![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
166 Cards in this Set
- Front
- Back
|
Stroma refers to... |
Cells embedded in the extracellular matrix |
|
|
Extracellular matrix is secreted by these cells |
Fibroblasts |
|
|
Stromal cells are derived from this cell lineage |
Mesodermal |
|
|
The layer separating epithelia from connective tissue is called the: |
Basal Lamina |
|
|
Three ways ECM regulates cell function? |
-signaling through surface receptors (integrins) -Regulating growth factor signals -Degradation products from ECM can affect cell function |
|
|
Fibronectin, laminin, and vitronectin all serve this purpose in the ECM They are these type of ECM proteins |
Help cells attach fibrous, adhesive |
|
|
Collagens are these type of molecules made of these type of chains: |
Trimeric; alpha |
|
|
A collagenous domain is: |
A triple helical region where every third AA is a glycine |
|
|
Collagens are divided into these types: |
Fibrillar, non-fibrillar |
|
|
"long unbranched polysaccharides consisting of a repeating disaccharideunit" describes: |
Glucosaminoglycans |
|
|
The main collagen in tendons, bone, ligaments, dentin, and skin is: |
Type 1 |
|
|
Where is type 2 collagen? |
Mainly in the cartilage matrix |
|
|
OI results from a mutation of either one of these genes, which code for: |
COL1A1, COL1A2; type 1 collagen |
|
|
Chrondrodysplasias result from a mutation in this type of collagen gene |
Type 2 |
|
|
Type one collagen is a ___trimer, and type two collagen is a ___trimer |
hetero, homo |
|
|
Type IV and type VI collagen can be found where? |
Basement membranes |
|
|
The anchoring fibrils that attach epithelia to the underlying tissue are composed of this type of collagen |
Type VII |
|
|
Dystrophic epidermis bullosa is a result of a mutation in this gene that makes this type of collagen |
COL7A1, Type VII |
|
|
A highly glycosolated protein is called a: |
Proteoglycan |
|
|
Dentinogingival/Alveogingival collagen serves this function: |
Holds free gingiva onto tooth |
|
|
What kind of collagen encircles the tooth? |
Circumferential |
|
|
What kind of collagen holds attached gingiva to bone? |
Periosteal |
|
|
This type of collagen runs between teeth |
Transseptal |
|
|
What type of fibers provide elasticity for tooth movement? Where are they located? What are they made of? |
Oxytalan fibers; periodontal ligament; fibrillin |
|
|
A mature collagen model to be used to make collagen fibrils is called: |
Tropocollagen |
|
|
Vitamin C is a cofactor for these hydroxylases which serve this function: |
prolyl, lysyl; hydroxylates prolines and lysines before triple helix formed. |
|
|
The collagen triple helix is right or left handed? |
Right |
|
|
A single collagen helix is right or left handed? |
Left |
|
|
Osteogenesis imperfecta types I, II, III, IV are all ___ ___ whereas types VII thru XVI are ___ ___ |
autosomal dominant, autosomal recessive |
|
|
The most severe form of OI is: |
Type 2 |
|
|
The most common form of OI leads to this happening with collagen: |
Trimers form, but less normal collagen 1 made |
|
|
In type 2 OI, this happens to collagen |
Abnormal pro-collagen chains are formed, breaking gly-x-y pattern, resulting in bad collagen (few normal collagen trimers) |
|
|
Progressive deforming/easily fractured bone OI is also called Type ___ OI |
3 |
|
|
These types of OI don't have mutations in collagen I genes |
Types V, VI, VII |
|
|
Type 1 DI is associated with this disease |
OI |
|
|
DSPP mutations yield this disease |
Type II DI |
|
|
Goodpasture syndrome results from autoantibody attack on this type of collagen |
IV |
|
|
Type III and type V collagen mutations will often result in this disease |
Ehlers-Danlos syndrome |
|
|
Alport's syndrome, glomerular filtration issues, and basement membrane problems are often a result of a mutation in this type of collagen gene: |
IV |
|
|
Mutations in type VII collagen often result in this disease: |
Epidermolysis bullosa |
|
|
This molecule is expressed in high volumes in osteoblasts: |
Alkaline phosphotase |
|
|
Osteoblasts produce a lot of this type of collagen |
Type 1 |
|
|
Hypophosphatasia is a result of a mutation in the gene that produces this, which serves this function: |
Alkaline phosphatase; hydrolyzes an inhibitor of mineralization to deactivate it, promoting increase in phosphate concentration to increase local mineralization |
|
|
TNSALP codes for: |
Alkaline phosphatase |
|
|
Mutations in RUNX2 result in this disease: |
Cleidocranial dysplasia
|
|
|
Missing clavicles and supernumary teeth are symptoms of this disease: |
Cleidocranial dysplasia |
|
|
"ectopicmineralization in non-skeletal soft tissues, leading to sheets, plates of bonesforming across the ribs, joints" describes this disease: |
Fibrodysplasia Ossificans Progressiva (Stone man syndrome) |
|
|
Stone man syndrome occurs as a result in the mutation of this gene |
ACVR1 |
|
|
Mutations in ACVR1 result in this disease, and the gene codes for this type of protein: |
Fibrodysplasia ossificans progressiva; BMP Type 1 receptor |
|
|
What is the morphological result of reduced amounts of sclerostin? |
Increased bone mass |
|
|
Sclerostosis and Van Buchem's diseases will occur as a result of the mutation of this protein: |
SOST- codes for sclerostin |
|
|
When bones are unnaturally dense yet prone to fracture, you are dealing with this disease |
Osteopetrosis |
|
|
Mutations in genes required to code proteins for osteoclast resorption often result in this disease |
Osteopetrosis |
|
|
In osteoporosis, what is the problem that generates the disease in regards to bone cellular functions? |
Bone resorbed by osteoclasts will not be sufficiently regenerated by osteoblasts |
|
|
An anti-resorptive agent does what? |
Inhibits bone resorption |
|
|
What's the name of a drug that stimulates bone formation? |
Bone anabolic agent |
|
|
WNT/Beta-catenin is involved in these four steps in regards to bone cell differentiation: |
-Mesenchymal stem cells to osteoprogenitors -Osteoprogenitors to immature osteoblasts -Maturation of osteoblasts -Differentiation of osteoblasts (into osteocytes, apoptosis, or lining cells) |
|
|
Activating LRP5 mutations will do this to bone mass, whereas inactivating mutations will do this:
|
-Activating: increase -Deactivating: decrease |
|
|
BMP's 2 and 7 are essential for this step in bone cell development: |
Differentiation of mesenchymal cells to osteoprogenitor cells |
|
|
What is the official term for bone that forms in the wrong place? |
Heterotopic bone formation |
|
|
Bone that is dead without viable osteocytes is called: |
Osteonecrotic bone |
|
|
From what cells do osteoclasts originate? |
Hematopoietic cells; specifically macrophage/monocyte lineage |
|
|
Osteoclasts regulate these two other aspects of bone formation: |
-Activity of osteoblasts; phosphate homeostasis |
|
|
Osteoclastic resorption is required for these essential bone-building processes: |
-Longitudinal bone growth -Tooth eruption -Orthodontic tooth movement |
|
|
Use of bisphosphonates (which do what?) is associated with this disorder of bone: |
Inhibits bone resorption; osteonecrosis of the jaw |
|
|
What is the lifespan of osteocytes? |
Decades |
|
|
The inhibitor sclerostin is secreted via these cells to affect these cells |
osteocytes; osteoblasts |
|
|
FGF23, DMP1, PHEX, and MEPE are all expressed by this type of cell and serve this general function |
Osteocytes; regulate phosphate homeostasis |
|
|
How long is the lifespan of osteoclasts? |
Days |
|
|
What is the "master transcriptional factor" for osteoclasts? |
NFATc1 |
|
|
Osteopetrosis can result from impaired function of this type of cell |
Osteoclasts |
|
|
What is the normal range for serum calcium concentration? (mg/dL) |
8.5-10.5 mg/dL |
|
|
What is the biologically active fraction of calcium in the serum? (%) What form is this calcium in? |
45%; ion |
|
|
How much calcium is absorbed daily by the gut? How much is excreted daily in the urine? How much calcium is released daily in bone? How much calcium is deposited daily in bone? |
Gut: 200mg Bone: 500mg |
|
|
How much dietary phosphorus is absorbed via the gut? (% range) |
80-90% |
|
|
What is the standard serum Pi range? (mg/dL) |
2.5-4.5mg/dL |
|
|
TRP's serve what function in calcium homeostasis? |
Uptake from apical side of cell |
|
|
What do calbindins do? |
transcellular support of calcium |
|
|
What is responsible for extrusion of calcium on the basal surface of the cell? |
Calcium ATPases or Na dependent calcium exchangers |
|
|
What are the three steps of calcium uptake? |
-Uptake from apical side -Transcellular transport -Extrusion from basal surface |
|
|
What transporter takes up phosphate in the gut? What section of the gut is this transporter located? |
NaPi-IIb; ileum |
|
|
TRPV6 is responsible for what, where? |
Calcium uptake in the gut |
|
|
What are the major hormones regulated calcium homeostasis? (3) Phosphate homeostasis? (3) |
Ca: PTH, Calcitriol (Vit.D), Calcitonin PO4: PTH, Calcitriol, FGF23 |
|
|
What organ releases calcitonin? What's the effect of this hormone on its three target organs? |
-Thyroid; decrease release of Ca in bone, decrease uptake of Ca in gut, decrease reabsorption of Ca in kidney |
|
|
Increasing calcium release from bone, increasing calcium uptake in the gut, and increasing reabsorption of calcium in the kidney are all effects of this hormone in response to this level of calcium in serum: |
PTH; low |
|
|
Where are calcium sensing receptors located? |
The parathyroid gland |
|
|
In the case of high serum calcium; -Is CaSR signalling increased or decreased? -Is PTH secretion increased or decreased? |
-CaSR signalling is increased. -PTH secretion is decreased |
|
|
What effect does PTH have on phosphate reabsorption in the kidney? |
Decrease |
|
|
What's the function of PTH in regards to vitamin D? Where does this function occur? |
PTH stimulates the change of [25(OH)D3] to the active form of [1-25(OH)D3];the kidney |
|
|
What type of protein has its expression frequency changed by Vitamin D3? In what way? |
Calbindins; expression goes up |
|
|
What is the function of Vitamin D3 on PTH production? |
Inhibitory; decreases |
|
|
Vitamin D3 has three effects on phosphate homestasis. What are they? |
-Increased intestinal uptake -Increased reabsorption in kidney tubules -Increased release in to circulation from bone |
|
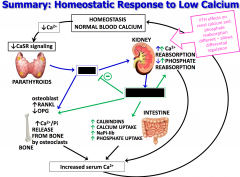
What belongs in the blue box? What belongs in the green box? |
Blue: PTH Green: Vitamin D |
|
|
What cells respond directly to calcitonin? How? |
Osteoclasts; retract their ruffled border |
|
|
When is FGF23 expression induced? Where? |
When serum phosphate is too high- primarily in osteocytes, but also in o-blasts, lining cells, etc |
|
|
What is the main mechanism for phosphate homeostasis regulation? |
Kidney reabsorption |
|
|
PTH has what effect on phosphate reabsorption? How? |
Inhibits; by inhibiting NaPiIIa and NaPiIIc in the kidney tubules |
|
|
FGF23 has what effect on serum phosphate? |
Lowers |
|
|
Net effects of PTH, calcitonin, FGF23, and Vitamin D on Ca and PO4 serum levels? |
PTH: Calcium up, phosphate down Calcitonin: Calcium down Vitamin D: Calcium up, phosphate up FGF23: Phosphate down |
|
|
Six symptoms of hypocalcemia? |
-Muscle cramping -Increased neuromusc. excitability -Muscle spasms -Fatigue -Cardiac dysfunction -Depression, psychosis, seizures |
|
|
Hypoparathyroidism can result in this status in regards to serum calcium levels |
Hypocalcemic |
|
|
Pseudohypoparathyroidism results from this bodily response to PTH; results in this status in regards to serum levels of calcium: |
PTH resistance; hypocalcemic |
|
|
Mutations in VDR or 1-alpha hydroxylase result in this disease: This condition has this effect on serum calcium levels |
Rickets; vitamin D resistance. Decreases serum calcium levels (hypocalcemic) |
|
|
DiGeorge syndrome is associated with this irregular anatomy, and results in this classified disorder |
Lack of parathyroid glands; hypoparathyroidism |
|
|
Activating CaSR mutations results in what physiological response, and what blood serum outcome? |
Decreased calcium reabsorption in kidney as a result of incorrect reading of calcium levels as high by CaSR and parathyroid; leads to hypocalcemia |
|
|
Osteomalacia manifests in this symptom |
Soft bones- as a result of a failure of osteoid to calcify |
|
|
Type 1 Vitamin D dependent rickets results from a mutation in this: |
renal 25-OH-vitamin D-1α-hydroxylase |
|
|
The serum difference which distinguishes VDDR1 and 2 is: |
VDDR1 has very low serum Vitamin D3. VDDR2 has very high serum VD3. |
|
|
Vitamin D Dependent Rickets Type 2 is caused by: |
Defects in the Vitamin D receptor |
|
|
Which type of VDDR is associated with alopecia? |
VDDR2
|
|
|
Oversecretion of PTH not responsive to CaSR signalling results in: |
Hyperparathyroidism |
|
|
Mutations in tumor suppressor genes can lead to tumors in endocrine tissues. What is the name of these tumors, and what are 2 genes which can be mutated to result in them? What is the serum molecular alteration that results? |
Multiple endocrine neoplasias; MEN1, MEN2A |
|
|
Chronic renal failure can result in this type of hyperparathyroidism. What's the other condition that can bring about this type of hyperparathyroidism? |
Secondary -Vitamin D malabsorption |
|
|
XLH is due to mutations in what gene? What does this gene do? |
PHEX; inhibits FGF23 production. (leads to hypophosphatemia because FGF23 never inhibited, endlessly produced |
|
|
What disease results from mutations in FGF23 disabling its cleavage? How does this affect phosphate levels? |
Autosomal dominant hypophosphatemic rickets (ADHR); decreases phosphate levels because FGF23 is never destroyed |
|
|
What does DMP1 do? What disease results from the mutation of DMP1? |
DMP1 inhibits FGF23 production. Autosomal recessive hypophosphatemic rickets results from mutation of DMP1. |
|
|
Loss of function mutation is NaPiIIc results in what disease? What is the result of this mutation? |
Hereditary hypophosphatemic rickets with hypercalciuria (HRHH) -Inefficient reabsorption of Pi in kidney. |
|
|
Tumor induced osteomalacia happens because: |
Tumors secrete FGF23 into the bloodstream. Lowers Pi independent of serum concentration levels |
|
|
Inactivating mutations in FGF23 can lead to this serum status: |
Hyperphosphatemia |
|
|
What are familial tumoral calcinoses? |
Inherited disorders which result in an excess of serum phosphate- hyperphosphatemic state |
|
|
What are the four phases of skeletal formation? |
-Migration of preskeletal cells -Interaction of these cells with epithelial cells -Mesenchymal condensation -Differentiation to chondroblasts or osteoblasts by mesenchymal cells |
|
|
During fracture repair, this method of bone formation is used. It is the primary method of bone formation for most bones in the body |
Endochondral |
|
|
This method of bone formation could be referred to as indirect. Why? |
Endochondral; mesenchyme forms a cartilaginous template first |
|
|
When mesenchymal cells differentiate directly into osteoblasts, this type of ossification has occurred: |
Intramembranous |
|
|
In bony remodeling, what type of bone do we start with, and what type do we end up with? |
Woven changes to lamellar |
|
|
Compact and cancellous bone are both subgroups of this type of bone: |
Lamellar/(secondary) |
|
|
Trabecular bone is another name for this type of bone: |
Cancellous |
|
|
Haversian canals occur in this type of lamellar bone |
Compact |
|
|
What are the four stages of fracture repair? |
1) Formation of hematoma 2) Formation of fibrocartilage callous 3) Tissue metaplasia; we switch that fibrocartilage out for bone 4) Remodeling and turnover occurs to attempt to make bone look like what it was before break |
|
|
Inflammatory cytokines associated with hematoma? (5) |
-TNF-alpha -Interleukins (IL) 1, 6, 11, 18 |
|
|
What lays down the fibrous connective tissue matrix of the first callous in fracture repair? |
Fibroblasts |
|
|
In hypoxic regions post-fracture, what step initiates endochondral ossification? |
Mesenchymal stem cells differentiate into chondrocytes |
|
|
Osteogenic precursor cells come primarily from this tissue layer |
Periosteum |
|
|
The first bone that appears in the formation of a bony callous is of this type: |
Woven |
|
|
What are three angiogenic factors involved in the fracture repair process? |
-PDGF -VEGF -ANGPT (angiopoietin) |
|
|
What are the three TGF-beta superfamily members involved in bone repair? |
-TGF-beta -BMP-2 -GDF-8 |
|
|
What are the two primary roles of TGF-beta superfamily growth factors? |
-Promote ECM synthesis, and assembly/initiation of callous formation -Promote osteogenic differentiation |
|
|
Macrophages, mesenchymal cells, and inflammatory cells secrete these small chemical signals during bone repair |
Inflammatory cytokines |
|
|
High strain on an area undergoing fracture healing has what effect? |
Promotes fibrous tissue |
|
|
What conditions promote cartilage formation in bone repair? |
Intermediate strain, low O2 tension. |
|
|
Low strain and high O2 tension promotes what substance to form during fracture healing? |
Intramembranous Bone |
|
|
In fracture healing, what releases TGF-beta? |
Platelets in hematoma |
|
|
Cartilage is vital for this type of bone formation |
Endochondral |
|
|
What collagen types predominate hyaline cartilage? |
II, X |
|
|
Elastic cartilage is found in these three locations: |
-Eustachian tubes -Epiglottis -Ear lobes |
|
|
The pubic symphysis, TMJ, and intervertebral disks are all composed of this type of cartilage: |
Fibrocartilage |
|
|
Type 1 and Type 2 collagen make up the extracellular matrix of this type of cartilage: |
Fibrocartilage |
|
|
What is the master transcriptional factor for endochondral bone formation? |
SOX9 |
|
|
Hypertrophic chondrocytes produce this growth factor which stimulates angiogenesis |
VEGF |
|
|
When is SOX9 turned off? What is turned on to signal the next stage of bone genesis? |
The hypertrophic stage of epipheseal plate growth; RUNX2, Osterix |
|
|
IHH, PTHrP, VEGF, and FGFs all represent this class of molecules and are involved in this phase of bone formation |
Signalling molecules; chondrocyte differentiation |
|
|
Where is PTHrP expressed? What does it do? |
The ends of bones during bone growth; keeps pre-hypertrophic cells proliferating and prevents them from entering hypertrophic phase |
|
|
What stage of cell growth in bone formation promotes production of Indian Hedgehog Protein (IHH)? What's the function of IHH? |
Hypertrophy; Stimulates PTHrP production to keep chondrocytes proliferating in the pre-hypertrophic phase |
|
|
What type of signaling inhibits chondrocyte proliferation? What type promotes it? |
FGF; BMP |
|
|
Achondrodysplasia comes as a result of mutation in which gene? |
FGFR3 |
|
|
Dwarfism as a result of a mutation in FGFR3 gene is a symptom of this greater systemic disease |
Achondrodysplasia |
|
|
What is the main proteoglycan in cartilage? |
Aggrecan |
|
|
Loss of function mutation in SOX9 results in what disease? What is the genetic pattern of expression for this kind of mutation? |
Camplomelic Dysplasia; Autosomal dominant |
|
|
What is the receptor of IHH? PTHrP? |
PTC1; PTH1R |
|
|
FGFR3; -Expressed where? -Functions (2)? |
-Proliferating chondrocytes -Limits chondrocyte proliferation, -Suppresses IHH |
|
|
Stickler syndrome demonstrates this level of disease severity; results from a mutation in this gene: |
Mild; Type 2 collagen |
|
|
Spondyloepiphyseal dysplasia results from a mutation in this gene, and demonstrates with this phenotype |
COL2A1; dwarfism |
|
|
What does aggrecan assemble with in order to form giant aggregates? |
Hyaluronan |
|
|
How many articular surfaces are present in the TMJ? |
3 |
|
|
Intrascapular TMJ disorders are referred to as being of the ___ type |
articular |
|
|
Rheumatoid arthritis can lead to this type of TMJ disorder |
Articular |