![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
233 Cards in this Set
- Front
- Back
|
What have all introduced inhaled anesthetics after 1950 contained, and what is the exception?
|
Fluorine, with the exception being ethyl vinyl ether
|
|
|
What is unique about all introduced inhaled anesthetics beginning with halothane?
|
They have all been nonflammable |
|
|
Problem with chloroform
|
Was associated with several unexplained intraoperative deaths of otherwise healthy patients, and there were numerous cases of hepatotoxicity |
|
|
Fluorine chemistry
|
Techniques and fluorine chemistry were developed from efforts to produce the first atomic weapons, but found the fortuitous socially beneficial purpose in providing a method of synthesizing modern inhaled anesthetics to my: modern inhaled anesthetics are halogenated partly or entirely with fluorine, which provides greater stability and less toxicity |
|
|
What were the advantages of halothane compared to older anesthetics?
|
It was nonflammable, had a pleasant odor, have low toxicity, and had pharmacokinetic properties allowing faster induction and emergence compared to each other |
|
|
Problems with halothane
|
After four years of use reports of fulminant hepatic necrosis began to appear; halothane also sensitizes the myocardium to the dysrhythmiogenic effects of catecholamines |
|
|
When was it enflurane introduced in clinical practice?
|
1972
|
|
|
Advantages of enflurane
|
Unlike halothane, it did not sensitize the heart catecholamines, and it was not associated with hepatotoxicity
|
|
|
Problems with enflurane
|
It was metabolized to inorganic fluoride and could cause evidence of seizure activity on the EEG, especially when administered at high concentrations and in the presence of hypocapnia
|
|
|
When was isoflurane introduced?
|
1980
|
|
|
Advantages of isoflurane
|
It was not associated with cardiac dysrhythmias and underwent less metabolism and halothane and enflurane; it allowed a more rapid onset of surgical anesthesia and faster awakening compared with the predecessors
|
|
|
What was the problem of isoflurane?
|
It's pungency made it impractical for inhalation induction of anesthesia
|
|
|
Development of sevoflurane and desflurane
|
Sevoflurane and desflurane are halogenated exclusively with fluorine and were first synthesized in the late 1960s and 1970s respectively, but both were expensive and difficult to synthesize and were therefore not immediately considered for commercial use, and it was not until the 1980s that their development was reconsidered in light of new appreciation that a growing proportion of anesthetic practice was taking place in the outpatient setting and that drugs halogenated exclusively with fluorine were less soluble in the blood, allowing faster awakening from anesthesia |
|
|
Blood – gas partition coefficient of inhaled anesthetics
(Isoflurane, enflurane, halothane, desflurane, sevoflurane, nitrous oxide) |
Isoflurane: 1.46 |
|
|
MAC (volumes percent, 30 – 55 years old) of inhaled anesthetics
(Isoflurane, enflurane, halothane, desflurane, sevoflurane, nitrous oxide) |
Isoflurane: 1.15 |
|
|
Vapor pressure (mmHg, 20 C)
(Isoflurane, enflurane, halothane, desflurane, sevoflurane, nitrous oxide) |
Isoflurane: 240 |
|
|
Stable in hydrated carbon dioxide absorbent?
(Isoflurane, enflurane, halothane, desflurane, sevoflurane, nitrous oxide) |
Isoflurane: yes |
|
|
Stable in desiccant carbon dioxide absorbent?
(Isoflurane, enflurane, halothane, desflurane, sevoflurane, nitrous oxide) |
Isoflurane: no, carbon monoxide formation |
|
|
Compound A formation?
(Isoflurane, enflurane, halothane, desflurane, sevoflurane, nitrous oxide) |
Isoflurane: no |
|
|
Amount metabolized (%)
(Isoflurane, enflurane, halothane, desflurane, sevoflurane, nitrous oxide) |
Isoflurane: zero – 0.2 |
|
|
Definition of anesthetic state
|
Although inhaled anesthetics have been used to provide anesthesia for over 160 years, there is no single accepted definition of what constitutes the anesthetics they, for our purposes an operational definition of immobility in response to surgical stimulation and amnesia for intraoperative prevents has proved useful |
|
|
What are the measurable and universal characteristics of all inhaled anesthetics?
|
Include production of immobility and amnestic effects
|
|
|
How is immobility measured?
|
By the minimum alveolar concentration, MAC
|
|
|
MAC
|
The minimum alveolar concentration of anesthetic required to suppress movement to a surgical incision in 50% of patients
|
|
|
What other factors are part of the anesthetic state?
|
Unconsciousness and analgesia
|
|
|
Measuring Unconsciousness
|
Unconsciousness as part of the anesthetic state of it is impossible to measure in an immobile patient who does not remember events from surgery
|
|
|
Analgesia measurement
|
Analgesia was once said to be part of the anesthetic state, but it also cannot be measured in an immobile patient cannot remember
|
|
|
Inhaled anesthetics and pain
|
Surrogate measures of pain, i.e. increased heart rate or systemic blood pressure, suggest that inhaled anesthetics do not suppress the perception of painful stimuli
|
|
|
What else is unique about inhaled anesthetics and pain?
|
Some inhaled anesthetics have hyperalgesic (pain enhancing) effects at low concentrations
|
|
|
What is another common central effects of inhaled anesthetics, and what is the exception?
|
Skeletal muscle relaxation, with the exception being nitrous oxide which increases skeletal muscle tone
|
|
|
Inhaled anesthetics and immobility
|
Inhaled anesthetics produce immobility in large part by their actions on the spinal cord, as evidenced by determination of MAC in decerebrate animals
|
|
|
Structures that regulate the amnestic effects of inhaled anesthetics |
Supraspinal structures such as the amygdala, hippocampus, and cortex are considered highly probable targets for the amnestic effects of anesthetics |
|
|
Central nervous system depression by inhaled anesthetics mechanism
|
Inhaled anesthetics produce anesthesia by enhancing the function of inhibitory ion channels and by blocking the function of excitatory ion channels: enhancing the function of inhibitory ion channels leads to hyperpolarization of the neuron, hyperpolarization results when chloride anions enter neurons through y-aminobutyric acid A receptors (GABAA) or glycine receptors, or when there is an efflux of potassium cations out of neurons through potassium ion channels |
|
|
The biophysical mechanism of interaction between inhaled anesthetics and ion channels
|
Is not well understood, but could prove crucial to how inhaled anesthetic works and help in the design of new inhaled anesthetics; it is thought that inhaled anesthetics exert their effects on IM channels by binding directly to the channels as ligands binding to a receptor, however a minority view holds that they act indirectly by altering the physical property of the membrane and in doing so stabilize open or closed states of ion channels |
|
|
Factors that increase MAC
|
Drugs
age electrolytes red hair |
|
|
Drugs that increase MAC |
Amphetamines(acute use) |
|
|
When is MAC at its highest in terms of age? |
Highest at six months of age |
|
|
Electrolyte abnormalities that increase MAC
|
Hypernatremia, and hyperthermia
|
|
|
Factors that decrease MAC
|
Drugs, age, a letter late disturbances, anemia, hypercarbia, hypothermia, hypoxia, and pregnancy
|
|
|
Drugs that decrease MAC
|
Propofol, etomidate, barbiturates, benzodiazepines, ketamine, A two – agonists (clonidine,dexmedetomidine), ethanol (acute use), local anesthetics, opioids, amphetamines (chronic use), lithium, verapamil
|
|
|
At what age does MAC decrease |
In elderly patients
|
|
|
Electrolyte disturbances that decrease MAC
|
Hyponatremia
|
|
|
What structural characteristic to all modern inhaled anesthetics share and what is the exception?
|
All are halogenated hydrocarbons, with the exception of nitrous oxide |
|
|
How do isoflurane and desflurane differ from each other?
|
They differ only by the substitution of one chlorine atom or fluorine on isoflurane
|
|
|
Physical state of inhaled anesthetics at ambient temperature
|
Nitrous oxide exists as a gas at ambient temperature, although will become a liquid at higher pressures; the remaining inhaled anesthetics are liquids at ambient temperatures
|
|
|
How are halothane, sevoflurane, and isoflurane delivered?
|
By variable – bypass vaporizers
|
|
|
Variable – bypass vaporizer
|
Contains two streams of in flowing fresh gas, one contacting a reservoir (sump), of liquid anesthetic and the other by passing the reservoir; concentration of anesthetic in the gas leaving the vaporizer is determined by the relative flow of fresh gas through the reservoir channel versus the bypass channel, and control of concentration occurs by adjustment of the dial on the vaporizer |
|
|
Why is each variable – bypass vaporizer calibrated specifically for an individual anesthetic?
|
Because each anesthetics vapor pressure differs
|
|
|
How is desflurane administered?
|
By a heated vaporizer
|
|
|
Why is desflurane administered by heated vaporizer?
|
Because the vapor pressure of desflurane at sea level is 700 mmHg at 20°C (near boiling state at room temperature), and delivery by a variable – bypass vaporizer can produce unpredictable concentrations, for this reason the specifically designed vaporizer that heats desflurane cast 2 atm of pressure is used to accurately meter and deliver desflurane vapor corresponding to adjustments of concentration dial by the anesthesiologist |
|
|
Alternate way of administering desflurane
|
There is a variable – bypass vaporizer that delivers desflurane in which gas flow is controlled through the sump and the bypass
|
|
|
What happens with an aesthetic degradation by metabolism or by an interaction with carbon dioxide absorbents (especially when desiccated)? |
It can produce several potentially toxic compounds
|
|
|
Methoxyflurane metabolism |
Methoxyflurane produces inorganic fluoride, which is responsible for the sporadic incidents of nephrotoxicity, i.e. high output renal failure, after prolonged use
|
|
|
What is produced from the breakdown of sevoflurane?
|
Compound A (i.e.trifluoroethyl vinyl ether)
|
|
|
What other inhaled anesthetic produces compound a? |
Halothane produces a similar compound
|
|
|
What are the compounds produced by sevoflurane and halothane shown to do?
|
Have been shown to be nephrotoxic and animals after prolonged exposure
|
|
|
What are the recommendations for sevoflurane administration?
|
In humans prolonged anesthesia with sevoflurane and low fresh gas flows, 1 L/minute, resultant compound a exposure adequate to produce transient proteinuria, enzymuria, and glycosuria, but there is no evidence of increased serum creatinine or long – term effects on renal function; nevertheless the package insert for sevoflurane recommends low fresh gas flow, i.e. less than 2 L per minute, be restricted to less than 2 MAC hours (i.e. MAC concentration times duration of anesthesia) |
|
|
What variables influence the amount of volatile anesthetic degradation on exposure to carbon dioxide absorbants in the clinical relevance? |
The condition, i.e. hydration and temperature, and chemical makeup of the absorbent, fresh gas flow rates, minute ventilation, and most importantly the anesthetic itself |
|
|
Effect of temperature and hydration of carbon dioxide absorbent
|
Although desflurane and isoflurane are very stable in hydrated carbon dioxide absorbent up to temperatures of more than 60°C, full desiccation of conventional carbon dioxide absorbent containing sodium and potassium hydroxide causes degradation and carbon monoxide production from these volatile anesthetics at all temperatures |
|
|
Effect of fresh gas flow rates |
Hi fresh gas flow rates, especially those exceeding normal minute ventilation, accelerate the desiccation of absorbent in the desiccation leads to accelerated degradation, and because degradation is an exothermic process the temperature of the absorbent may increase dramatically
|
|
|
Consequences of the exothermic reaction
|
The exothermic reaction that results from interaction of desiccated carbon dioxide absorbent and volatile anesthetics, especially sevoflurane, can produce extremely high temperatures inside the absorbent canister, which may lead to explosion and fire in the canister or anesthetics circuit
|
|
|
How can the remote risk of fire and explosion from exothermic reactions be avoided?
|
By employing measures that ensure maintenance of adequate hydration in the carbon dioxide absorbent, (i.e. changing the absorbent regularly, turning fresh gas flow down more often unattended anesthesia machines, limiting fresh gas flow rates during anesthesia, and when in doubt about hydration of the absorbent changing it)
|
|
|
How is the relative potency between inhaled anesthetics compared? |
By the MAC, the dose required to suppress movement in 50% of patients in response to surgical incision |
|
|
What percentage of patients should not move in response to incision at a MAC of 1.2?
|
95%
|
|
|
What percentage should not move in response to an MAC of 1.3? |
99%
|
|
|
Is Mac affected by gender or duration of surgery?
|
No
|
|
|
What is remarkable about the MAC values of different anesthetics when put together? |
That they are additive, for example 0.5 MAC of nitrous oxide administered 0.5 MAC of isoflurane has the same effect as one MAC of any inhaled agent in preventing movement in response to incision
|
|
|
What can be said that the anesthetic level at the brain which is needed to prevent movement in response to a surgical incision? |
It is likely to be greater than the MAC, again reflecting the inhibition of reflex responses at the spinal cord level |
|
|
What do the pharmacokinetics of inhaled anesthetics described?
|
Their uptake (absorption) from alveoli into the systemic circulation, distribution in the body, and eventual elimination by the lungs or metabolism principally in the liver
|
|
|
Ultimate goal of delivery of inhaled anesthetics
|
By controlling the inspired partial pressure (PI) (same as the concentration[%] when referring to the gas phase) of an inhaled anesthetic, a gradient is created such that the anesthetic is delivered from the anesthetic machine to its site of action, the brain, so the primary objective of inhaled anesthesia is to achieve a constant and optimal brain partial pressure (Pbr) of anesthetic |
|
|
Equilibration of the brain and other tissue partial pressures |
The brain and all other tissues equilibrate with the partial pressure of the inhaled anesthetic delivered to them by the arterial blood (Pa), and likewise the blood equilibrate the alveolar partial pressure (PA) |
|
|
What then is the useful but indirect method of controlling the brain partial pressure? |
Maintaining a constant and optimal PA, since the PA of inhaled anesthetics mirrors its Pbr and is the reason the PA is used as an index of anesthetic depth, our reflection of the rate of induction and recovery from anesthesia, and a measure of equal potency |
|
|
what determines the alveolar partial pressure and ultimately the brain partial pressure of an inhaled anesthetic?
|
Input (delivery) into the alveoli minus uptake (loss) of the drug from the alveoli into the pulmonary arterial blood
|
|
|
What factors does input of the inhaled anesthetic depend on?
|
The PI, alveolar ventilation (VA), and characteristics of the anesthetic breathing system
|
|
|
What factors does uptake of the inhaled anesthetic depend on?
|
Solubility, cardiac output, and alveolar – to – venous partial pressure difference (a-vD)
|
|
|
So what are the six factors that act simultaneously to determine the alveolar partial pressure of inhaled anesthetic?
|
1. PI (inhaled anesthetic partial pressure)
2. Alveolar ventilation(VA) 3. Characteristics of the anesthetic breathing machine 4. Solubility 5. Cardiac output 6. Alveolar to Venus partial pressure difference |
|
|
What is necessary during initial administration of an inhaled anesthetic?
|
A high PI
|
|
|
What does the initial high PI do?
|
(I.e. input) offsets the impact of uptake into the blood and accelerates induction of anesthesia as reflected by the rate of increase in the PA
|
|
|
What is this effect called?
|
The concentration effect
|
|
|
the range of concentrations necessary to produce the concentration effect is likely only possible with what drug?
|
nitrous oxide
|
|
|
what is the next step to take as uptake of volatile agent into the blood begins to decrease? |
-this is when you should decrease the PI to match the decreased anesthetic uptake, , which is critical to do if you want to achieve a constant and optimal Pbr, because if the PI was maintained constant with time (constant input) the PA (depth of anesthesia, which also reflects the Pbr) would continue to progressively rise as uptake of the anesthetic into the blood drops
|
|
|
second gas effect
|
-an effect separate and independent from the concentration effect, this is the ability of the large-volume uptake of one gas (first gas) to accelerate the rate of increase of the PA of the second gas |
|
|
example of second gas effect
|
the initial large volume uptake of nitrous oxide accelerates the uptake of gases such as O2 and volatiles |
|
|
alveolar hyperoxygenation |
-the transient increase of about 10% of PaO2 that occurs with the initial administration of N2O, reflecting the second gas effect |
|
|
explanation of the second gas effect
|
the explanation is likely the increased tracheal inflow of all inhaled gases (ie. both the 1st and 2nd gases) and the concentration of the 2nd gas into a smaller lung volume (concentration effect) due to the high-volume uptake of the first gas
|
|
|
clinical significant of 2nd gas effect
|
even though it is proven, there really isnt any
|
|
|
impact of alveolar ventilation (VA) on input of anesthetic
|
like PI, increasing VA promotes input of inhaled anesthetic to offest uptake into the blood, with the net effect being a more rapid rise of PA and induction of anesthesia
|
|
|
what effect will hypoventilation have?
|
it will predictably have the opposite effect
|
|
|
what does controlled ventilation of the lungs result in, and what does this do to the PA?
|
-it results in hyperventilation and decreased venous return, which will accelerate the rate of increase of PA by virtue of the increased input (VA) and decreased uptake (dec CO)
|
|
|
what does all of this result in?
|
the risk of anesthetic overdose
|
|
|
so what should you do when moving from spontaneous to controlled ventilation?
|
decrease the PI of volatile anesthetics to maintain the PI similar to that during spontaneous ventilation
|
|
|
characteristics of the anesthetic breathing system which influence the rate of increase of PA
|
-the volume of the system
-the solubility of the anesthetic gases in the rubber/plastic components of the system -gas inflow from the anesthetic machine |
|
|
effect of the volume of the breathing system
|
the volume of the system acts as a buffer which slows the attainment of the PA
|
|
|
how can this buffer effect be negatied?
|
with high gas inflow from the anesthetic machine
|
|
|
effect of solubility of anesthetic gas in the plastic
|
-initially it will slow the rate at which the PA increases, but at the conclusion of the anesthetic reversal of the partial pressure gradient in the anesthetic breathing system will result in extraction of anesthetic whcih slows the rate at which the PA decreases
|
|
|
how is the solubility of inhaled anesthetics denoted?
|
by partition coefficients
|
|
|
partition coefficients
|
-a distribution ratio which describes how an inhaled anesthetic distributes itself between 2 phases when at equilibrium (when the partial pressures are identical between 2 phases, such as alveoli and blood)
-for example, a blood-gas partition coefficient of 10 means the concentration of agent in the blood is 10 and in the alveolar gas is 1 when the partial pressures in each of them is equal |
|
|
what do partition coefficients depend on?
|
temperature, for example the solubility of a gas in a liquid is increased when temperature is decreased (unless stated assume temp at 37C when partition coefficients are given)
|
|
|
what does high blood solubility for an inhaled agent mean?
|
-the blood should be thought of as a pharmacologically inactive reservoir, the size of which is determined by the solubility of the gas in the blood
-high blood solubility means that a large amount of agent must be dissolved in the blood before equilibrium with the gas phase (agent in the alveoli) is reached |
|
|
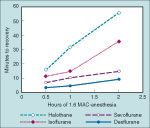
what is true when the blood-gas partition coefficient is high?
|
a large amount of anesthetic must be dissolved in the blood before the Pa equilibrates with the PA, and the rate of induction of anesthesia for an agent is paralleled by the rate of rise of the FA, so the FA will rise slower for agents with high blood-gas partition coefficients, hence things like iso, enf, and halothane are slower than des, sevo, and N2O
|
|
|
what can be done clinically to offset the impact of a high blood solubility on the rate of rise of the PA?
|
increase the PI
|
|
|
low blood solubility
|
-means that minimal amounts of anesthetic have to be dissolved in the blood before equilibrium is reached, so the rate of increase of the PA and hence the Pa and Pbr are rapid
|
|
|
blood-gas partition coefficient for isoflurane
|
1.46
|
|
|
blood-gas partition coefficient for enflurane
|
1.9
|
|
|
blood-gas partition coefficient for halothane
|
2.54
|
|
|
blood-gas partition coefficient for desflurane
|
0.42
|
|
|
blood-gas partition coefficient for sevoflurane
|
0.69
|
|
|
blood-gas partition coefficient for nitrous oxide
|
0.46
|
|
|
tissue-blood partition coefficients
|
determine the time necessary for equilibration of the tissue with the Pa
|
|
|
how is this time predicted?
|
by calculating a time constant (ie. the amount of anestehtic that can be dissolved in the tissue divided by tissue blood flow) for each tissue
|
|
|
what are brain-blood partition coefficients for agents such as isoflurane? the less soluble agents?
|
-for the more soluble agents, such as isoflurane, about 3-4 minutes
-for the less soluble, about 2 minutes |
|
|
how many time constants does complete equilibration with any tissue, including the brain, require?
|
at least 3 times constants
|
|
|
what does this mean for an agent like isoflurane?
|
this is the rationale for maintaining a constant PA for 10-15 minutes before assuming the Pbr is similar to the PA (ie. 3 time constants: 3x 3-4 is about 10-15)
|
|
|
how about for the less soluble agents such as nitrous oxide, des, and sevo?
|
complete equilibrium will be achieved in about 6 minutes (ie. 3 time constants)
|
|
|
importance of the blood-gas partition coefficient for nitrous oxide, and what is it?
|
its 0.46, and the importance is that this blood-gas partition coefficient is 34 times more than the one for nitrogen (which is 0.014), which means that nitrous oxide will leave the blood to enter air-filled cavities 34x faster than nitrogen will leave these cavities and enter the blood, resulting in a preferential trasnfer of N2O, causing the volume or pressure of air-filled cavities to increase
|
|
|
nitrous oxide entry into a cavity with a compliant wall
|
(eg. intestinal gas, pneumothorax, pulmonary blebs, air embolism) will cause the gas space to expand, increasing its volume
|
|
|
nitrous entry into a cavity with a noncompliant wall
|
(eg. the middle ear, cerebral ventricles, supratentorial subdural space) will cause an increase in the pressure of the cavity
|
|
|
what 3 things influence the magnitude of increase of volume or pressure of an air-filled cavity caused by nitrous oxide?
|
-the PA of nitrous
-blood flow to the air-filled cavity -the duration of nitrous administration |
|
|
what is one of the contraindications to using nitrous oxide?
|
the presence of a closed oneumothorax, as its been shown in animal models that nitrous at 75% doubles the volume of a pneumo in 10 minutes
|
|
|
what might be happening if there is decreasing pulmonary compliance in a patient with a history of chest trauma (ie. rib fractures) who is getting nitrous?
|
may reflect nitrous oxide induced expansion of an unrecognized pneumothorax
|
|
|
what other complication can occur with nitrous?
|
air bubbles from a venous air embolus can be caused to expand rapidly
|
|
|
nitrous oxide for bowel surgery
|
-as opposed to the rapid expansion of pneumos and air emboli, the increase in bowel gas volume caused by nitrous is slow
-if an intraabdominal operation is short, using nitrous isnt an issue -if the bowel gas volume is increased, such as during a SBO, it may be prudent to limit the concentration of nitrous to 50%, which would cause bowel gas volume to double at most even during a prolonged operation |
|
|
effect of cardiac output on induction
|
-CO influences agent uptake into the blood and therefore the PA by carrying either more or less anesthetic from the alveoli
|
|
|
what does a high CO do to induction?
|
(eg fear)
-high cardiac output will cause more rapid uptake of the anesthetic, so the rate of increase in the PA and induction of anesthesia are slow |
|
|
low CO?
|
(eg. shock)
-increases the rate of increase of PA because there is less uptake into the blood to oppose input, leading to the common clinical knowledge that induction of patients in shock is rapid |
|
|
effect of a right-to-left shunt or intrapulmonary shunt on induction of anesthesia?
|
will slow the rate of induction, due to the dilutional effects of the shunted blood, which has no anesthetic on board, on the partial pressure of anesthetic in the blood coming from vented alveoli (similar to the effect of a right-to-left shunt on PaO2)
|
|
|
left-to-right shunt
|
(eg. AV fistula, volatile-induced increase in cutaneous blood flow)
-results in venous blood delivered to the lungs that has a higher partial pressure of anesthetic than the blood in the tissue veins -this results in offsetting of the dilutional effect of a right-to-left shunt |
|
|
what needs to be there in order for the effect of a left-to-right shunt on Pa to be detectable?
|
there has to be a concominant right-to-left shunt
|
|
|
what is the effect of wasted ventilation (ventilation of nonperfused alveoli) on the rate of induction?
|
-it really doesnt influence the rate of induction, because a dilutional effect is not produced
-what it does though is produce a difference between the PA and Pa of the inhaled agent (similar to the observed difference between the ETCO2 and the PaCO2) |
|
|
A-VD
|
-alveolar-to-venous partial pressure difference
-reflects the tissue uptake of inhaled agents |
|
|
body tissue compartments and their blood flow
|
vessel-rich group (brain, heart, kidneys, and liver): accounts for only 10% of body mass but gets 75% of CO
muscle group: 50% of mass but 19% CO fat group: 20% mass, gets 5 % CO vessel-poor group: 20% of mass, 1% CO |
|
|
highly perfused tissues and anesthetic
|
-as the brain, heart, kidneys, and liver recieve about 75% of CO, they equilibrate rapidly with the Pa, and as a result after 3 time constants (6-12 minutes for inhaled agents) about 75% of returning venous blood is at the same partial pressure as PA (ie. a narrow A-VD)
|
|
|
consequence of this narrowing of A-VD
|
-the uptake of anesthetics from the alveoli is greatly decreased after 6-12 min, which is reflected by the narrowing PI-to-PA difference
-and after this amount of time the concentration of inhaled anesthetics should be decreased in order to maintain a constant PA (as there is dec uptake, if the concentration remains high the PA will simply rise) |
|
|
skeletal muscle and fat and anesthetics
|
-as stated, make up around 70% of body mass, but only recieve <25% CO
-they will continue to act as inactive reservoirs of anesthetic for several hours -equilibration of fat with inhaled anesthetics in blood probably neve roccurs |
|
|
how can recovery of anesthesia be defined?
|
as the rate at which the PA decreases with time
|
|
|
elimination of inhaled anesthetics
|

-elimination of inhaled anesthetics is reflected by the decrease in the alveolar concentration (FA) compared with the concentration present at the conclusion of anesthesia (FAO)
-awakening from anesthesia is paralleled by these curves |
|
|
in what ways does recovery from anesthesia differ from induction of anesthesia?
|
-the absence of a concentration effect during recovery (the PI cant be less than 0)
-the variable tissue concentrations of anesthetics which will exist at the beginning of recovery -the potential importance of metabolism on the rate of decrease in the PA |
|
|
tissue concentration impact on recovery from anesthesia
|
-tissue stores of agent serve as a reservoir to maintain PA when the partial pressure gradient is reversed by decreasing the PI to 0 at the end of anesthesia
|
|
|
what does the impact of tissue stores of agent depend on?
|
the duration of anesthesia, and the solubility of the agent in the various tissues
|
|
|
when is and when isnt the duration of anesthesia impactful on recovery?
|
-time to recovery will be prolonged in proportion to the duration of anesthesia for soluble agents, such as iso, but the impact of duration with the less soluble agents (des, sevo) is minimal
|
|
|
what is an important difference between induction of anesthesia and recovery?
|
the potential impact of metabolism of inhaled agents on recovery
|
|
|
for which agent is metabolism the principal determinant of the rate of decrease in the PA?
|
for the lipid soluble methoxyflurane
|
|
|
for which is metabolism and the VA equally important?
|
halothane
|
|
|
for which is VA the principle determinant of the rate of decrease of the PA?
|
the less lipid soluble agents, such as isoflurane, desflurane, and sevoflurane
|
|
|
so in conclusion, what 2 things do the pharmacokinetics of the elimination of inhaled anesthetics depend on?
|
the length of administration, and the blood gas solubility of the inhaled agent
|
|
|
context sensitive half-times for the inhaled anesthetics
|
can be calculated based on computer simulations, as with the IV agents
|
|
|
time needed for a 50% decrease in anesthetic concentration for iso, sevo, and des
|
-is less than 5 minutes for all, and does not increas esignificantly with increasing time of anesthesia
-presumably reflects the initial phase of elimination, which is dependent of primarily VA |
|
|
what does determination of other decrement times, such as 80% and 90% decreases of anesthetic concentrations, reveal
|
differences between various inhaled anesthetics
|
|
|
80% decrement times
|
-are less than 8 minutes for des and sevo, and do not increase with increasing time of anesthetic
-whereas for iso it increases significantly after 60 minutes of administration, reaching a plateau of about 30-35 minutes |
|
|
90% decrement times
|
-for desflurane increases slightly from 5 minutes after 30 min of administration, to 14 after 6 hours, which is still way less than for sevo after this amount of time (65 min) and iso (86 min)
|
|
|
so when does the principle difference in the rates of elimination between iso, sevo, and des occur?
|
in the final 20% of the elimination process
|
|
|
diffusion hypoxia
|
-can occur after nitrous is shut off if patients are allowed to breath room air, as the initial outpouring of N2O from blood into alveoli can dilute the PaO2 enough that it decreases
|
|
|
how can diffusion hypoxia be prevented?
|
by filling the patient's lungs with oxygen at the end of nitrous administration
|
|
|
circulatory effects of the inhaled anesthetics
|
-data from healthy volunteers who got equipotent doses of agents showed there was no difference in the circulatory effects of these drugs, especially during maintenance of anesthesia
-it should be noted, however, that patients undergoing surgery may respond differently than healthy volunteers |
|
|
proposed mechanisms for the circulatory effects of inhaled anesthetics
|
-direct myocardial depression
-inhibition of CNS and sympathetic outflow -depression of transmission of impulses through autonomic ganglia -attenuated carotid sinus reflex activity -decreased formation of cyclic adenosine monophosphate -inhibition of calcium reuptake by myocardial sarcoplasmic reticulum -dec influx of Ca ions through slow channels |
|
|
effects of inhaled agents on MAP
|

MAP decreases in a dose-dependent manner with increasing MAC of all inhaled agents
|
|
|
what is the main reason for this decrease in MAP, and what is the exception?
|
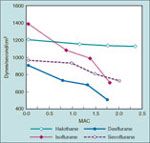
-the decrease in MAP primarily reflects a decrease in SVR vs. a dec in CO, with the exception being halothane, which lowers MAP almost entirely by decreasing CO, with SVR being relatively unchanged
|
|
|
inhaled anesthetics effect on CO
|

|
|
|
how can this dose-related decrease in SVR be minimized?
|
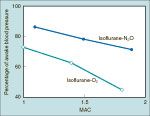
by substituting NO for a portion of the volatile drug, because nitrous in contrast to the other inhaled agents causes no change or a slight increase in MAP when given alone to volunteers
|
|
|
effect of inhaled agents on heart rate
|

-stepwise increases in the agents causes an increase in heart rate, though at different concentrations for each agent
|
|
|
isoflurane and heart rate
|
at concentrations as low as 0.25 MAC, starts to cause a linear increase in heart rate
|
|
|
decflurane and HR
|
-heart rate increases minimally with a concentration less than 1 MAC
-but at higher concentrations, the heart rate increases in a linear, dose-dependent manner |
|
|
sevoflurane and heart rate
|
-in contrast to iso and des, the heart rate doesnt start to increase until concentration exceeds 1.5 MAC
-although, induction with 1% sevo has been associated with tachycardia in kids and adults |
|
|
what is this tachycardia thought to be due to?
|
-may be due to sympathetic nervous system stimulation associated with epileptiform brain activity
|
|
|
what happens for the tendency of desflurane to stimulate the circulation? (ie. increase MAP and HR)
|
it wanes during maintenance of anesthesia
|
|
|
halothane effect on heart rate
|
-does not effect heart rate likely due to inhibition of the baroreceptor reflex (although iso, sevo, and des also diminish the baroreceptor response)
|
|
|
what is the increase in HR with desflurane concentrations above 1 MAC due to, and is it attenuated by nitrous oxide?
|
-due to sympathetic nervous system stimulation, rather than reflex baroreceptor response
-it is NOT attenuated by mixing in nitrous oxide |
|
|
inhaled anesthetics effect on cardiac index
|

-the effect of iso, sevo, and des is minimal
-TEE actually shows des produces minor increases in EF and LV velocity of circumferential shortening compared to awake measurements |
|
|
effect of abrupt increases in cncentration of inhaled agents on the CV system
|

-an abrupt increase in desflurane at concentration above 1 MAC causes a transient circulatory stimulation in the absence of opioids, adrenergic blockers, etc
-isoflurane can to a lesser extent also increase HR and BP |
|
|
what is seen with this circulatory stimulation?
|
-an increase in plasma epi and norepi concentrations, and in sympathetic nervous system activity
|
|
|
what is seenw ith an abrupt increase in sevoflurane from 1 MAC to 1.5 MAC?
|
a slight decrease in HR
|
|
|
a stepwise increase in end-tidal decflurane from 4% to 8% within 1 minute
|
-can result in the doubling of heart rate and blood pressure from baseline
-though giving opiates, clonidine, or esmolol can profoundly attenuate the HR and BP responses |
|
|
what happens if the rapid increase of end-tidal des from 4% to 8% is repeated again 30 minutes later?
|
-results in minimal changes to heart rate and blood pressure, suggesting the receptors which mediates these responses adapt to repeated stimulation
|
|
|
ciculatory effects seen with rapid increases in sevo, halothane, or enflurane concentration
|
none are seen
|
|
|
which inhaled agents are used for their lack of pungency?
|
sevo and halothane
|
|
|
what does induction with halothane in children do, in comparison to sevo?
|
-halothane causes depression of myocardial activity, while sevo does not
|
|
|
what happens with maintenance of anesthesia in adults with 1 MAC of sevo or halothane in 67% nitrous oxide?
|
both will decrease myocardial contractility
|
|
|
comparison of giving inhaled agents with nitrous oxide-oxygen vs. oxygen alone
|
-basically the decrease in MAP, SVR, cardiac index, and LV stroke work index and inc in HR, pulmonary artery pressure, and CVP are the same with each, except that they are all more pronounced with desflurane in oxygen rather than with nitrous oxide
|
|
|
which inhaled anesthetic sensitizes the myocardium to premature ventricular extrasystoles?
|
-halothane does, especially in the presence of catecholamines
-iso, sevo, and des do not seem to do this |
|
|
what does animal study evidence suggest is the reason inhaled anesthetics suppress ventricular dysrhythmias related to myocardial ischemia?
|
prolongation of the effective refratory period
|
|
|
inhaled agent effect on incidence of bradycardia
|
-the choice of agent will affect the incidence of bradycardias associated with vagal stimulation, for example children given sevo have less bradycardia and sinus arrest during traction of the ocular muscles than with halothane
|
|
|
what are all inhaled agents known to do to the EKG?
|
prolong the QT interval (although the degree to which each agent does this has not been compared)
|
|
|
which anesthetic should be avoided in pts with congenital long QT syndrome?
|
sevoflurane
|
|
|
propofol, sevoflurane and the QT interval
|
-while both prolong the QT interval, neither causes increased transmural dispersion of repolarization, which is a measure of heterogenous rates of repolarization of myocardial cells during phase 2 and 3 of the action potential
|
|
|
so what is the clinical significance of prolonged QT in pts?
|
unclear
|
|
|
what is the mainstay of therapy for patients with LQTS?
|
B-blockers; all modern inhaled agents have been shown to be safe with B-blockade
|
|
|
which agent has been shown to produce numerous intraop malignant arrhythmias in patients not being B-blocked?
|
halothane, and all of these have been attributed to undiagnosed LQTS
|
|
|
anesthesia for patients with CAD
|
multiple studies of patients having a CABG or at risk of CAD have failed to show any difference between inhaled vs. IV anesthesia, or between the inhaled agents compared to the others
|
|
|
concern with isoflurane and CAD
|
-there was a concern that because iso dilates small-diameter coronary arteries it may cause coronary steal, and cause pts with susceptible anatomy to develop regional myocardial ischemia as the result of coronary vasodilation, but these concerns turned out to be invalid
|
|
|
what is the effect of volatile anesthetics on the heart?
|
they have a protective effect, limiting the area of myocardial injury and preserving function after exposure of the heart to ischemic insult
|
|
|
what is the protective effect of inhaled agents on the myocardium called?
|
anesthetic preconditioning
|
|
|
how is this explained?
|
-it is NOT explained by a favorable alteration of myocardial oxygen supply-demand ratio, as evidence suggests the inhaled agents exert a protective effect on the myocardium in the setting of decreased regional perfusion
|
|
|
agents and CABG vs. propofol
|
-maintenance with 0.2-1 MAC of des or sevo compared to propofol showed less incidence of abnormally elevated troponins
-also, sevo given for the entire duration of CABG vs. only during pre and post bypass showed lower rates of post-op MI, and sevo given only pre and postbypass vs. propofol for these showed lower risk of MI as well |
|
|
ischemic preconditioning
|
-a fundamental protective mechanism that is seen in all tissues in all species
-exposure of tissues to single or multiple brief episodes of ischemia confers a protective effect on that tissue against reversible or irreversible injury to subsequent prolonged ischemia |
|
|
periods of ischemic preconditioning in the myocardium
|
there are 2 distinct periods when the myocardium is protected after a brief ischemic insult:
1. 1-2 hours after the episode, then it dissipates 2. the benefit reappears 24 hours later, and can last 3 days |
|
|
what is the mechanism of this protection?
|
the opening of mitochondrial ATP sensitive K+ channels confers the protection, resulting from the binding of various ligands to G protein-coupled receptors; this is thought to play the role in the protection conferred by volatile agents
|
|
|
inhaled anesthetics effect on breathing
|
-increase the frequency, with smaller tidals volumes
-minute ventilation is preserved, but the dec tidal volumes causes a greater proportion of deadspace ventilation to alveolar ventilation |
|
|
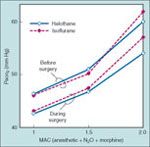
agents effect on PaCO2
|

-gas exchange becomes progressively less efficient as depth of anesthesia increases, and PaCO2 increases proportionally to depth
|
|
|
what can be done to attenuate the increase in PaCO2 at deeper levels of anesthesia?
|
substitute nitrous oxide (60%) for an equivalent portion of volatile agent
|
|
|
other effect shown on breathing with volatile agents
|

-agents produce a dose-related blunting of CO2 responsiveness, leading to apnea in subjects recieving 1.7 MAC of des
|
|
|
what has been shown to decrease the blunting of ventilation with inhaled anesthetics?
|
-it is blunted in patients having surgery vs. those healthy subjects in studies, showing the stimulation of surgery on breathing
|
|
|
what other ventilatory stimulating effect do all volatile agents blunt?
|
the stimulating effect of arterial hypoxemia
|
|
|
changes to the chest wall caused by inhaled agents
|
-cause cephalad movement of the diaphragm, and inward displacement of the rib cage due to enhanced expiratory muscle use, leading to a decrease in FRC
-atelectasis will occur in the dependent lung portions, to a greater extent when spontaneous ventilation is permitted |
|
|
effect of inhaled anesthetics on hypoxic pulmonary vasoconstriction
|
they dont effect it
|
|
|
effect of inhaled agents on airway resistance
|
-in the absence of bronchoconstriction, cause only minimal bronchodilation, but have been shown to decrease respiratory systemic resistance after intubation
|
|
|
airway irritant effects of inhaled anesthetics
|
differ, ranging from pungent to nonpungent
|
|
|
nonpungent agents
|
-sevoflurane, halothane, and nitrous oxide are nonpungent and cause minimal or no irritation over a broad range of concentrations
-these are the agents chosen when inhalational induction is desired |
|
|
pungent agents
|
-isoflurane and desflurane are pungent and can irritate the airways at concentrations >1 MAC, esp in the absence of drugs that can blunt this such as opiates or sedative-hypnotics
-even though they are irritating, the reason they can safely be given through an LMA is that it generally takes less than 1 MAC for maintenance with an LMA (ie. nonirritating concentrations) |
|
|
signs of airway irritations
|
-coughing
-breath holding -laryngospasm -arterial oxygen desaturation |
|
|
what are the CNS effects of giving nitrous oxide without volatile agents?
|
-causes cerebral vasodilation and increases cerebral blood flow
-the cerebral metabolic rate for oxygen (CMRO2) increases slightly |
|
|
how can these effects be counteracted?
|
by concurrently giving opioids, barbiturates, or propofol (but not ketamine)
|
|
|
effect of inhaled agents on cerebral vascular responsiveness to changes in PaCO2
|
they do NOT abolish the responsiveness
|
|
|
effects of the volatile agents on CNS
|
-halothane, iso, des, and sevo all decrease CMRO2 |
|
|
CBF increase for the agents compared
|
the increase in CBF is greater with halothane than with iso/sevo/des
|
|
|
effects of volatile agents on ICP
|
-ICP increases with all volatile agents at >1 MAC
-in addition, the autoregulation, ie. adaptive mechanism normalizing cerebral blood flow over a wide range of arterial BPs, is impaired at concentrations <1 MAC |
|
|
patients undergoing supratentroial craniotomy who recieve 1 MAC of iso or des
|
-show a decrease in cerebral perfusion pressure, and an arterial-venous oxygen difference
-but, showed no change in ICP |
|
|
patients having pituitary tumor resection who get 1 MAC of des, iso, sevo
|
show small increases in ICP and decrease in CBF
|
|
|
nitrous oxide and ICP
|
-50% N2O with 0.5 MAC of iso/des showed better relaxation than those getting 1 MAC iso/des
|
|
|
what do inhaled anesthetics do to cerebral responsiveness to changes in PaCO2?
|
do not change it
|
|
|
inhaled agents and nitrous effect on evoked potentials
|
-all agents and N2O depress the amplitude and increase the latency of somatosensory evoked potentials in a dose-dependent manner
-potentials may be abolished at 1 MAC of agents, or 0.5 MAC and 50% N2O |
|
|
what about low concentrations of agent on evoked potentials?
|
0.2 to 0.3 MAC do decrease the reliability of motor evoked potential monitoring
|
|
|
EEG changes due to volatile agents
|
-increasing depth of anesthesia causes increased amplitude and synchrony
-as depth increases, start to see periods of electrical silence taking up a greater proportion of the time (burst suppression) |
|
|
when does the isoelectric pattern dominate the EEG?
|
from 1.5 to 2 MAC
|
|
|
what can sevoflurane (and enflurane) be associated with on EEG?
|
-epileptiform activity, especially at higher doses or when controlled hyperventilation is instituted
-siezure like activity has even been seen in children during sevoflurane induction |
|
|
neuromuscular effects of volatile agents
|
-produce dose-related skeletal muscle relaxation and enhance the activity of succ and NDMBs
|
|
|
which of the volatile anesthetics has an enhancing effect on neuromuscular blockers, and has a greater effect on their reversal when turned down?
|
desflurane
|
|
|
inhaled agents and malignant hyperthermia
|
-of course all have the ability to cause MH, but studies show des, and possibly sevo and iso have a lower risk than halothane
|
|
|
categorization of hepatic injury after anesthesia
|
can be classified as:
-severe (immune mediated) -mild |
|
|
severe liver injury following anesthesia
|
-can occur with halothane, sevo, iso, or des, and involves massive necrosis of the liver that can cause need for transplant or death, and whose mechanism is immunologic, and requires prior volatile agent exposure
|
|
|
mechansism of hepatic injury by inhaled agents
|
-halothane, iso, and des all undergo hepatic metabolism by the cytochrome P450 enzymes to produce trifluoroacetate, which can covalently bind to hepatocyte proteins, forming TFA-hepatocyte moities which act as haptens and get recognized as foreign by the body, so antibodies to them are formed; then on subsequent exposure to a TFA forming anesthetic an immune response can be provoked, leading to hepatic necrosis
|
|
|
sevoflurane and liver injury
|
even though sevo is not metabolized to TFA, it can undergo degredation on contact with CO2 absorbers to compound A, which may act in a manner analogous to TFA and provoke an immulogic response
|
|
|
mild liver injury secondary to inhlaed agents
|
-occurs after giving halothane, is mainly characterized by a modest elevation of serum transaminases, and is thought to mediated by reductive metabolism of halothane
-the likelyhood is increase dwhen there is also a decrease in hepatic blood flow and hence reduced oxygen delivery to the liver |
|
|
so what should be done in terms of the anesthetic in patients with a hepatic history?
|
-should probably avoid inhaled anesthetics in those who have had hepatic injury following anesthesia before, but no need to in patients with preexisting hepatic disease unrelated to anesthetics
|