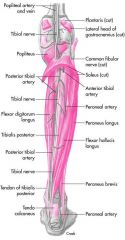
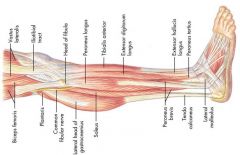
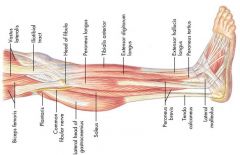
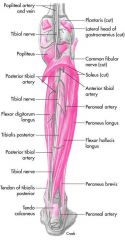
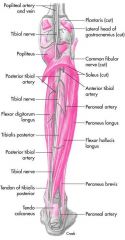
lateral malleolus -posterior tendons?
|
Peroneus brevis & peroneus longus
|
|
|
|
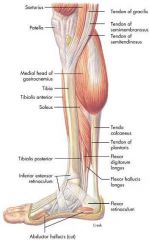
medial malleolus -posterior tendons?
|
•“Tom, Dick & Harry”
–Tibialis posterior –Flexor digitorum longus –Flexor hallucis longus |
|
|
|
Function of the tuberosity of the 5th metatarsal?
|
insertion for peroneus brevis & tertius (and abductor digiti minimi)
|
|
|
|
what is the advantage of pennate muscles?
|
Force depends on the angle. The grater the angle the the lower the force transmitted to the tendon and thus the greater the higher the maximum capable force. There is a higher number of fibres compared to a fusiform muscle.
|
|
|
|
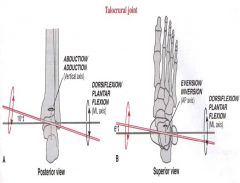
Degrees of movement of talocrural joint?
|
–50 degrees of plantar flexion
–15 to 20 degrees of dorsiflexion –Greater range of dorsiflexion with knee flexed (reduces gastroc tension) –Fibula rotates 3 to 5 degrees externally with ankle dorsiflexion & 3 to 5 degrees internally during plantarflexion |
|
|
|
movement of subtalar & transverse tarsal joints? (degrees)
|
–Inversion & eversion occurs here
–Classified as gliding or arthrodial –Combined movement of •20 to 30 degrees of inversion •5 to 15 degrees of eversion |
|
|
|
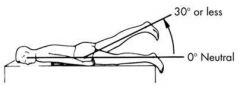
Metatarsophalangeal joints
|
–Classified as condyloid-type joints
–Great toe metatarsophalangeal (MP) joint flexes 45 degrees & extends 70 degrees –MP joints of the four lesser toes •40 degrees of flexion •40 degrees of extension •also abduct & adduct minimally |
|
|
|
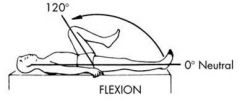
Movement of great toe interphalangeal (IP) joint
|
joint flexes from 0 degrees of full extension to 90 degrees of flexion
|
|
|
|
Proximal interphalangeal (PIP) joints movement?
|
in lesser toes flexes from 0 degrees of extension to 35 degrees of flexion
|
|
|
|
Distal interphalangeal (DIP) joints movement?
|
flexes 60 degrees & extend 30 degrees
|
|
|
|
Excessive _____ forces injures deltoid ligament (medially) and is ___ common
|
eversion
less |
|
|
|
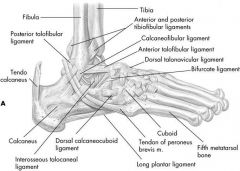
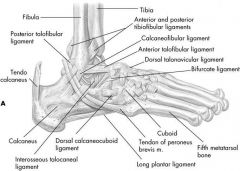
Most ____ ankle sprain results from excessive ____ that causes damage to lateral ligamentous structures, primarily _____ & _____
|
common
inversion anterior talofibularligament calcaneofibularligament |
|
|
|
Most common ankle sprain results from excessive inversion that causes damage to lateral ligamentousstructures, primarily anterior talofibularligament & calcaneofibularligament
|
|
|
|
|
Most common ankle sprain results from excessive inversion that causes damage to lateral ligamentousstructures, primarily anterior talofibularligament & calcaneofibularligament
|
|
|
|

|
Excessive eversion forces injures deltoid ligament (medially) -less common
|
|
|
|
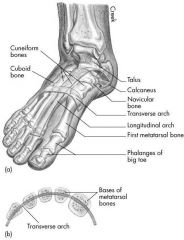
There are two _____ arches of the foot and one _____arch
|
|
longitudinal & transverse
–Medial arch -extends from calcaneus bone to talus, navicular, 3 cuneiforms, and proximal ends of 3 medial metatarsals –Lateral longitudinal arch -extends from calcaneus to cuboid and proximal ends of 4th& 5thmetatarsals –Long arches may be high, medium, or low |
|
|
Transverse arch location?
|

|
–extends across foot from 1stmetatarsal to the 5thmetatarsal
|
|
|
triceps surae includes
|
gastrocnemius & soleus
|
|
|
|
Plantar flexors
|
–Gastrocnemius
–Flexor digitorum longus –Flexor hallucis longus –Peroneus (fibularis) longus –Peroneus (fibularis) brevis –Plantaris –Soleus –Tibialis posterior |
|
|
|
Plantar flexors
|
|
–Gastrocnemius
–Flexor digitorum longus –Flexor hallucis longus –Peroneus (fibularis) longus –Peroneus (fibularis) brevis –Plantaris –Soleus –Tibialis posterior |
|
|
Ankle and foot joint evertors?
|
|
–Peroneus (fibularis) longus
–Peroneus (fibularis) brevis –Peroneus (fibularis) tertius –Extensor digitorum longus |
|
|
Ankle & footjoint Invertors
|
|
–Tibialisanterior
–Tibialisposterior –Flexor digitorum longus (flexor of lesser toes) –Flexor hallucis longus (flexor of great toe) |
|
|
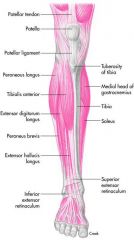
Ankle & footjoint muscles Anteriorcompartment
|
|
–Tibialisanterior
–Extensorhallucislongus –Extensordigitorumlongus –Peroneus(fibularis)tertius |
|
|
Ankle & footjoint muscles Lateral compartment
|
|
–Peroneus (fibularis) longus
–Peroneus (fibularis) brevis |
|
|
Ankle & foot joint muscles Deep posterior compartment
|
|
–Flexor digitorum longus
–Flexor hallucis longus –Tibialis posterior |
|
|
Ankle & foot joint muscles
Superficial posterior compartment |
|
–Gastrocnemius (medial head)
–Gastrocnemius (lateral head) –Soleus |
|
|
Ankle Dorsiflexion Agonists
|
–Tibialis anterior
–Extensor digitorum longus –Peroneus (fibularis) tertius •Extensor hallucis longus |
|
|
|
Ankle Plantar Flexion
•Agonists |
–Gastrocnemius
–Soleus •Flexor digitorum longus •Flexor hallucis longus •Peroneus (fibularis) longus •Peroneus (fibularis) brevis •Plantaris •Tibialis posterior |
|
|
|
Transverse Tarsal & Subtalar Inversion
•Agonists |
–Tibialis anterior
–Tibialis posterior •Flexor digitorum longus •Flexor hallucis longus |
|
|
|
Transverse Tarsal & Subtalar Eversion
•Agonists |
–Peroneus (fibularis) longus
–Peroneus (fibularis) brevis –Peroneus (fibularis) tertius –Extensor digitorum longus |
|
|
|
Toe Flexion
•Agonists |
–Flexor hallucis longus
–Flexor digitorum longus |
|
|
|
Toe Extension
•Agonists |
–Extensor hallucis longus
–Extensor digitorum longus |
|
|
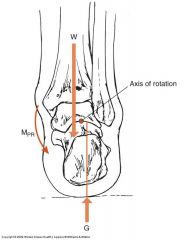
Talocrural joint - Axes of rotation and joint movements.
|
|
|
|
|
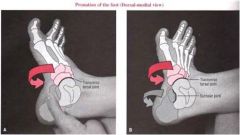
•Transverse tarsal joint - Axes of rotation and joint movements - pronation
|
|
|
|
|
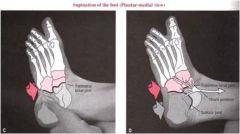
•Transverse tarsal joint - Axes of rotation and joint movements supination
|
|
|
|
|
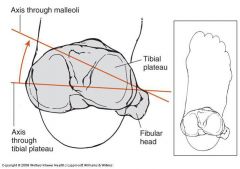
Axis of rotation through tibial plateu and malleoli
|
|
|
|
|
what are the associated movements during exaggerated pronation of the subtalar joint while weight bearing?
|
Hip (internal rotation, flexion and adduction)
Knee (Valgus strain) Subtalar joint (pronation and lowering of the logitiudinal arch) Transverse tarsal joint (inversion/ supination) |
|
|
|
kinetics of plantar flexor muscles during gait?
|
•Also supinate the subtalar or transverse tarsal joints.
•(except for peroneus longus and brevis). •Become active right after the dorsiflexor muscles relax. •Are active throughout most of the stance phase of gait (especially between foot-flat and toe-off). •Act eccentrically to decelerate the forward motion (dorsiflexion) of the leg (from foot-flat to about heel off). •Switch to a concentric activation in order to provide push off thrust (between heel-off and toe-off). |
|
|
|
What are the strongest plantar flexor muscles?
|
•The gastrocnemius and the
soleus muscles are the strongest plantar flexors (producing 80% of the total plantarflexion torque). |
|
|
|
kinetics of supinator muscles of the foot/ ankle during gait?
|
The tibialis posterior, flexor hallucis longus, and the flexor digitorum longus are the primary supinators.
•Tibialis posterior is the strongest supinator. •During stance phase, the tibialis posterior is active longer than the others, and it decelerates the pronating rearfoot and assist in controlling the lowering of the medial longitudinal arch. •Through eccentric action, the tibialis posterior also absorbs some of the impact of loading. |
|
|
|
The column consists of?
|
33 vertebrae, 24 of which are moveable
|
|
|
|
most mobile joint of the cervical region?
|
atlas and axis
|
|
|
|
Most highly loaded structure in the skeletal system?
|
Lumbar region
|
|
|
|
Strength and Forces at the Vertebral Joints
|
•Trunk extension strengths average 210 Nm.
•Trunk flexion strengths average 150 Nm. •Trunk lateral flexion averages 145 Nm. •Trunk rotation strengths average 90 Nm. •Intra-abdominal pressure, ligaments, and other structures also contribute to the net strength moments. |
|
|
|
Posture when sitting
|
–Unsupported sitting is more strenuous on spine.
–When sitting, lumbar lordosis is reduced, and the upper body center of gravity shifts forward. –Lumbar load is reduced in supported sitting, especially with lumbar support and a reclined |
|
|
|
posture when standing?
|
–S-shaped spine acts as an elastic rod support.
–Erector spinae helps keep spine erect. –When slouching, the ligaments and joint capsules maintain posture. |
|
|
|
•Atlantoaxial joint
|
–Atlas (C1) sits on axis (C2)
–Most cervical rotation occurs here –Trochoid or pivot-type joint –Most mobile joint of any two vertebrae |
|
|
|
•Atlantooccipital joint
|
–first joint
–formed by occipital condyles of skull sitting on articular fossa of the 1stvertebra –allows capital flexion & extension |
|
|
|
vertebral articulations, type and movement?
|
–Cumulative effect of combined movement from several vertebrae allows for substantial movements
•Minimal movement between any 2 vertebrae (except atlantoaxial joint) –Cumulative effect of combined movement from several vertebrae allows for substantial movements –Vertebral articulations classified as arthrodial –Gliding-type joints due to limited gliding movements –Gliding movement between superior & inferior articular processes of facets joints |
|
|
|
herniated or “slipped” disk
|
–nucleus protruding through annulus resulting from substantial weakening combined with compression
–protrusion puts pressure on spinal nerve root, causing radiating pain, tingling, numbness, and/or weakness in lower extremity |
|
|
|
Degrees of movement - CERVICAL region
|
–Flexes 45 degrees
–Extends 45 degrees –Laterally flexes 45 degrees –Rotate approximately 60 degrees |
|
|
|
Degrees of movement - LUMBAR region
(including trunk movement) |
–Flexes approximately 80 degrees
–Extends 20 to 30 degrees –Lumbar lateral flexion to 35 degrees –Rotation approximately 45 degrees |
|
|
|
•Muscles that move the head–Anterior
|
•Rectus capitis anterior
•Longus capitis |
|
|
|
•Muscles that move the head– Posterior
|
•Longissimus capitis
•Obliquus capitis superior •Obliquus capitis inferior •Rectus capitis posterior -major & minor •Trapezius, superior fibers •Splenius capitis •Semispinalis capitis |
|
|
|
Muscles that move the head–Lateral
|
•Rectus capitis lateralis
•Sternocleidomastoid |
|
|
|
•Muscles that move the head–Lateral
|
•Rectus capitis lateralis
•Sternocleidomastoid |
|
|
|
•Musclesofthevertebralcolumn–Superficial
|
•Erector spinae (sacrospinalis)
–Spinalis -cervicis, thoracis –Longissimus -capitis, cervicis, thoracis –Iliocostalis -cervicis, thoracis, lumborum •Splenius cervicis |
|
|
|
•Musclesofthevertebralcolumn
–Deep |
•Longus colli -superior oblique, inferior oblique, vertical
•Interspinales -entire spinal column •Intertransversales -entire spinal column •Multifidus -entire spinal column •Psoas minor •Rotatores -entire spinal column •Semispinalis -cervicis, thoracis |
|
|
|
•Musclesofthethorax
|
–Diaphragm
–Intercostalis-external,internal –Levatorcostarum –Subcostales –Scalenus-anterior,medius,posterior –Serratusposterior-superior,inferior –Transversusthoracis |
|
|
|
•Musclesoftheabdominalwall
|
–Rectus abdominis
–External oblique abdominal (obliquus externus abdominis) –Internal oblique abdominal (obliquus internus abdominis) –Transverse abdominis (transversus abdominis) –Quadratus lumborum |
|
|
|
Muscles that Move the Head
|
–3 anterior vertebral muscles –longus capitis, rectus capitis anterior & rectus capitis lateralis
•All are flexors of head & upper cervical spine •Rectus capitis lateralis –laterally flexes head –assists rectus capitis anterior in stabilizing atlantooccipital joint |
|
|
|
Muscles that Move the Head
|
|
•All originate on cervical vertebrae & insert on occipital bone of skull (capitis name)
–3 anterior vertebral muscles –longus capitis, rectus capitis anterior & rectus capitis lateralis •All are flexors of head & upper cervical spine •Rectus capitis lateralis –laterally flexes head –assists rectus capitis anterior in stabilizing atlantooccipital joint |
|
|
Posterior muscles- Muscles that Move the Head
|
•Rectus capitis posterior major & minor, obliquus capitis superior & inferior, and semispinalis capitis
•All are extensors of head except obliquus capitis inferior which rotates atlas •Obliquus capitis superior assists rectus capitis lateralis in lateral flexion of head •Rectus capitis posterior major rotates head to ipsilateral side •Semispinalis capitis rotates head to contralateral side •Upper trapezius extend head & rotate its to ipsilateral side |
|
|
|
Posterior muscles - Muscles that Move the Head
|

|
•Rectus capitis posterior major & minor, obliquus capitis superior & inferior, and semispinalis capitis
•All are extensors of head except obliquus capitis inferior which rotates atlas •Obliquus capitis superior assists rectus capitis lateralis in lateral flexion of head •Rectus capitis posterior major rotates head to ipsilateral side •Semispinalis capitis rotates head to contralateral side •Upper trapezius extend head & rotate its to ipsilateral side |
|
|
muscles that extend spine and assist in rotation & lateral flexion
|
Cervical area
–Longus colli muscles •located anteriorly •flex cervical & upper thoracic vertebrae •Posterior –Erector spinae group, transversospinalis group, interspinal-intertransverse group & splenius •All run vertically parallel to spinal column |
|
|
|
Posterior Muscles of the Thorax
|
•Scalene muscles elevate first 2 ribs to increase thoracic volume
•External intercostals further expand the chest •Levator costarum & serratus posterior –inspiration •Internal intercostals, transversus thoracis, & subcostales contract to force expiration |
|
|
|
Cervical Extension
•Agonists |
–Erector Spinae
|
|
|
|
Cervical Lateral Flexion
•Agonists |
–Sternocleidomastoid
–Erector Spinae |
|
|
|
Cervical Rotation
•Agonists |
–Sternocleidomastoid
|
|
|
|
Lumbar Flexion
•Agonists |
–Rectus abdominis
–External oblique abdominal –Internal oblique abdominal |
|
|
|
Lumbar Extension
•Agonists |
–Erector spinae
|
|
|
|
Lumbar Lateral Flexion
•Agonists |
–Erector spinae
–External oblique abdominal –Internal oblique abdominal |
|
|
|
Lumbar Rotation
•Agonists |
–Rectus abdominis
–External oblique abdominal –Internal oblique abdominal |
|
|
|
Where is the centre of pressure (CoP)?
|
•The CoP lies between the feet and just anterior to the ankle.
•When a person stands on a force platform the CoP can be determined by measuring the weight bearing of the feet and subsequently calculating a theoretical average force between the feet. |
|
|
|
•Knee joint
|
–largest joint in body
–very complex –primarily a hinge joint •Enlarged femoral condylesarticulate on enlarged tibial condyles •Medial & lateral tibial condyles (medial & lateral tibial plateaus) -receptacles for femoral condyles •Tibia –medial –bears most of weight |
|
|
|
•Fibula
|
-lateral
–serves as the attachment for knee joint structures –does not articulate with femur or patella –not part of knee joint |
|
|
|
•Patella
|
–sesamoid (floating) bone
–imbedded in quadriceps & patellar tendon –serves similar to a pulley in improving angle of pull, resulting in greater mechanical advantage in knee extension |
|
|
|
Gerdy’stubercle
|
Iliotibialtract of tensor fasciae lataeinserts on
|
|
|
|
“PesAnserine”
|
Sartorius, gracilis, & semitendinosusinsert just below the medial condyleon upper anteromedialtibialsurface
|
|
|
|
Collateral ligaments
|
The primary function of the collateral ligaments is to limit excessive motion in the frontal plane.
A secondary function of the collateral ligaments is to limit the extremes of knee extension In full knee extension (locked position), the MCL and posterior capsule provide resistance. Full extension elongates the collateral ligaments by 20% (compared to the flexion). A taut MCL is particular vulnerable to valgus stress. |
|
|
|
meniscus (medial and lateral) function?
|
–Thicker on outside border & taper down very thin to inside border
–Can slip about slightly, but held in place by various small ligaments –Medial meniscus -larger & more open Cappearance –Lateral meniscus -closed Cconfiguration |
|
|
|
•Anterior cruciate ligament (ACL) injuries
|
–one of most common serious injuries to knee
–mechanism often involves noncontact rotary forces associated with planting & cutting, hyperextension, or by violent quadriceps contraction which pulls tibia forward on femur |
|
|
|
•Posterior cruciate ligament (PCL) injuries
|
–not often injured
–mechanism of direct contact with an opponent or playing surface |
|
|
|
•Tibial (medial) collateral ligament (MCL)
|
–maintains medial stability by resisting valgus forces or preventing knee from being abducted
–injuries occur commonly, particularly in contact or collision sports –mechanism of teammate or opponent may fall against lateral aspect of knee or leg causing medial opening of knee joint & stress to medial ligamentous structures |
|
|
|
•Synovial cavity of the knee
|
–supplies knee with synovial fluid
–lies under patella and between surfaces of tibia & femur –"capsule of the knee” |
|
|
|
•Infrapatellar fat pad
|
–just posterior to patellar tendon
–an insertion point for synovial folds of tissue known as “plica” •an anatomical variant that may be irritated or inflamed with injuries or overuse of the knee |
|
|
|
•Bursae of the knee
|
–more than 10 bursae in & around knee
–some are connected to synovial cavity –they absorb shock or prevent friction |
|
|
|
Knee ROM?
|
•Extends to 180 degrees
(0 degrees of flexion) •Hyperextension of 10 degrees or > not uncommon •Flexion occurs to about 140 degrees •With knee flexed 30 degrees or > –internal rotation 30 degrees occurs –external rotation 45 degrees occurs |
|
|
|
•Knee “screws home”, how and why?
|
to fully extend due to the shape of medial femoral condyle
–As knee approaches full extension tibia must externally rotate approximately 10 degrees to achieve proper alignment of tibial & femoral condyles –In full extension •close congruency of articular surfaces •no appreciable rotation of knee –During initial flexion from full extension •knee “unlocks” by tibia rotating internally, to a degree, from its externally rotated position to achieve flexion |
|
|
|
internal rotation of the knee will not occur unless the knee if flexed to _____ to >20-30 degrees or
|
20-30 degrees or >
|
|
|
|
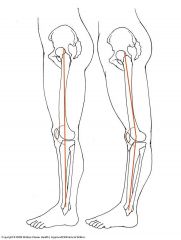
what is the Q angle?
|
–Central line of pull for entire quadriceps runs from ASIS to the center of patella
–Line of pull of patella tendon runs from center of patella to center of tibial tuberosity –Angle formed by the intersection of these two lines at the patella is the Q angle –Normally, angle will be 15 degrees or less for males & 20 degrees or less in females –Generally, females have higher angles due to a wider pelvis –Higher Q angles generally predispose people in varying degrees to a variety of potential knee problems including lateral patellar subluxation or dislocation, patellar compression syndrome, chondromalacia, and ligamentous injuries –For people with above normal Q angles, it is particularly important to maintain high levels of strength & endurance in vastus medialis so as to counteract lateral pull of vastus lateralis |
|
|
|
Does external rotation of Hip alter Knee joint alignment?
|

yes
|
|
|
|
what is Genu Recurvatum
|
|
|
|
|
Knee joint muscles location
•Posterior-primarilykneeflexion |
–Bicepsfemoris
–Semimembranosus –Semitendinosus •Sartorius •Gracilis •Popliteus •Gastrocnemius |
|
|
|
•Femoral nerves innervates the knee extensors (quadriceps)
|
–rectus femoris
–vastus medialis –vastus intermedius –vastus lateralis |
|
|
|
•Sciatic nerve innervation –tibial division and –common peroneal
|
–tibial division
•semitendinosus, semimembranosus, biceps femoris (long head) –common peroneal (fibular) division •biceps femoris (short head) |
|
|
|
•Quadriceps muscles
|
-vital in jumping
–functions as a decelerator •when decreasing speed to change direction •when coming down from a jump –eccentric contraction during decelerating actions –controls slowing of movements initiated in previous phases of the sports skill |
|
|
|
Muscle imbalance in the knee produces _____ Tilt
|
Patella
|
|
|
|
Knee Extension
•Agonists |
–Rectus Femoris
–Vastus Lateralis –Vastus Intermedius –Vastus Medialis |
|
|
|
Knee Flexion
•Agonists |
–Biceps Femoris (Long & Short Head)
–Semitendinosus –Semimembranosus |
|
|
|
Knee Internal Rotation
•Agonists |
–Semitendinosus
–Semimembranosus –Popliteus |
|
|
|
Knee External Rotation
•Agonists |
–Biceps Femoris
|
|
|
|
Knee Extension
•Agonists |
–Rectus Femoris
–Vastus Lateralis –Vastus Intermedius –Vastus Medialis |
|
|
|
Knee Flexion
•Agonists |
–Biceps Femoris (Long & Short Head)
–Semitendinosus –Semimembranosus |
|
|
|
Knee Internal Rotation
•Agonists |
–Semitendinosus
–Semimembranosus –Popliteus |
|
|
|
Knee External Rotation
•Agonists |
–Biceps Femoris
|
|
|
|
facet orientation of the ______spine.
|
|
|
|
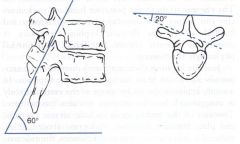
Facet Orientation in the T/Spine?
|
in the T/Spine –60 degrees to the Horizontal plane; 20 degrees to the Coronal plane.
|
|
|
|
Thoracic Spine: three regions?
|
•Upper (T1, T2 (T3) -similar to cervical spine.
•Mid (T3-T9)= ‘functional thoracic'. •Lower (T10-T12) –similar to lumbar spine. |
|
|
|
Kinematics of the Thoracic Spine: Kyphosis
|
20-55º Kyphosis
Average = 45º Kyphosis maintained in supine position and during trunk muscle contraction. |
|
|
|
Thoracic Spine ROM?
(Neumann p.286) |
–Flexion30-40º
–Extension20-25º –Axial rotation 30º –Lateral flexion 25º |
|
|
|
Flexion in the thoracic involves what structures?
|
concentric activity of the rectus abdominis and controlledby eccentric activity of the erector spinae, multifidi, etc.
•There is a stretching/ distraction of all the posterior elements. •Stabilised by passive (ligamentous) structures (supraspinous, interspinous, posterior longitudinal ligaments, and posterior annulus fibrosus) and muscular contractions. |
|
|
|
Extension in the thoracic involves which structures?
|
•an osseous stabilisation formed by approximation of the inferior articular process on the inferior vertebra, and approximation of the spinous processes.
•Further stabilisation is achieved through passive stretch of anterior annulus fibrosus, and anterior longitudinal ligament. •Eccentric contraction of rectus abdominis further controls the movement. |
|
|
|
Lateral flexion in the thoracic involves which structures?
|
•initiated by ipsilateral contraction of erector spinae and quadratus lumborum.
•both zygapophysial facet joint surfaces slide on each other. •On the ipsilateral side, the inferior articular process slide inferiorly, and on the contralateral side, the inferior articular process slide superiorly. •Controlled by contralateral eccentric contraction of erector spinae, quadratus lumborum, and the ‘segmental’ muscles (multifidii / rotatores). •Further controlled by passive ligamentous (capsular) structures (ligs. intertransversales, capsules). |
|
|
|
Rotation in the thoracic involves which structures?
|
•Almost a pure rotation/torsion of the IV disc, with little lateral translation.
•initiated by concentric activity of ipsilateral erector spinae, ipsilateral internal obliques and contralateral external obliques. •The ribcage is the strongest stabilising factor for all the thoracic movements, provide the strongest stabilising support (resistance to further movement). •The multifidus muscle probably acts more like a stabilising muscle bilaterally (creates compressive force across the joint). •Rotation is further controlled by the ligamentous structures (articular capsule, supraspinous, interspinous, and the collagen fibres of the annulus fibrosus running in that direction). |
|
|
|
T1,T2 function are similar to normal cervical spine function? T or F
|
True
|
|
|
|
About __ of sagittal plane _____ for each segment (occuring with _____).
|
5º
rotation flexion |
|
|
|
Upper Thoracic Spine _____& _____
Lateral flexion (__-__degº total segmental ROM). |
T1
T2 4-8º |
|
|
|
Lateral flexion is associated with ______ in ipsilateral _____rotation and contralateral ________ rotation of the upper ribs.
|
coupled motion
anterior posterior |
|
|
|
The ribs on the same side (side of LF) rotate _______, and those on the contralateral side rotate _____ –spinous rotates _____.
|
anterior
posterior TOWARD |
|
|
|
Upper Thoracic Spine (T1,T2) axial rotation ROM?
|
8-12º total segmentalROM
|
|
|
|
explain coupled motion in Upper Thoracic Spine (T1,T2).
|
The coupled motion that may occur is inconsistent within and between individuals, due to the influence of muscle activity.
|
|
|
|
Mid-thoracic Spine (___-___) is the ____mobile in __ rotation (__ total segmental ROM).
|
T3-T9
most axial 5º |
|
|
|
explain movement in the thoracic spine
|
•Promotes lateral translation of the facets accompanied by ipsilateral translation and tilt of the vertebral body (i.e. ipsilateral flexion) posterior rotation of the ipsilateral ribs, and anterior rotation of the contralateral ribs. I.e. Spinous rotates AWAY.
|
|
|
|
explain coupled motion in Mid-thoracic Spine (T3-T9)
|
coupled motion is limited by the thin IV disc and tension in the costal ligaments.
|
|
|
|
Rotation of the ribs occurs due to?
|
tension developed in the costal ligaments during axial rotation in the mid-thoracic spine.
|
|
|
|
Anterior sagittal rotation (and anterior translation) is limited by?
|
the vertical vertebral articular facet joints.
|
|
|
|
Sagittal rotation for each segment in Mid-thoracic Spine (T3-T9)?
|
is about 5º.
|
|
|
|
Lateral flexion in the Mid-thoracic Spine (T3-T9) is restricted by?
|
approximation of the ribcage.
|
|
|
|
Flexion in the Mid-thoracic Spine (T3-T9) is limited by?
|
tension in the posterior spinal ligaments and approximation of the ribs.
|
|
|
|
Extension in the Mid-thoracic Spine (T3-T9) is associated with _____ and limited by the bony contact of the ____ and the _______.
|
posterior translation
articular processes spinous processes |
|
|
|
Movement in the lower Thoracic Spine (T10-T12) is influenced by?
|
the variability of the posterior elements (i.e. facet tropism) and the anatomy of the lower two ribs.
|
|
|
|
The lower thoracics have increasing ____ plane rotation caudally (i.e. __º of total segmental ROM at T10-11, but __º on average between T8 and T12).
|
sagittal
20 5 |
|
|
|
The mobility in the ____ plane is similar to that of the upper and middle thoracic region (approx. ___º total ROM).
|
coronal
6 |
|
|
|
In lateral flexion, the segmental motions ____ caudally (from ___º at T9-10 to ___º at T11-12) –due to ___.
|
increase
6 12 the lower 2 ribs |
|
|
|
The ___thoracic segments have a more limited segmental axial rotation (___º) compared to the ____and ______thoracic regions.
|
lower
5-7 upper mid- |
|
|
|
Coupled thoracic motion
|
•There is a varying degree of coupled motion in the thoracic spine.
•These regional variations in movement coupling are probably due to the vertebral orientation within the kyphosis, the zygapophysial joint orientation, and the costal articulations. •The movement of the thoraxinto right rotation is associated with posterior rotation of the ipsilateral ribs. |
|
|
|
Explain the compressive load on the thoracic spine.
|
•The gravitational line falls anterior to the vertebral bodies, thereby increasing the axial load on the region.
•The compressive load on the thoracic spine increases caudally from 9% of body weight at T1 to 47% of body weight at T12. •This is counter met by a progressive increase in vertebral body size, end-plate cross-sectional area, and bone content. •About 76% of compressive load in the upper thoracic spine is transferred through the vertebral body/intervertebral (disc) complex. |
|
|
|
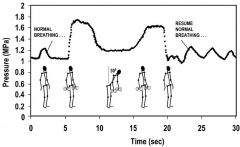
Explain intradiscal pressure in the thoracic spine.
|
|
•In upright standing position, the intradiscal pressure is about 1 MPa in the middle thoracic spine (T6-7, T7-8), but only 0.9 MPa at T9-10, T10-11.
•So, due to the increased end-plate cross-sectional area, the intradiscal pressure actually decreases caudally.•The intradiscal pressure varies greatly with different positions/manoeuvres. •Sitting upright does not alter the intradiscal pressure (from satnding upright), but lying on the side decreases the intradiscal pressure to about 0.3 MPa. Carrying weights (20 kg) increases the intradiscal pressures, but actually decreases when the person is 30º flexed (at the hips) -(opposite to the Lumbar Spine!) |
|
|
•Rib movement occurs around a _____axis, which extends from the costo-vertebral joint towards the rib tubercle.
•In the upper ribs, the axis is located at about __º to the coronal plane (___–shown right), whereas in the lower ribs the axis is oriented closer to the sagittal plane (__ –shown left). |
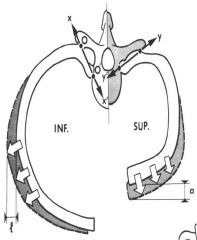
medio-lateral. 35. Y. X.
|
|
|
|
Movement of the upper ribs ____the sternum and ____ the A-P diameter of the ribcage (i.e. a ‘pump-handle’).
|
elevates
increases |
|
|
|
movement of the lower ribs has a greater influence on the ____dimensions of the ribcage (i.e. a ‘bucket-handle’).
|
lateral
|
|
|
|
Pelvic ______ increases the length of stride in running; in kicking it results in a greater distance or more speed to the kick
|
rotation
|
|
|
|
Teres ligament
|
attaches from deep in acetabulum to a depression in femoral head, slightly limits adduction
|
|
|
|
Ischiofemoral ligament
|
located posteriorly, extends from ischium to trochanteric fossa of femur, limits internal rotation
|
|
|
|
ROM hip flexion ?
|
0 to 130 degrees of flexion
|
|
|
|
What is the ROM of the hip (femoropelvic) in extension?
|
|
|
|
|
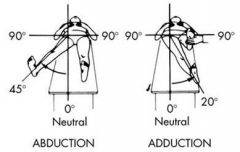
What is the ROM of Adduction and Abbduction of the femoropelvic joint?
|
–0 to 35 deg of abduction
–0 to 30 deg of adduction |
|
|
|
what is the ROM of adduction and abbduction of the hip?
|
|
|
|
|
what is the ROM of adduction and abbduction of the hip?
|
|
|
|
|
ROM of adduction and abbduction of the hip?
|
–0 to 35 degrees of abduction
–0 to 30 degrees of adduction |
|
|
|
ROM of internal and external rotation of the hip?
|
–0 to 45 degrees of internal rotation
–0 to 50 degrees of external rotation |
|
|
|
Motions accompanying pelvic Anterior rotation
|
Lumbar Spine Motion - Extension
Right Hip Motion - Flexion Left Hip Motion - Flexion |
|
|
|
Motions accompanying pelvic Posterior rotation
|
Lumbar Spine Motion - Flexion
Right Hip Motion -Extension Left Hip Motion - Extension |
|
|
|
Motions accompanying pelvic right lateral rotation
|
Lumbar Spine Motion -Right lateral flexion
Right Hip Motion-Adduction Left Hip Motion-Abduction |
|
|
|
Motions accompanying pelvic Left lateral rotation
|
Lumbar Spine Motion-Left lateral flexion
Right Hip Motion-Abduction Left Hip Motion-Adduction |
|
|
|
Motions accompanying pelvic-Right transverse rotation
|
Lumbar Spine Motion-Left transverse rotation
Right Hip Motion-Internal rotation Left Hip Motion-External rotation |
|
|
|
Motions accompanying pelvic- Left transverse rotation
|
Lumbar Spine Motion-Right transverse rotation
Right Hip Motion-External rotation Left Hip Motion-Internal rotation |
|
|
|
Anterior & posterior pelvic rotation plane of movement?
|
–sagittal or anteroposterior plane
|
|
|
|
•Right & left lateral pelvic rotation plane of movement?
|
–lateral or frontal plane
|
|
|
|
•Right transverse (clockwise) rotation & left transverse (counterclockwise) pelvic rotation plane of movement?
|
–horizontal or transverse plane of motion
|
|
|
|
Six two-joint muscles have one action at hip & another at knee, what are they
|
biceps femoris (long head)
sartorious gracilis semitendinosis semimembranosis rectus femoris |
|
|
|
•Hip joint & pelvic girdle muscles
–Anterior-primarily hip flexion |
•Iliopsoas
•Pectineus •Rectusfemoris •Sartorius |
|
|
|
•Hip joint & pelvic girdle muscles–Medial -primarily hip adduction
|
•Adductorbrevis
•Adductorlongus •Adductormagnus •Gracilis |
|
|
|
•Hip joint & pelvic girdle muscles–Posterior -primarily hip extension
|
•Gluteusmaximus
•Bicepsfemoris •Semitendinosus •Semimembranosus •Externalrotators |
|
|
|
•Hip joint & pelvic girdle muscles–Lateral -primarily hip abduction
|
•Gluteusmedius
•Gluteusminimus •Externalrotators •Tensorfasciaelatae |
|
|
|
•Pelvic muscles acting on hip joint
|
•Iliacus
•Psoas major •Psoas minor |
|
|
|
•Pelvic muscles acting on hip joint
–Gluteal region -extend & rotate hip |
•Gluteus maximus
•Gluteus medius •Gluteus minimi •Tensor fascia latae •Six deep external rotators -piriformis, obturator externus, obturator internus, gemellus superior, gemellus inferior, & quadratus femoris |
|
|
|
•Thigh -divided into 3 compartments by _____ _____.
|
intermuscular septa
|
|
|
|
–Anterior compartment –primarily knee extensors
|
•Rectus femoris
•Vastus medialis •Vastus intermedius •Vastus lateralis •Sartorius |
|
|
|
–Posterior compartment –hamstring group
|
•Biceps femoris
•Semitendinosus •Semimembranosus |
|
|
|
–Medial compartment –primarily adductors
|
•Adductor brevis
•Adductor longus •Adductor magnus •Pectineus •Gracilis |
|
|
|
Femoral n. innervation
|
•Iliopsoas
•Rectus femoris •Vastus medialis •Vastus intermedius •Vastus lateralis •Pectineus •Sartorius •Sensation to anterior & lateral thigh and medial leg & foot |
|
|
|
Obturator nerve innervation
|
•Adductor brevis
•Adductor longus •Adductor magnus •Gracilis •Obturator externus •Sensation to medial thigh |
|
|
|
Superior gluteal nerve innervation
|
•arises from L4, L5, & S1 to innervate gluteus medius, gluteus minimus, & tensor fasciae latae
|
|
|
|
Inferior gluteal nerve innervation
|
•arises from L5, S1, & S2 to supply gluteus maximus
|
|
|
|
Branches from sacral plexus- innervation
|
•piriformis (S1, S2), gemellus superior (L5, S1, S2), gemellus inferior & obturator internus (L4, L5, S1, S2), & quadratus femoris (L4, L5, S1)
|
|
|
|
–Sciatic nerve
•tibial division innervation |
–semitendinosus, semimembranosus, biceps femoris (long head) & adductor magnus
–sensation for posterolateral lower leg & plantar aspect of foot |
|
|
|
–Sciatic nerve
•common peroneal (fibular) division |
–sensation to anterolateral lower leg & dorsum of foot
|
|
|
|
Six Deep Lateral Rotator Muscles - Hip
|
Piriformis, Gemellus superior, Gemellus inferior, Obturator externus, Obturator internus, Quadratus femoris
|
|
|
|
Hip Flexion
•Agonists |
–Psoas
–Iliacus (Iliopsoas) –Rectus Femoris –Pectineus •Sartorius •Tensor Fasciae Latae |
|
|
|
Hip Extension
•Agonists |
–Gluteus Maximus
–Biceps Femoris (Long Head) –Semitendinosus –Semimembranosus |
|
|
|
Hip Abduction
•Agonists |
–Gluteus Medius
•Tensor Fasciae Latae •Gluteus Maximus •Gluteus Minimus |
|
|
|
Hip Adduction
•Agonists |
–Adductor Brevis
–Adductor Longus –Adductor Magnus –Gracilis |
|
|
|
Hip Internal Rotation
•Agonists |
–Gluteus Minimus
•Gluteus Medius •Tensor Fasciae Latae |
|
|
|
Hip External Rotation
•Agonists |
–Gluteus Maximus
–Six Deep External Rotators |
|
|
|
Gait cycle:
|
From first heel contact to second heel contact with the same foot.
|
|
|
|
Stride length
|
The distance between two successive heel contacts of the same foot.
|
|
|
|
Step length:
|
The distance between two successive heel contacts of the two different feet.
|
|
|
|
Step width:
|
The lateral distance between the heel centres of two consecutive foot contacts (7-9 cm)
|
|
|
|
Foot angle:
|
The degree of “toe out” = the angle between the line of progression of the body and the long axis of the foot (7 degrees).
|
|
|
|
Cadence =
|
step rate: The number of steps per minute
|
|
|
|
Gait speed:
|
1.37 m/s (4.9 km/h)
|
|
|
|
Step length:
|
72 cm
|
|
|
|
Stance phase:___ of gait cycle
From ____ contact to ____ |
60%
heel toe off |
|
|
|
Swing phase:____ of gait cycle
From ___to heel contact |
40%
toe off heel |
|
|
|
Double-limb support:At ____ & ____ of gait cycle.
Decreases with increasing speed |
0-10%
50-60% |
|
|
|
•The subtalar joint pronates /everts ______ of gait cycle (adding flexibility to the foot).
|
30-55%
|
|
|
|
•Late during the stance, the arch rises because of _______of _____joint giving the foot rigidity.
|
supination
subtalar |
|
|
|
•Right after heel contact, the foot _______and _____.
|
plantar flexes
pronates |
|
|
|
•Pronation is controlled by two mechanisms: they are?
|
1) the calcaneus tips into eversion (due to the ground) reaction force passing lateral to the A-P axis of rotation).
•This also pushes the head of talus medially in the horisontal plane and inferiorly in the sagittal plane. •This motion abducts and dorsiflexes the subtalar joint (which is consistent with the definition of pronation). 2) The second mechanism is the internal rotation of tibia and fibula during early stance phase |
|
|
|
•At _____ the pronated (everted) subtalar joint moves into supination
|
35%
|
|
|
|
•By late stance phase, the fully _______subtalar joint and elevated and tensed ______ _____ arch converts the midfoot into a more rigid lever.
|
supinated
medial longitudinal |
|
|
|
the “windlass effect” is?
|
•During the later part of the stance phase, the midfoot and forefoot must be relatively stable and rigid in order for the foot to push off.
•The whole foot is stabilised by extrinsic and intrinsic muscles as well as ligaments and the osseous structure of the medial longitudinal arch. |
|
|
|
cyclic gait phases and events:
|
.Initial Contact = Heel Strike (HS)
.Loading response = HS ¨ foot flat (FF) .Midstance = FF ¨ midstance .Terminal stance = Midstance ¨ heel off .Pre-swing = Heel off ¨ toe off .Initial swing = Toe off ¨ early accel. .Midswing = Acceleration ¨ midswing .Terminal swing = Midswing ¨ deceleration |
|
|
|
Sagittal Plane Kinematics:
Initial Contact (Heel Strike): |
•HIP: 25°flexion
•KNEE: 0°-5 °flexion •ANKLE: 0°(90 °) •Hip stabilised by extensor activity of hamstrings and gluteals. •Knee stabilised by contraction of quads and hamstrings. •Ankle dorsiflexors are positioning foot for initial contact. |
|
|
|
Sagittal Plane Kinematics:
Loading Response Phase (Heel Strike to Foot Flat) |
.HIP: 25‹flexion
.KNEE: 0‹¨ 15‹flexion (Lowers CM) .ANKLE: 0‹¨ 10‹plantar flexion .Hip abductors stabilise pelvic drop in frontal plane. .Hip extensors counteract trunk and hip flexion. .Quads control knee flexion providing shock absorption. .Ankle dorsiflexors decelerate foot drop. |
|
|
|
Sagittal Plane Kinematics:
Midstance Phase: (Foot Flat to midstance event) |
.HIP: 25‹flexion ¨ 0‹
.KNEE: 15‹flexion ¨ 0‹flexion .ANKLE: 10‹plantar flexion ¨ 5‹dorsi flexion .Hip abductors continue to minimize pelvic drop in the frontal plane. .Quads resist knee flexion until COG passes over base of support, then quads are silent. .Soleus and gastroc eccentrically control forward tibial progression. |
|
|
|
Sagittal Plane Kinematics:
Terminal Stance Phase: (Midstance event to HO) |
.HIP: 0‹flexion ¨ 20‹extension
.KNEE: 0‹ .ANKLE: 5‹¨ 10‹dorsiflexion .Brief burst from hip flexors resisting hyperextension of the hip. .Tensor fascia latae active throughout stance to resist pelvic drop. .Minimal to no quad or hamstring activity .Ankle plantar flexors contribute to heel rise through passive tension. |
|
|
|
Sagittal Plane Kinematics:
Pre-swing Phase: (Heel Off to Toe Off) |
.HIP: 20‹extension ¨ 0‹
.KNEE: 0‹¨ 40‹flexion .ANKLE: 10‹dorsiflexion ¨ 20‹plantar flexion .Flexion of the femur may be facilitated by adductor longus and rectus femoris. .Adductors stabilize pelvis during weight shift to other foot. .Rectus femoris may restrain rapid passive knee flexion, otherwise quads silent. .Passive tension in ankle plantar .flexors facilitates knee flexion and then decreases to zero in preparation for toe off. |
|
|
|
Sagittal Plane Kinematics:
Pre-swing Phase: (Heel Off to Toe Off) |
.HIP: 20‹extension ¨ 0‹
.KNEE: 0‹¨ 40‹flexion .ANKLE: 10‹dorsiflexion ¨ 20‹plantar flexion .Flexion of the femur may be facilitated by adductor longus and rectus femoris. .Adductors stabilize pelvis during weight shift to other foot. .Rectus femoris may restrain rapid passive knee flexion, otherwise quads silent. .Passive tension in ankle plantar .flexors facilitates knee flexion and then decreases to zero in preparation for toe off. |
|
|
|
Sagittal Plane Kinematics:
Initial Swing: |
•HIP: 15 °
•KNEE: 60° •ANKLE: 10°plantar flexion •Hip flexors flex hip. •Adductor longus brings leg toward midline. •Ankle pre-tibials initiate dorsiflexion to clear toes. |
|
|
|
Sagittal Plane Kinematics:
Mid-Swing: |
•HIP: 25 °
•KNEE: 25° •ANKLE: 0° •Hip flexors and momentum flex hip. •Hamstrings begin to decelerate knee extension. •Knee extension created by tibial •forward momentum. •Ankle pre-tibials concentrically contract to clear foot. |
|
|
|
Sagittal Plane Kinematics:
Terminal Swing: (Mid-swing->deceleration) |
•HIP: 25 °
•KNEE: 0° •ANKLE: 0°plantar flexion •Hamstrings continue to decelerate forward swing of leg. •Quadriceps may contract to extend knee in preparation for initial contact. •Ankle pre-tibials contract to prepare foot for initial contact. |
|
|
|
The path of the Center of Pressure (CoP) under the foot
|
|
•At heel contact the CoP is located just lateral to the midpoint.
•It then moves progressively to the lateral midfoot region at midstance and to the medial forefoot region during heel off to toe off. •Ends at the base of the Hallux during toe off. |
|
|
Determinants of Gait
|
Pelvic Rotation –transverse plane
Lateral Pelvic Tilt –frontal plane Knee Flexion –during stance Ankle PF -at Toe Off Ankle DF –at Foot strike Gait Width –frontal plane |
|
|
|
the foot at Ground Contact
|
Contact Made on the Lateral Border of the Heel
Foot is Supinated Foot is Rigid |
|
|
|
the foot at early Stance to MidStance
|
Foot is PronatedFoot is Mobile (flexible)Enhances Balance
|
|
|
|
the foot at Late Stance to Toe-Off
|
Foot is Supinated
Foot is Rigid Enhances Propulsion |
|
|
|
Pronation/Supination excess or limitation can lead to?
|
Too Little
–Loss of force dissipation -Loss of Mobility –BalanceStress Injury Too Much Relationship to Tibial Rotation Associated Patellar Tracking Issues Soft-Tissue Stress |
|
|
|
Ground Reaction Forces in running Influenced BY?
|
–Velocity
–Vertical Displacement –Shoes –Surface |
|
|
|
Ground Reaction Forces in Running influence?
|
–Foot Pressures
–Joint Forces –Joint Moments –Impact Shock |
|
|
|
What Factors Influence Speed ???
|
Stride LengthAnthropometric FactorsStrengthFlexibilityNeuromuscular Factors
Stride RateNeuromuscular FactorsTechnique |
|
|
|
Kinematics of the SI joints- inc ROM
|
•Relatively small rotational and translational movements.
•0.2-2º of rotation and •1-2mm of translation. •Primarily in the sagittal plane. •Nutation and counter-nutation. •Combination of compression force on the articular surfaces and actual slide movements between the surfaces. |
|
|
|
Nutation
|
•Nutation = Nodding
•Sacral base = Anterior-inferior •Sacral apex = Posterior-superior •Flexion of the sacrum on the ilium |
|
|
|
Counter-nutation
|
•The reverse motion
•Sacral base = Posterior-superior •Sacral apex = Anterior-(inferior) •Extension of the sacrum on the ilium |
|
|
|
SI motion in gait cycle?
|
•During a gait cycle each of the SI joints goes through two full cycles of alternating flexion and extension.
|
|
|
|
As one innominate flexes (PSIS moves posteriorly-inferiorly), the ipsilateral sacral base moves?
|
anteriorly and inferiorly.
|
|
|
|
as the other innominate extends (moves anteriorly superiorly), the sacral base on that side moves
|
posteriorly-superiorly.
|
|
|
|
during a continuous motion the sacrum performs what movement?
|
an oblique and horisontal figure-of-eight, rocking movement.
|
|
|
|
At R heel contact during gait
the R sacroiliac flexion and the R side of the pubic symphysis moves in which direction? |
superiorly
|
|
|
|
The Intervertebral Disc
|
•10-12 mm in height (5 cm in total).
•10-20 concentric, circumferential lamellae. •More type II fibres centrally. •More type I collagen fibers towards the periphery of the anulus. •Fibres in each lamella are parallel arranged and run obliquely in a 65º angle to the sagittal plane. •Run opposite directions from each other. |
|
|
|
the endplates are the ______components of the IV disc during axial compression
|
weakest
|
|
|
|
The facet shape may be ____(upper lumbar facets) or ____ (lower lumbar facets).
|
flat C-or J-curved
|
|
|
|
The shape and orientation govern the role of facet joints in preventing
|
forward displacement and rotatory dislocation of the motion segment.
|
|
|
|
The extent of forward displacement depends on the extent to which the superior articular facets face ______.
|
backwards
|
|
|
|
The extent to which the joint can resist rotation is related to the extent to which its superior articular facets face ______.
|
medially
|
|
|
|
Combination of A-P and M-L orientation of the facets creates a maximisation of resistance in _____
|
both directions.
|
|
|
|
A C-shaped articular facet provides a greater resistance in ___displacement as opposed to a J-shaped facets. (Lumbar)
|
forward
|
|
|
|
Kinematics of the Lumbar Spine: actions
|
•Axial compression
•Axial distraction •Flexion •Extension •Axial rotation •Lateral flexion •Rotation in flexio |
|
|
|
axial compression with slight extension (or with some IV disc degeneration) the load is also transmitted via the ______.
|
facet joints
|
|
|
|
Flexion of the lumbar spine involves both anterior sagittal ___ and anterior _____.
|
rotation
translation |
|
|
|
The zygapophysial joint capsules stretch about _____ during flexion.
|
5-7 mm
|
|
|
|
In lumbar flexion the vertebral bodies undergo posterior sagittal _____(extension) and a small posterior translation
|
rotation
translation |
|
|
|
in lateral flexion (lumbar) theoretically, both facet joints will slide (in ____directions) and cause ____ strain on both sides.
|
opposite
capsule |
|
|
|
The ROM (lumbar) increases when the lumbar spine is in a slightly flexed, seated position.
|
increases
|
|
|
|
Coupled Lumbar motion
|
•Combination of 8-13º of anterior sagittal rotation and 1-3 mm of forward translation, and these movements are consistently accompanied by axial and coronal rotations of about 1º.
•Some vertical and lateral translations also occur but are of small amplitude. •Conversely, extension involves posterior sagittal rotation and posterior translation, with some axial and coronal rotation, but little vertical and lateral translation. •Axial rotation and lateral flexion are coupled with one another and with sagittal rotation. |
|
|
|
What is the Instantaneous Axis of Rotation
|
The exact location of the IAR is a function of the amount of sagittal rotation and the amount of simultaneous sagittal translation that occurs during the phase of motion defined by the starting and end positions.
|
|
|
|
what is the location of the Instantaneous Axis of Rotation (IAR)
|
•In health individuals, the IAR lies close to the upper endplate and slightly posterior.
•If more anterior translation of the upper vertebra occurred then the IAR would shift anteriorly/inferiorly (and posteriorly/inferiorly if more posterior translation occurred). •With increased rotation the IAR moves more superiorly (and inferiorly if less rotation occurred). |
|
|
|
•Concentric contractions
|
–shortening contraction of muscles against gravity or resistance
|
|
|
|
•Eccentric contraction
|
–muscle lengthens under tension to control the joints moving with gravity or resistance
|
|
|
|
•Quadriceps contracts _______when the body slowly lowers in a weight bearing movement through lower extremity action
|
eccentrically
|
|
|
|
Muscular Actions
•Flexion of the thigh |
–Iliopsoas (also flexes trunk)
–Rectus femoris (also extends knee) –Sartorius –Pectineus –Tensor fascia latae |
|
|
|
Muscular Actions •Extension of the thigh
|
–Hamstrings (also flexes knee)
–Gluteus maximus |
|
|
|
Muscular Actions•Abduction of the thigh
|
–Gluteus medius
–Gluteus minimus –Tensor fascia latae –Piriformis |
|
|
|
Muscular Actions•Adduction of the thigh
|
–Gracilis
–Adductors longus, brevis, and magnus –Pectineus |
|
|
|
•Standing on two limbs—hip load is approximately ___ body weight (BW)
|
30%
|
|
|
|
•Standing on one limb—hip load is ____×BW
|
2.5–3.0
|
|
|
|
•Stair climbing—hip load is __BW
|
3×
|
|
|
|
•Walking—hip load is 4–7×BW
•Running—hip load is up to 10×BW •Hip can withstand 12–15×BW |
4–7x
10× 12–15× |
|
|
|
•More than ____ of hip injuries occur in the soft tissue.
|
60%
|
|
|
|
The Knee Joint
|
•Knee joint is a double condyloid joint.
•It has 2 degrees of freedom. •Flexion-extension •When flexing, there is a small but significant amount of rotation. |
|
|
|
Muscular Actions
•Extension of the Knee |
–Quadriceps femoris
•Rectus femoris •Vastus intermedius •Vastus lateralis •Vastus medialis |
|
|
|
Muscular Actions
•Flexion of the Knee |
–Hamstrings
•Biceps femoris •Semimembranosus •Semitendinosus |
|
|
|
Knee _______ stronger than _____ throughout range of motion
|
extensorsf
lexors |
|
|
|
•The foot and ankle consist of:
|
–26 irregular-shaped bones
–30 synovial joints –30 muscles –>100 ligaments |
|
|
|
•Most motion of the foot occurs at 3 joints:
|
–Talocrural
–Subtalar –Midtarsal |
|
|
|
talocrural joint
|
•The proximal joint of the foot is the talocrural joint (ankle joint).
•It is designed for stability rather than mobility. •This consists of articulations between the tibia and talus (tibiotalar joint) and tibia and fibula (tibiofibular joint). |
|
|
|
SubtalarJoint
|
•More distal than the talocrural joint
•Articulation between the talus and calcaneus •Talus and calcaneus are the largest weight-bearing bones in the foot. |
|
|
|
MidtarsalJoint
|
•Consists of two joints (calcaneocuboid and talonavicular)
•The alignment of the axes of these joints affects the mobility of the midfoot. |
|
|
|
•Sample forces on the ankle and foot
|
–Ground forces during walking: 0.8–1.1×BW at heel strike, 0.8×BW during midstance, 1.3×BW at toe-off
–Compression at the ankle joint during walking: 3×BW at heel strike, 5×BW at toe-off –During running: ankle forces of 9.0–13.3×BW and Achilles tendon forces of 5.3–10×BW |
|
|
|
There are two branches of kinetics;
|
STATICS and DYNAMICS
|
|
|
|
Kinematics
|
Describes the motion of a body without reference to the forces causing it. Examines how, when, and where a body moves.
|
|
|
|
kinematic motion movement may be LINEAR, CURVILINEAR
|
LINEAR,
CURVILINEAR angular parabolic |
|
|
|
DYNAMICS
|
the changes in motion brought on by unbalanced forces.
|
|
|
|
Lever Functions
|
•Magnify a force
•Increase speed and range of-motion (ROM) •Balance torques •Change direction of force |
|
|
|
First class lever
|
-FAR
-When axis close to force, produces speed and ROM, when close to resistance, produces power -About 25% of the muscles in your body operate as first class levers |
|
|
|
Second Class
|
•ARF
•Very few occurrences in the body •Gain resultant force (you can lift more), lose distance Force |
|
|
|
Third Class
|
•RFA
•As much as 85% of the muscles in the body function as third class levers •Usually produce speed at the expense of force •Greater lever length = greater speed (ex.) |
|
|
|
Laws of Motion
|
•Inertia
•Acceleration •Reaction •“A body in motion tends to stay in motion at the same speed in a straight line unless acted upon by a force; •A body at rest tends to remain at rest unless acted upon by a force” •English translation: unbalanced forces cause motion; Balanced forces don’t change anything |
|
|
|
Factors Influencing Balance
|
1.Location of the center of gravity in relation to the base of support
2.Size of the base of support 3.Mass of the person 4.Height of the center of gravity 5.Traction/friction 6.Sensory perceptions |
|
|
|
•Sternoclavicular (SC)
–(multiaxial) arthrodial classification –Movements |
•anteriorly 15 degrees with protraction
•posteriorly 15 degrees with retraction •superiorly 45 degrees with elevation •inferiorly 5 degrees with depression |
|
|
|
•Sternoclavicular (SC)
–Ligamentous support |
•anteriorly by the anterior SC ligament
•posteriorly by the posterior SC ligament •costoclavicular & interclavicular ligaments provide stability against superior displacement |
|
|
|
•Acromioclavicular (AC) joint
|
–arthrodial classification
–20-to 30-degree total gliding & rotational motion accompanying other shoulder girdle & shoulder joint motions –supported by •Coracoclavicular ligaments •Superior acromioclavicular ligament •Inferior acromioclavicular ligament –often injured |
|
|
|
Joints
•Scapulothoracic |
–not a true synovial joint
–does not have regular synovial features –movement depends on SC & AC joints which allows the scapula to move •25-degrees abduction-adduction •60-degrees upward-downward rotation •55-degrees elevation-depression –supported dynamically by its muscles –no ligamentous support |
|
|
|
Without the accompanying scapula movement humerus can only be raised into approximately 90 degrees of total shoulder abduction & flexion
|
90
|
|
|
|
5 muscles primarily involved in shoulder girdle movements
|
–Trapezius -upper, middle, lower
–Rhomboid -deep –Levator scapula –Serratus anterior –Pectoralis minor -deep |
|
|
|
Scapula Abduction
|
•Scapula move laterally away from spinous processes without rotation
•EX. Push-up & bench press •Agonists –Pectoralisminor –Serratusanterior |
|
|
|
Scapula Adduction
|
•Return from abduction
•Occurs with retractions •Agonists –Middle Trapezius –Rhomboids |
|
|
|
Scapula Upward Rotation
|
•Lateral & upward movement
•Agonists –Middle Trapezius –Lower Trapezius –Serratus anterior |
|
|
|
Scapula Downward Rotation
|
•Downward & Medial Movement
•Glenoid Fossa is rotated downward when downward movement of shoulder joint occurs •EX. Lat Pulls -pulling wt. down •Agonists –Pectoralis Minor –Rhomboid |
|
|
|
Scapula Elevation
|
•Lifting scapula without rotation in anatomic position
•Shoulder Shrug •Agonists –LevatorScapula –UpperTrapezius –Rhomboid |
|
|
|
Scapula Depression
|
•EX. Dip
•Agonists –Lower Trapezius –Pectoralis Minor |
|
|
|
5 muscles primarily involved in shoulder girdle movements
|
–Trapezius -upper, middle, lower
–Rhomboid -deep –Levator scapula –Serratus anterior –Pectoralis minor -deep |
|
|
|
Scapula Abduction
|
•Scapula move laterally away from spinous processes without rotation
•EX. Push-up & bench press •Agonists –Pectoralisminor –Serratusanterior |
|
|
|
Scapula Adduction
|
•Return from abduction
•Occurs with retractions •Agonists –Middle Trapezius –Rhomboids |
|
|
|
Scapula Upward Rotation
|
•Lateral & upward movement
•Agonists –Middle Trapezius –Lower Trapezius –Serratus anterior |
|
|
|
Scapula Downward Rotation
|
•Downward & Medial Movement
•Glenoid Fossa is rotated downward when downward movement of shoulder joint occurs •EX. Lat Pulls -pulling wt. down •Agonists –Pectoralis Minor –Rhomboid |
|
|
|
Which scapula movement usually occur with movement of humerus?
|
–Humeral flexion & abduction require scapula elevation, rotation upward, & abduction
–Humeral adduction & extension results in scapula depression, rotation downward, & adduction –Scapula abduction occurs with humeral internal rotation & horizontal adduction –Scapula adduction occurs with humeral external rotation & horizontal abduction |
|
|
|
Glenohumeral Joint type?
|
•multiaxial ball-&-socket
•enarthrodial |
|
|
|
Glenohumeral Joint ROM?
|
–90 to 95 degrees abduction
–0 degrees adduction, 75 degrees anterior to trunk –40 to 60 degrees of extension –90 to 100 degrees of flexion –70 to 90 degrees of internal & external rotation –45 degrees of horizontal abduction –135 degrees of horizontal adduction |
|
|
|
•Glenohumeral internal rotation deficit (GIRD)
|
–difference in internal rotation range of motion between an individual’s throwing & nonthrowing shoulders
–overhead athletes with a GIRD of greater than 20% had a higher risk of injury –stretching exercises recommended to regain internal rotation •improve performance •reduce likelihood of injury |
|
|
|
Pairing of shoulder girdle & shoulder joint movements
|
•Glenohumeral joint is paired with shoulder girdle to accomplish total shoulder range of motion
–Ex. 170 to 180 degrees of total abduction includes •approximately 60 degrees of scapula upward rotation •25 degrees of scapula elevation •95 degrees of glenohumeral abduction •Scapulohumeral rhythm –Not necessarily sequential actions, but synergistic relationship –Generally accepted ratio is 2 to 1 or for every 2 degrees of glenohumeral motion, there is 1 degree of scapula motion –May vary within and between individuals |
|
|
|
•Intrinsic glenohumeral muscles
|
–Originate on scapula & clavicle
–Deltoid, Coracobrachialis, Teres major –Rotator cuff group •subscapularis, supraspinatus, infraspinatus, & teres minor |
|
|
|
•Extrinsic glenohumeral muscles
|
–latissimus dorsi & pectoralis major
|
|
|
|
Muscles
•Anterior |
–Pectoralismajor
–Coracobrachialis –Subscapularis |
|
|
|
Muscles
•Superior |
–Deltoid
–Supraspinatus |
|
|
|
Muscles• Posterior
|
– Latissimus dorsi
– Teres major – Infraspinatus – Teres minor |
|
|
|
Lateral pectoral nerve arising from
|
C5, C6, & C7
–Pectoralis major (clavicular head) |
|
|
|
•Medial pectoral nerve arising from
|
C8 & T1
–Pectoralis major (sternal head) |
|
|
|
•Thoracodorsal nerve arising from
|
C6, C7, & C8
–Latissimus dorsi |
|
|
|
•Axillary nerve branching from
|
C5 & C6
–Deltoid –Teres minor –Sensation to lateral patch of skin over deltoid region of arm |
|
|
|
•Upper subscapular nerves arising from
|
C5 & C6
–Subscapularis |
|
|
|
•Lower subscapular nerve arising from
|
C5 & C6
–Subscapularis –Teres major |
|
|
|
•Suprascapula nerve originating from C5 & C6
|
–Supraspinatus
–Infraspinatus |
|
|
|
•Musculotaneous nerve branching from
|
C5, C6, & C7
–Coracobrachialis –Sensation to radial aspect of forearm |
|
|
|
Glenohumeral Flexion
•Agonists |
–Anterior Deltoid
–Upper Pectoralis Major |
|
|
|
Glenohumeral Extension
•Agonists |
–Teres Major
–Latissimus Dorsi –Lower Pectoralis Major |
|
|
|
Glenohumeral Abduction
•Agonists |
–Deltoid
–Supraspinatus –Upper Pectoralis Major |
|
|
|
Glenohumeral Adduction
|
•Agonists
–Latissimus Dorsi –Teres Major –Lower Pectoralis Major •EX. Lat. Pull -pull down weights |
|
|
|
Glenohumeral Internal Rotation
•Agonists |
–Latissimus Dorsi
–Teres Major –Subscapularis –Pectoralis Major •All attach anteromedially on humerus |
|
|
|
Glenohumeral External Rotation
•Agonists |
–Infraspinatus
–Teres Minor •Both attach posteriorly on greater tubercle |
|
|
|
Glenohumeral Horizontal Abduction
•Agonists |
–Posterior Deltoid
–Middle Deltoid –Infraspinatus –Teres Minor |
|
|
|
Glenohumeral Horizontal Adduction
•Agonists |
–Anterior Deltoid
–Pectoralis Major –Coracobrachialis |
|
|
|
Glenohumeral Diagonal Abduction
•Agonists |
–Posterior Deltoid
–Infraspinatus –Teres Minor –Triceps Brachii (Long Head) |
|
|
|
Glenohumeral Diagonal Adduction
•Agonists -both low & high |
–Anterior Deltoid
–Coracobrachialis –Biceps Brachii (short head) –Pectoralis Major -Upper & Lower |
|
|
|
Shoulder complex Four joints?
|
Four joints
1. The scapulothoracic “joint” 2. The sternoclavicular joint 3. The acromioclavicular joint 4. The glenohumeral joint |
|
|
|
Movements of the SC joint
|
•Elevation (45º)
•Depression (10º) •Protraction (15-30º) •Retraction (15-30º) •Axial rotation (40-50º) |
|
|
|
Stabilizing tissues of the AC joint:
|
-Superior and inferior AC joint capsular ligaments
-Deltoid and upper trapezius -Coracoclavicular ligament -Articular disc |
|
|
|
Movements of the AC joint:
|
Sagittal plane rotation adjustments (10-30º)
|
|
|
|
Movements of the scapulothoracic joint
|
-Elevation (superior slide)
-Depression (inferior slide) -Protraction (anterior-lateral slide) -Retraction (medial slide) -Upward rotation (inferior angle rotates supero-laterally) -Downward rotation (inferior angle rotates infero-medially) |
|
|
|
Stabilizing tissues of the GH joint:
|
•Rotator cuff muscles
•GH joint capsular ligaments •Coracohumeral ligament •Long head of biceps brachii •Glenoid labrum |
|
|
|
Movements of the GH joint
|
-Abduction and adduction (180º)
frontal vs. scapular plane (at 20 to 35º to the frontal plane) -Flexion (120º) and extension (45-55º) -Internal and external rotation (usually associated with pro-and retraction of the scapula); (70º and 85º respectively) |
|
|
|
Elevators of the scapulothoracic joint
|
-Upper trapezius (through postural support by maintaining shoulder in position)
-Levator scapulae-Rhomboids |
|
|
|
Depressors of the scapulothoracic joint
|
-Lower trapezius
-Latissimus dorsi -Pectoralis minor -Subclavius(by depressionof the clavicle) |
|
|
|
Protractors of the scapulothoracic joint
|
-Serratus anterior
|
|
|
|
Retractors of the scapulothoracic joint
|
-Middle trapezius
-Rhomboids -Lower Trapezius and Rhomboids also haveRotary functions. |
|
|
|
Abductors of the GH joint
|
-Anterior and middle deltoid
-Supraspinatus -Coracobrachialis (arm elevation through flexion eg. Abduction in the scapular plane) -Biceps (long head) (as for Coracobrachialis) |
|
|
|
Upward rotation of the scapulothoracic joint
|
Combination of muscles:-Deltoid (as whole)
-Serratus anterior-Trapezius (all parts) |
|
|
|
Upward rotation of the scapulothoracic joint
|
The lower fibers of serratus and upper and lower fibers of trapezius form a force couple that upwardly rotates the scapula.
The serratus anterior is the most effective upward rotator. The serratus anterior muscle has gradual increase in amplitude throughout the entire ROM of abduction. |
|
|
|
Upward rotation of the scapulothoracic joint
|
The supraspinatus is the primary initiatorof early abduction in association with upper trapezius which is especially active during this initiation, and then continues a gradual increase in activity (throughout abduction).
The upper trapezius elevates the clavicle during early phase while the lower trapezius is more actively performing scapular rotation during the late phase. |
|
|
|
A weakserratus anterior muscle leads to:
|
-Retraction of scapula (scapular winging).
-Shoulder impingement (due to limited upward rotation of the scapula causing reduced space between subacromial space. |
|
|
|
A paralysisof serratus anterior
|
(damage to long thoracic nerve):-Significant disruption in normal shoulder motion as the person cannot elevate the arm above 90º of abduction.
|
|
|
|
Internal rotation of the GH joint
|
-Subscapularis
-Pectoralis major -Latissimus dorsi -Teres major -and Anterior deltoid Produce 1.75 times greater isometric torque than the external rotators. |
|
|
|
External rotation of the shoulder
|
Supraspinatus (assists when GH is between neutral and full external rotation)
-Infraspinatus -Teres minor(SIT!)-Posterior deltoid Produce the smallest isometric torque of any muscle group at the shoulder |
|
|
|
Adduction and extension of the shoulder
|
-Sternocostal head of the pectoralis major
-Latissimus dorsi-Teres major-Long head of triceps-Posterior deltoid-Infraspinatus-Teres minor |
|
|
|
what is the angular orientation of the articulations of the shoulder?
|
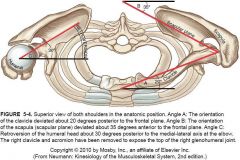
|
|
|
|
Rotation of C1 and C2?
|
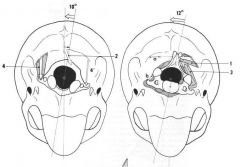
C1 10deg - C2 12deg
|
|
|
|
Elbow joint type?
|
•Ginglymus or hinge-type joint•Allows only flexion & extension
•2 interrelated joints –humeroulnar joint –radiohumeral joints |
|
|
|
As elbow flexes ___ degrees or more, its bony stability is unlocked, allowing for more side-to-side laxity
|
20
|
|
|
|
Stability in ___ is more dependent on the lateral (radial collateral ligament) & the ____ or (ulnar collateral ligament)
|
flexion
medial |
|
|
|
•Ulnar collateral ligament is critical in providing ____ support
|
medial
|
|
|
|
Elbow movement ROM
|
0 degrees of extension to 145 to 150 degrees of flexion
|
|
|
|
•Radioulnar joint
|
–Trochoid or pivot-type joint
–Radial head rotates around at proximal ulna –Distal radius rotates around distal ulna –Annular ligament maintains radial head in its joint |
|
|
|
•Radioulnar joint
|
–Supinate 80 to 90 degrees from neutral
–Pronate 70 to 90 degrees from neutral |
|
|
|
•Synergy between glenohumeral, elbow, & radioulnar joint muscles
|
–As the radioulnar joint goes through its ROM, glenohumeral & elbow muscles contract to stabilize or assist in the effectiveness of movement at the radioulnar joints
–Ex. when tightening a screw with a screwdriver which involves radioulnar supination, we tend to externally rotate & flex the glenohumeral & elbow joints, respectfully |
|
|
|
• Elbow flexors
|
– Biceps brachii
– Brachialis – Brachioradialis – Weak assistance from Pronator teres |
|
|
|
• Elbow extensor
|
– Triceps brachii
– Anconeus provides assistance |
|
|
|
•Radioulnar pronators
|
–Pronator teres
–Pronator quadratus –Brachioradialis |
|
|
|
•Radioulnar supinators
|
–Biceps brachii
–Supinator muscle –Brachioradialis |
|
|
|
•“Tennis elbow"
|
common problem usually involving extensor digitorum muscle near its origin on lateral epicondyle
–known lateral epicondylitis –associated with gripping & lifting activities |
|
|
|
golfer's elbow
|
•Medial epicondylitis
–somewhat less common –associated with medial wrist flexor & pronator group near their origin on medial epicondyle –Both conditions involve muscles which cross elbow but act primarily on wrist & hand |
|
|
|
Forearm Muscles• Anterior
– Primarily flexion & pronation |
• Biceps brachii
• Brachialis • Brachioradialis • Pronator teres • Pronator quadratus |
|
|
|
Upper arm Muscles• Posterior
|
– Primarily
extension & supination • Triceps brachii • Anconeus • Supinator |
|
|
|
•Radial nerve -originates from
|
C5, C6, C7, & C8
–Triceps brachii –Brachioradialis –Supinator (posterior interosseous nerve) –Anconeus –Sensation to posterolateral arm, forearm, & hand |
|
|
|
•Median nerve -derived from
|
C6 & C7
–Pronator teres –Pronator quadratus (anterior interosseus nerve) –Sensation to palmar aspect of hand & first three phalanges, palmar aspect of radial side of fourth finger, dorsal aspect of index & long fingers |
|
|
|
•Musculotaneous nerve -branches from
|
C5 & C6
–Biceps brachii –Brachialis |
|
|
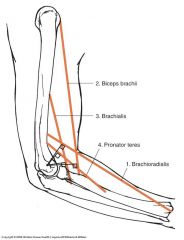
Elbow flexors
|
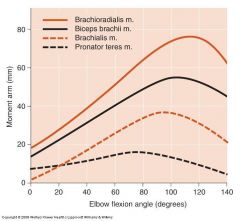
|
|
|
|
Elbow Flexion
•Ex. Biceps curl •Agonists |
–Biceps brachii
–Brachialis –Brachioradialis |
|
|
|
Elbow Extension
•EX. Push-up •Agonists |
–Triceps brachii
•Anconeus |
|
|
|
Radioulnar Pronation
•Agonists |
–Pronator teres
–Pronator quadratus –Brachioradialis |
|
|
|
Radioulnar Supination
•Ex. Tightening a screw •Agonists |
–Biceps brachii
–Supinator muscle –Brachioradialis |
|
|
|
The Wrist & Hand •Relate functional anatomy to joint actions
|
–flexion, extension, abduction ieradial deviation, & adduction ieulnardeviation of wrist & hand
–29 bones –More than 25 joints –More than 30 muscles •18 are intrinsic |
|
|
|
• Carpal bones form a three-sided arch what are some structural components?
|
– concave on palmar side
– bony arch is spanned by transverse carpal & volar carpal ligaments – creates the carpal tunnel – frequently a source of problems known as carpal tunnel syndrome |
|
|
|
•Wrist joint movement?
|
–condyloid-type joint
–allows flexion, extension, abduction, & adduction –motion occurs primarily between distal radius & proximal carpal row (scaphoid, lunate, & triquetrum) |
|
|
|
•Wrist joint ROM?
|
–70 to 90 degrees of flexion
–65 to 85 degrees of extension –15 to 25 degrees of abduction ieradial deviation –25 to 40 degrees of adduction ieulnardeviation |
|
|
|
•Each finger has 3 joints ROM?
|
–Metacarpophalangeal (MCP) joints
•Condyloid •0 to 40 degrees of extension •85 to 100 degrees of flexion –Proximal interphalangeal (PIP) joints •Ginglymus •Full extension to 90 to 120 degrees of flexion –Distal interphalangeal(DIP) joints •Ginglymus •Flex 80 to 90 degrees from full extension |
|
|
|
•Thumb has 2 joints, ROM?
|
–Metacarpophalangeal (MCP) joint
•Full extension into 40 to 90 degrees of flexion •Ginglymus–Interphalangeal (IP) joint •Flex 80 to 90 degrees •Ginglymus–Carpometacarpal (CMC) joint of thumb •Unique saddle-type joint •50 to 70 degrees of abduction •Flex 15 to 45 degrees & extend 0 to 20 degrees |
|
|
|
Extrinsic muscles of wrist & hand grouped according to function & location
•6 muscles move wrist but not fingers & thumb? |
–3 wrist flexors
•flexor carpi radialis •flexor carpi ulnaris •palmaris longus –3 wrist extensors •extensor carpi radialis longus •extensor carpi radialis brevis •extensor carpi ulnaris |
|
|
|
•3 muscles primary flexors of phalanges
|
–Also involved in wrist joint actions
–Generally weaker in their wrist actions –Flexors •Flexor digitorum superficialis •Flexor digitorum profundus •Flexor pollicis longus (thumb flexor) |
|
|
|
wrist Muscles–Extensors
|
•Extensor digitorum
•Extensor indicis •Extensor digiti minimi •Extensor pollicis longus (thumb extensor) •Extensor pollicis brevis (thumb extensor) |
|
|
|
–Abductor of thumb & wrist
|
Abductor pollicis longus
|
|
|
|
•_____ nerve & all ____ tendons except ____ & ___ pass through carpal tunnel
|
Median
flexor flexor carpi ulnaris palmaris longus |
|
|
|
•Wrist abductors
|
also radial deviation
–Generally cross wrist joint anterolaterally& posterolaterallyto insert on radial side of hand •Flexor carpiradialis •Extensor carpiradialislongus •Extensor carpiradialisbrevis •Abductor pollicislongus •Extensor pollicislongus •Extensor pollicisbrevis |
|
|
|
•Wrist adductors
|
also ulnardeviation
–cross wrist joint anteromedially& posteromediallyto insert on ulnarside of hand •Flexor carpiulnaris •Extensor carpiulnaris |
|
|
|
•Intrinsic hand muscles have origins & insertions on bones of hand
–Radial side -four muscles of thumb |
•opponens pollicis
•abductor pollicis brevis •flexor pollicis brevis •adductor pollicis |
|
|
|
•Intrinsic hand muscles have origins & insertions on bones of hand–Ulnar side -three muscles of little finger
|
•opponens digiti minimi
•abductor digiti minimi •flexor digiti minimi brevis |
|
|
|
•Intrinsic hand muscles
|
•4 lumbricals
•3 palmar interossei •4 dorsal interossei |
|
|
|
Muscles•Anteromedially at elbow & forearm and anterior at hand
|
–Primarily wrist flexion
•Flexor carpi radialis •Flexor carpi ulnaris •Palmaris longus |
|
|
|
Muscles •Anteromedially at elbow & forearm and anterior at hand
|
–Primarily wrist & phalangeal flexion
•Flexor digitorum superficialis •Flexor digitorum profundus •Flexor pollicis longus |
|
|
|
Muscles
•Posterolaterally at elbow & forearm and posterior at hand |
–Primarily wrist extension
•Extensor carpi radialis longus •Extensor carpi radialis brevis •Extensor carpi ulnaris |
|
|
|
Nerves
•Radial nerve from |
C6, C7, & C8
–Extensor carpi radialis brevis –Extensor carpi radialis longus |
|
|
|
•Posterior interosseous nerve from radial nerve
|
C6, C7, & C8
–Extensor carpi ulnaris –Extensor digitorum –Extensor digiti minimi –Abductor pollicis longus –Extensor pollicis longus –Extensor pollicis brevis –Extensor indicis |
|
|
|
•Median nerve -arising from
|
C6, C7, C8, & T1
–Flexor carpi radialis –Palmaris longus –Flexor digitorum superficialis |
|
|
|
•Anterior interossseous nerve from median nerve
|
–Flexor digitorum profundus for index & long finger
–Flexor pollicis longus –Intrinsic muscles •abductor pollicis brevis, flexor pollicis brevis (superficial head), opponens pollicis, and 1st& 2ndlumbrical |
|
|
|
Nerves
•Ulnar nerve -branching from |
C8 & T1
–Flexor digitorum profundus for 4th& 5thfingers –Flexor carpi ulnaris –Remaining intrinsic muscles •flexor pollicis brevis (deep head), adductor pollicis, palmar interossei, dorsal interossei, 3rd& 4thlumbrical, opponens digiti minimi, abductor digiti minimi, & flexor digiti minimi brevis –Sensation to ulnar side of hand, ulnar one-half of ring finger & entire little finger |
|
|
|
Intrinsic Muscles of the Hand
•Thenar eminence -muscular pad on palmar surface of 1stmetacarpal |
–abductor pollicis brevis
–opponens pollicis –flexor pollicis brevis –adductor pollicis |
|
|
|
Intrinsic Muscles of the Hand
•Hypothenar eminence -muscular pad that forms ulnar border on palmar surface |
–abductor digiti minimi
–flexor digiti minimi brevis –opponens digiti minimi |
|
|
|
Intrinsic Muscles of the Hand •Intermediate muscles
|
–three palmar interossei
–four dorsal interossei –four lumbrical muscles |
|
|
|
Intrinsic Muscles of the Hand
•Four muscles act on CMC of thumb |
–opponens pollicis -opposition in thumb metacarpal
–abductor pollicis brevis & flexor pollicis brevis abduct thumb metacarpal –flexor pollicis brevis flexes thumb metacarpal –adductor pollicis adducts thumb metacarpal –flexor pollicis brevis & adductor pollicis flex proximal phalanx of thumb |
|
|
|
Intrinsic Muscles of the Hand
|
•Three palmar interossei
–adduct the 2nd, 4th, & 5thphalanges •Four dorsal interossei –flex & abduct index, middle, & ring proximal phalanxes –assist with extension of middle & distal phalanxes of index, middle, & ring fingers •Third dorsal interossei –adducts middle finger •Four lumbricales –flex index, middle, ring, & little proximal phalanxes –extend middle & distal phalanxes of index, middle, ring, & little fingers. |
|
|
|
Intrinsic Muscles of the Hand•Three muscles act on little finger
|
–opponens digiti minimi causes opposition of little finger metacarpal
–abductor digiti minimi abducts 5thmetacarpal –flexor digiti minimi brevis flexes 5thmetacarpal |
|
|
|
Wrist Flexion
•Agonists |
–Flexor carpi radialis
–Flexor carpi ulnaris –Palmaris longus –Flexor digitorum superficialis –Flexor digitorum profundus –Flexor pollicis longus |
|
|
|
Wrist Extension
•Agonists |
–Extensor carpi radialis longus
–Extensor carpi radialis brevis –Extensor carpi ulnaris –Extensor digitorum –Extensor indicis –Extensor digiti minimi –Extensor pollicis longus –Extensor pollicis brevis |
|
|
|
Wrist Abduction ieulnardeviation
•Agonists |
–Flexor carpi radialis
–Extensor carpi radialis longus –Extensor carpi radialis brevis –Abductor pollicis longus –Extensor pollicis longus –Extensor pollicis brevis |
|
|
|
Wrist Adduction ieradial deviation
•Agonists |
•Flexor carpi ulnaris
•Extensor carpi ulnaris |
|
|
|
Phalangeal Flexion
•Agonists |
–Flexor digitorum superficialis
–Flexor digitorum profundus –Flexor pollicis longus |
|
|
|
Phalangeal Extension
•Agonists |
–Extensor digitorum
–Extensor indicis –Extensor digiti minimi –Extensor pollicis longus –Extensor pollicis brevis |
|
|
|
Wrist: The every day functional ROM
|
10º flexion,
35º extension, 10º radial deviation, 15º ulnar deviation. Optimal every-day (functional) hand/wrist position: 10-15 degrees extension and 10 degrees ulnar deviation. |
|
|
|
The wrist is a double-joint system:
Occurring both the ____ and the ___ joints (predominantly capitate) |
radiocarpal
midcarpal |
|
|
|
Midcarpal joint has ___axes of rotation, both through _____.
|
2
head of capitate |
|
|
|
The ___ and head of the ___ both translate palmar with dorsal rotation (extension).
|
Lunate
capitate |
|
|
|
A total of ___degrees of extension is achieved by minimal rotation of each carpal bone.
|
60
|
|
|
|
Full extension elongates the palmar ____ligament, palmar capsule and wrist/finger______ muscles. (i.e. Act as stabilizers and creates the close-packed position of the wrist).
|
radiocarpal
flexor The wrist flexion is similar to extension but in reverse fashion. The wrist is not very stable in flexion. |
|
|
|
•Rotation (ulnar deviation) occurs as the _____ rotates ulnarly and slides radially on the ____ and _____and vice versa for radial deviation
|
capitate
lunate & scaphoid •Scaphoid, lunate, and triquetrum slide/roll radially and ulnarly |
|
|
|
•The proximal carpal row slightly ______during ulnar deviation (scaphoid in ____º ____) –FUNCTIONAL position of the wrist.
|
extends
20º extension |
|
|
|
Rotational collapse of wrist
|
The mobile proximal row of carpal bodies is intercalated between two rigid structures (the forearm and the distal row of carpal bones) and is thus prone to a rotational collapse in a zig-zag fashion when compressed from both ends.
|
|
|
|
•The strongest wrist flexors are
|
flexor digitorum profundus and superficialis.
|
|
|
|
•The strongest wrist extensors
|
the extensor carpi ulnaris and the extensor digitorum.
|
|
|
|
Primary wrist extensor muscles:
|
•Extensor carpi radialis longus
•Extensor carpi radialis brevis •Extensor carpi ulnaris |
|
|
|
Secondary wrist extensor muscles:
|
•Extensor digitorum
•Extensor indicis •Extensor digiti minimi •Extensor policis longus |
|
|
|
Primary wrist flexor muscles:
|
•Flexor carpi radialis
•Flexor carpi ulnaris •Palmaris longus |
|
|
|
Secondary wrist flexor muscles:
|
•Flexor digitorum profundus
•Flexor digitorum superficialis •Flexor policis longus |
|
|
|
Radial deviators of the wrist:
|
•Extensor carpi radialis longus
•Extensor carpi radialis brevis •Extensor carpi ulnaris •Extensor policis brevis •Flexor carpi radialis •Abductor policis longus •Flexor policis longus |
|
|
|
Ulnar deviators of the wrist:
|
•Extensor carpi ulnaris
•Flexor carpi ulnaris |
|
|
|
Maximum grip strength is obtained with approximately ___ degrees wrist extension.
|
30
|
|
|
|
Palmar surface is concave with three integrated arch systems: They are?
|
2 transverse (Proximal and Digital) + 1 longitudinal
|
|
|
|
•Thumb is rotated __degrees medially (internally) relative to the other digits.
|
90
|
|
|
|
Kinematics of the Thumb
|
•Abduction and adduction
•Flexion and extension •Opposition and reposition (combination of the two other planes of motion). |
|
|
|
OPPOSITION of theThumb - Motion is divided into two phases:
|
In phase one, the thumb metacarpal abducts. In phase two, the abducted metacarpal flexes and medially rotates across the palm towards the little finger
|
|
|
|
Zig-zag deformity of the fingers
Swan-neck deformity: |
Hyperextension of PIP joint
Flexion of DIP joint |
|
|
|
Zig-zag deformity of the fingers: Boutonniere deformity:
|
Flexion of PIP joint
Hyperextension of DIP joint |
|
|
|
Composition of cartilage?
|
•70-85% of weight is water (65-80% of the total weight).
•Water is most concentrated near the articular surface (80%) •Decreases in a near-linear fashion with increasing depth (65% in the deep zone). •The fluid contains free mobile cations Na+, K+ Ca++, which greatly influence mechanical behaviours of the cartilage •The remainder is primarily proteoglycans (PGs) and collagen type II fibers. |
|
|
|
mechanical behaviours of cartilage:
|
•Viscoelasticity
•Bi-phasic creep response in compression •Stress-relaxation response under compression •Permeability of articular cartilage |
|
|
|
Articular cartilage has only a limited capacity for repair and regeneration, and if subjected to an abnormal range of stresses can quickly undergo total failure.
It is hypothesised that the following biomechanical factors relates to failure progression: |
1. The magnitude of the imposed stress
2. The total number of sustained peaks 3. The changes in the intrinsic molecular and microscopic structure of the collagen-PG matrix 4. The changes in the intrinsic mechanical property of the tissue |
|
|
|
Internal and External Force Effects on COG, •Objects in Flight
|
–No external force
–Whole body system –COG not effected by internal forces –I.F. serve to change shape only |
|
|
|
Internal and External Force Effects on COG•Generate force against support
|
–Reaction Force
–External Force •Responsible for moving COG |
|
|
|
Mechanical Loads on the Body
|
•Compression
•Tension •Shear •Stress –Torsion –Bending –Combined Loads |
|
|
|
Effects of Loading
|
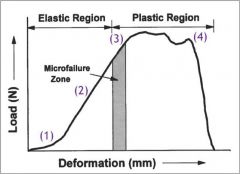
|
•Load-Deformation Curve
•Yield Point or Elastic Limit •Failure •Repetitive vs Acute |
|
|
Newton’s Laws of Motion •First Law
|
–Law of inertia
–A body will maintain a state of rest or constant velocity unless acted on by an external force that changes the state |
|
|
|
Newton’s Laws of Motion •Second Law
|
–Law of Acceleration
–A force applied to a body causes an acceleration of that body of a magnitude proportional to the force, in the direction of the force, and inversely proportional to the body’s mass |
|
|
|
Newton’s Laws of Motion
•Third Law |
–Action-Reaction
–When one body exerts a force on a second, the second body exerts a reaction that is equal in magnitude and opposite in direction on the first body |
|
|
|
Newton’s Law of Gravitation
|
•All bodies are attracted to one another with a force proportional to the product of their masses and inversely proportional to the distance between them
•Greater the mass the greater the attraction •Further apart less attraction |
|
|
|
Friction
|
•Force that acts at the interface of surfaces in contact
•Occurs in the direction opposite the impending motion •Static Friction •Maximum Static Friction •Kinetic (Sliding) Friction |
|
|
|
Factors that Influence the Outcome when Two Bodies Collide
|
•Elasticity of the two objects
•Direction of Impact |
|
|
|
Oblique Impact with Moving Bodies
•Six Variables to consider |
–Velocity of object 1
–Velocity of object 2 –Angle created by the vectors from 1 and 2 –Mass of object 1 –Mass of object 2 –Mutual coefficient of restitution |
|
|
|
•instantaneous velocity (v) is?
|
slope (tangent) to the displacement-time curve at a particular instant
|
|
|
|
Factors to take into account when assessing muscle strain are:
|
•Low strength
•Reduced flexibility •High risk player •Early season •Must-win game |
|
|
|
Active Motion
|
•Is the movement of a joint in a specific direction through its range of motion, determined by the actionof the voluntary muscles
|
|
|
|
Passive Motion
|
•Is the movement of a joint in a specific direction through its range of motion, determined by its structural ligamentous integrity withoutvoluntary muscle activity.
|
|
|
|
The goal of Motion Palpation MP is to assess the:
|
•Quantity:How much does the joint move?
•Quality:How does the joint move through its ROM? •Joint play:What is the quality of resistance (too much or too little)? •End feel:At what point is the end feel encountered, what is the quality of resistance, and at what point does the motion stop? •Symptoms:Changes in the amount or the location during assessment and motion? |
|
|
|
Joint Play
|
•The qualitative evaluation of the joint’s resistance to movement when it is in a neutral or loose-packed position.
•It is the best opportunity to isolate the joint capsule from its periarticular muscles. •Evaluated by a small magnitude, springing movement of the joint. •Is the discrete, short-range movement of a joint independent of the action of voluntary muscles, determined by springing the joint in the neutral position |
|
|
|
End Play / End Feel
|
•The qualitative assessment of the end play zone (EPZ).
•Evaluated by applying additional overpressure to the specific joint at the end range of passive movement. •Characterised as a sense of increasing restriction towards first stop and a firmer resistance at its limits (second stop). •Is the discrete, short-range movement of a joint independent of the action of voluntary muscles, determined by springing the joint at the limit of the passive range of motion (the end range). |
|
|
|
End Feel
•Capsular |
•Firm but giving
•Increasing resistance with increasing length •Example: ext. Rotation of shoulder •Abnormal: capsular fibrosis or adhesions leading to a capsular pattern |
|
|
|
End Feel•Ligamentous
|
•Like capsular, but slightly firmer quality
•Example: knee extension •Abnormal: abnormal resistance because of ligament shortening |
|
|
|
End Feel
•Soft tissue approximation |
•Giving / squeezing
•Results from approximation of soft tissue (painless) •Example: Elbow flexion •Abnormal: muscle hypertrophy, soft tissue swelling |
|
|
|
End Feel•Bony
|
•Hard, non-giving
•Example: Elbow extension •Abnormal: bony exostosis, articular hypertrophy |
|
|
|
End Feel
•Muscular |
•Firm, but giving
•Increases with elongation (not as stiff as capsular or ligamentous) •Example: Hip flexion •Abnormal: muscle hypertrophy or hypotrophy |
|
|
|
End Feel•Muscle spasm
|
•Guarded, resisted by muscle contraction
•End feel cannot really be assessed •Abnormal: protective muscle splinting as a result of joint injury/disease |
|
|
|
End Feel
•Interarticular |
•Bouncy, springing quality
•Abnormal: meniscal tear |
|
|
|
End Feel•Empty
|
•Normal end feel resistance is missing, unusual give
•End feel is not encountered at normal point •Abnormal: hypermobility or instability |
|
|
|
Joint cavitation (audible release)
|
•ANormal joint.
•BLong axis distraction. •CElastic recoil of capsule. •DSudden increased volume decreases capsule tension. •EStimulating high-threshold receptors. •FGases coalesce into central area. |
|
|
|
•Bursa•Bursa
|
–Fibrous, fluid-filled sac that reduces friction
–Located between bones, tendons, and other structures |
|
|
|
•Subacromial bursa
|
–Bursa between acromion process and insertion of supraspinatus muscle
|
|
|
|
–17 muscles that contribute to scapula and shoulder joint movements are listed
|
–Major muscles
–Deltoid, trapezius, rhomboids, pectoralis major, latissimus dorsi, serratus anterior –Rotator cuff (4 muscles surrounding shoulder joint) ¯Infraspinatus, supraspinatus, teres minor, subscapularis |
|
|
|
•Sprain
•Subluxation |
–Rupture of fibers of ligament
|
|
|
|
17 muscles that contribute to scapula and shoulder joint movements are listed
|
–Major muscles
–Deltoid, trapezius, rhomboids, pectoralis major, latissimus dorsi, serratus anterior –Rotator cuff (4 muscles surrounding shoulder joint) ¯Infraspinatus, supraspinatus, teres minor, subscapularis |
|
|
|
•Sprain
•Subluxation •Ectopic calcification |
–Rupture of fibers of ligament
–Partial dislocation –Hardening of organic tissue through deposit of calcium salts in areas away from the normal sites |
|
|
|
•Impingement syndrome
|
–Irritation of structures above shoulder joint
–Due to repeated compression between greater tuberosity and acromion process |
|
|
|
•Carrying angle
|
–Angle between ulna and humerus with elbow extended
–10–20° |
|
|
|
•Osteochondritis dissecans
|
–Inflammation of bone and cartilage resulting in splitting pieces of cartilage into the joint
|
|
|
|
Carpal bone articulations
|
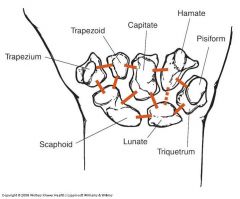
|
|